Cutaneous post-transplant lymphoproliferative disorders
Cutaneous post-transplant lymphoproliferative disorders
Clinical features Post-transplant lymphoproliferative disorders (PTLDs) are defined by the WHO as lymphoid or plasmacytic proliferations secondary to immunosuppression in patients with solid organ, bone marrow, or stem cell allograft transplant.1 The spectrum of PTLD is very wide and includes polyclonal and monoclonal B cell (usually, but not always, EBV driven) and T-cell proliferations. The incidence of PTLD is around 2%, and the prognosis is variable with survival of between 50% and 80%.2 Presentation is usually early in lesions driven by EBV and late in those not driven by the virus. The incidence of PTLD is higher in children, in those that are seronegative for EBV at the time of transplantation, and in patients with heart–lung, lung, or gastrointestinal transplants.1 Renal transplant patients have a lower incidence of PTLD. Extranodal involvement is common, particularly in the lungs, gastrointestinal tract, CNS, and even the transplanted organ. Cutaneous involvement by PTDL is very rare with no more than 30 cases reported in the literature.2–20 It is usually restricted to the skin, and may affect children and adults, with no sex predilection. Presentation is with single or multiple papules, nodules, or plaques that may involve the limbs, trunk,
EBV+ MCU is a localized, circumscribed process typically contained by a peripheral rim of small T cells. It does not form a mass lesion.38
Methotrexate and other non-transplant iatrogenic-associated lymphoproliferative disorders
Clinical features Methotrexate-associated lymphoproliferative disorder (MALD) was defined by the WHO in 2001 as a lymphoid proliferation or lymphoma in patients undergoing immunosuppressant treatment with methotrexate, mainly those with rheumatoid arthritis, psoriasis, and dermatomyositis, and often with associated EBV infection.1 The lymphoid proliferation may mimic
1481 Epstein-Barr virus-positive mucocutaneous ulcer
or face. Patients with cutaneous disease tend to have good prognosis, and improvement or complete regression is seen with reduction or cessation of immunosuppression.
Pathogenesis and histopathological features As mentioned above, most cases of B-cell proliferations are driven by EBV. The pathogenesis in cases negative for EBV is not clear but may be due to other viruses or chronic antigenic stimulation. Histologically, PTDL have been divided into early lesions (plasmacytic hyperplasia), polymorphic PTDL, and monomorphic PTDL.1 Early lesions of PTDL consist of hyperplasia of plasma cells with mature lymphocytes and occasional immunoblasts. EBV is usually demonstrated and clonality is absent. In polymorphic PTDL, there is a prominent dermal and often subcutaneous infiltrate composed of mature plasma cells, immunoblasts, and small to medium-sized irregular lymphocytes (Figs 29.249–29.253). Some cells may resemble Hodgkin or Reed-Sternberg cells.1,20 EBV and a B-cell clone are usually demonstrated. Monomorphic PTDL includes B and T/NK lymphomas that occur in an immunocompetent host, but most indolent B-cell lymphomas, with the exclusion of marginal zone lymphoma, are not included.21,22 Monomorphic T-cell PTDLs are much less common than those of B-cell lineage. Any type of T-cell lymphoma may be seen, and in the skin, mainly anaplastic large T-cell lymphoma has been described.11–16 A T-cell clone is usually demonstrated, but EBV is only exceptionally detected.14
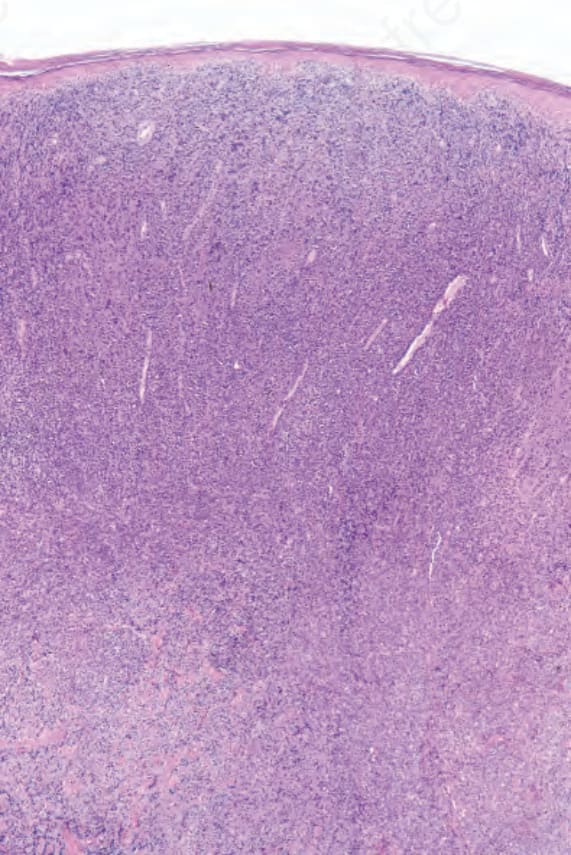
Fig. 29.249 Post-transplantation B-cell lymphoproliferative disorder: this patient developed a large perianal plaque following renal transplantation. The tumor regressed following reduction in immunosuppression.
