Pretibial lymphoplasmacytic plaque
Pretibial lymphoplasmacytic plaque
Clinical features Pretibial lymphoplasmacytic plaque first described as isolated benign primary cutaneous plasmacytosis is a variant of pseudolymphoma that characteristically occurs in children and adolescents with marked predilection for the pretibial area.1,2 Most cases described so far have been in Caucasians. Presentation is as a solitary, red-brown, long-standing (often years) scaly, erythematous plaque varying in size from less than 1 to 4 cm.1–6 Papular lesions may also be seen. The behavior is benign, but treatment is difficult.
Pathogenesis and histologic features The etiology of the process is unknown. The epidermis displays acanthosis and hyperkeratosis with focal parakeratosis. In the underlying superficial and deep dermis, there is a moderate to prominent perivascular and periadnexal mononuclear cell infiltrate composed of lymphocytes and numerous mature plasma cells.1–6 In some cases, focal interface inflammation of the epidermis and sweat glands is seen. Occasional epithelioid cell granulomas are rarely identified.
Differential diagnosis Primary cutaneous plasmacytosis is characterized clinically by multiple plaques with predilection for the trunk, occurs almost exclusively in Asians, and consists histologically of an infiltrate composed almost exclusively of mature polytypic plasma cells. Acral pseudolymphomatous angiokeratoma of children (APACHE) consists of warty papular lesions, usually on acral sites, and it is characterized histologically by more prominent epidermal changes and a dermal predominantly lymphocytic infiltrate with few plasma cells and a prominent proliferation of small vascular channels. T cell-rich angiomatous polypoid pseudolymphoma (TRAPP) presents as a single polypoid lesion, with predilection for adults and consists of a prominent dermal infiltrate composed of T lymphocytes with few plasma or no plasma cells and numerous small blood vessels.
prominent eosinophils. Kimura disease is morphologically similar, but clinically most patients are Asian and there is peripheral blood eosinophilia and raised serum IgE.
Lesions with prominent spindle cells are more likely to be confused with other spindled cell tumors, with differential diagnosis including solitary fibrous tumor, FDC sarcoma, and nodular fasciitis.
Differentiation from IgG4-RD requires close clinicopathological correlation and application of agreed diagnostic criteria.19
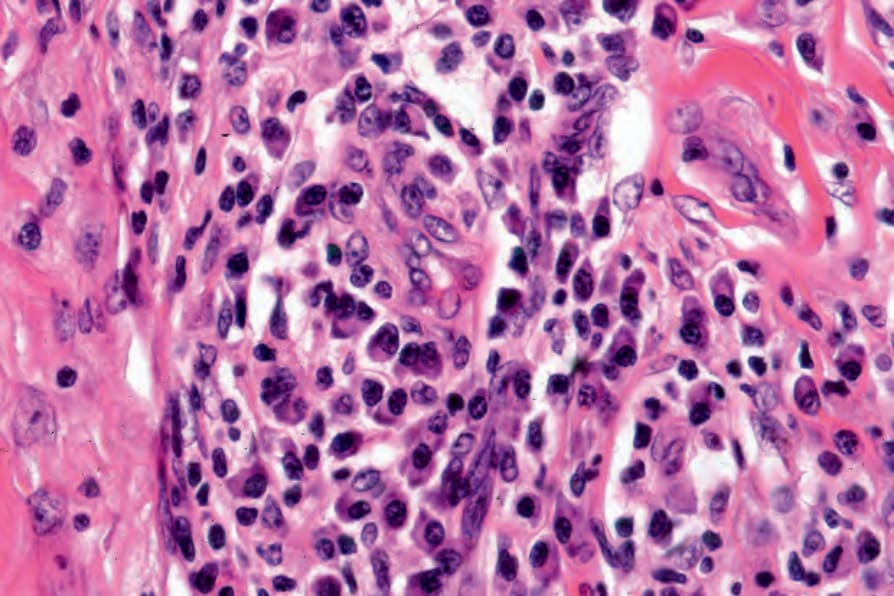
Fig. 29.267 Inflammatory pseudotumor of the skin: the infiltrate consists of lymphocytes and conspicuous plasma cells.