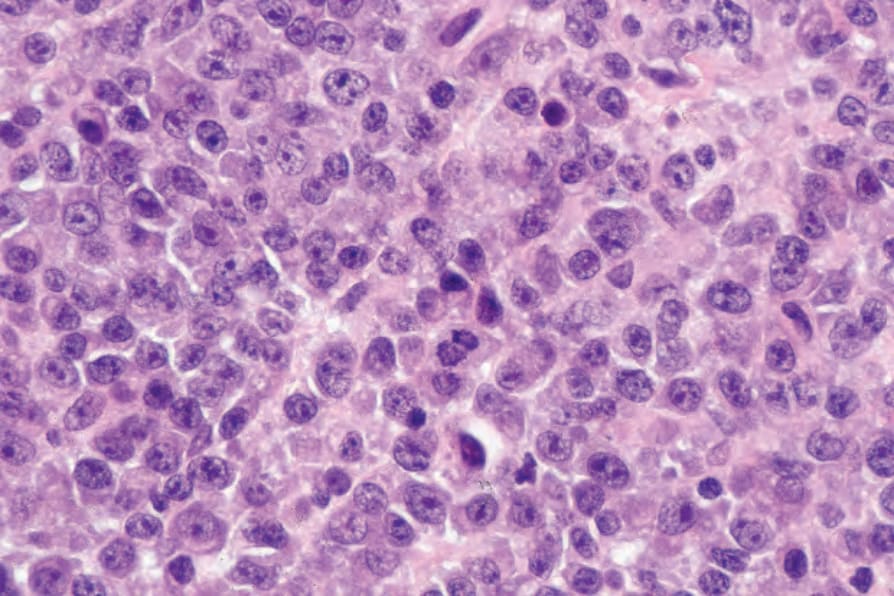
Fig. 29.250 Post-transplantation B-cell lymphoproliferative disorder: high-power view showing plasmacytoid differentiation.
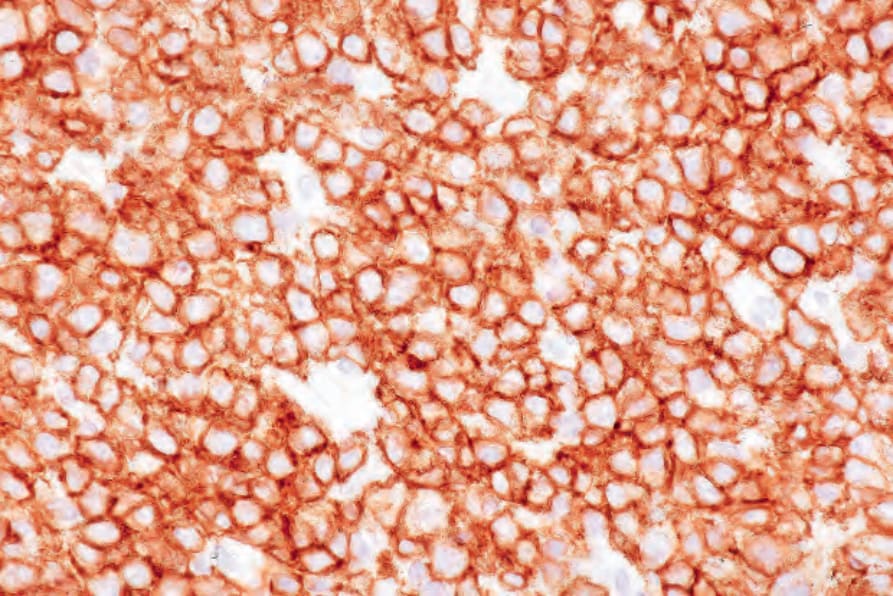
Fig. 29.251 Post-transplantation B-cell lymphoproliferative disorder: the tumor cells express CD138.