Mantle cell lymphoma
Mantle cell lymphoma
Clinical features Mantle cell lymphoma(MCL) (mantle zone lymphoma, centrocytic lymphoma, lymphocytic lymphoma of intermediate grade) is a rare peripheral B-cell lymphoma thought to be derived from naive pregerminal center B cells of the inner mantle zone.1 It accounts for approximately 3–10% of NHL subtypes.2 It is more common in old adults (median, 60 years) with predilection for males (2 : 1–4 : 1).1,3,4
MCL is a nodal disease that frequently disseminates to extranodal sites. Most cases are advanced stage (stage III or IV) at diagnosis. Generalized lymphadenopathy is the most frequent presentation (87–90%). Infiltration of bone marrow (80%), spleen (47–60%), and liver (13%) is frequent. The gastrointestinal tract (18–20%) and Waldeyer ring (10–12%) are also often affected, and most cases of lymphomatous polyposis of the intestine are due to this lymphoma. Neoplastic lymphocytes are typically found in peripheral blood using flow cytometry, and rarely there may be a leukemic picture.5–8 ‘B’ symptoms (clinical symptoms of pyrexia (sometimes periodic), weight loss, and night sweats) are present in 14% to 40% of patients.3,4 Anemia, low serum albumin, raised LDH, and β2-microglobulin levels are common.3,4 Cutaneous involvement is exceptional, and although MCL may present in the skin, it is almost invariably associated with systemic disease.9–13 Presentation is with erythematous nodules or tumors on the trunk or extremities, although indurated plaques, macules, and a maculopapular rash may occur.9–12 It can also be associated with cutaneous paraneoplastic phenomena. Several cases of insect bite-like reactions, similar to those more commonly seen in CLL, have been described. These manifest as a polymorphous rash comprising multiple pruritic, erythematous papules, nodules, plaques, and/or vesicles, that usually precede, but may follow, the diagnosis of lymphoma.14–18 Hypersensitivity reactions to mosquito bites, similar to those seen in association with NK/T-cell lymphomas, have also been described.19,20
Cutaneous lesions vary from superficial perivascular to nodular or diffuse dermal/subcutaneous monomorphic infiltrates (Figs 29.218–29.220).9–12 Small/intermediate and blastoid variants may be encountered.11 Insect
The median survival is only of 3–5 years.1,21 The most consistent prognostic indicators are a high mitotic or Ki-67 index and a blastoid or pleomorphic morphology.1,7,8,22,23 An indolent non-nodal leukemic variant characterized by involvement of peripheral blood, bone marrow, and often spleen is now recognized. Unlike more usual MCL, the neoplastic lymphocytes possess mutated immunoglobulin heavy chain genes and are SOX11 negative.24
Pathogenesis and histopathological features MCL is associated with a t(11;14)(q13;q32) translocation in most cases.1,3,4,25–27 This results in dysregulation of the PRAD1/CCND1 gene with overexpression of cyclin D1, a protein that is critical to cell cycle regulation.28,29 A variant translocation involving CCND1 and light chain genes may also occur.30 Most cases also contain a high number of non-random secondary chromosomal aberrations, some of which correlate with more aggressive behavior.31–33 A subset of MCLs lack t(11;14)(q13;q32) and do not overexpress cyclin D1. These cases show identical morphologic and clinical features as cyclin D1-positive cases and share the same gene expression profile, except that they express high levels of cyclin D2 or cyclin D3. Some have a t(2;12)(p12;p13) juxtaposing the cyclin D2 gene with the immunoglobulin lambda light chain gene.34,35 Immunoglobulin light and heavy chain genes are rearranged in many cases, but the V regions are usually either unmutated or show only low levels of somatic hypermutation.36,37
Nodal tumors may show a nodular, diffuse, or mixed growth pattern.1–3,5,38,39 In nodular variants, the nodules represent reactive follicles
1470 Cutaneous lymphoproliferative diseases and related disorders
breakpoint by PCR suffers from scattering of the breakpoints, and it is much less sensitive.43 The diagnosis may also be confirmed by reverse transcription PCR (RT-PCR) demonstration of cyclin D1 transcript overexpression.43 It should also be remembered that rare cases lack t(11;14). Thus, when confronted with a CD5-positive, cyclin D1-negative lymphoma with the morphological features of MCL, consideration should be given to staining for SOX11, cyclin D2, and/or cyclin D3 to avoid a misdiagnosis.
Differential diagnosis MCL must be distinguished from other small B-cell lymphomas that may disseminate to the skin, including follicular lymphoma and B-small lymphocytic lymphoma/chronic lymphocytic leukemia, cutaneous follicle center lymphoma, and PCMZL. Differentiation from primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT) may also be problematic.45 Follicular lymphoma and cutaneous follicle center lymphoma are typically CD5–/CD10+, marginal zone lymphoma, and PCDLBCL-LT are CD5–/ CD10– and small cell lymphocytic lymphoma is CD5+CD23+/CD10–. All are cyclin D1 and SOX11 negative.3,46,47
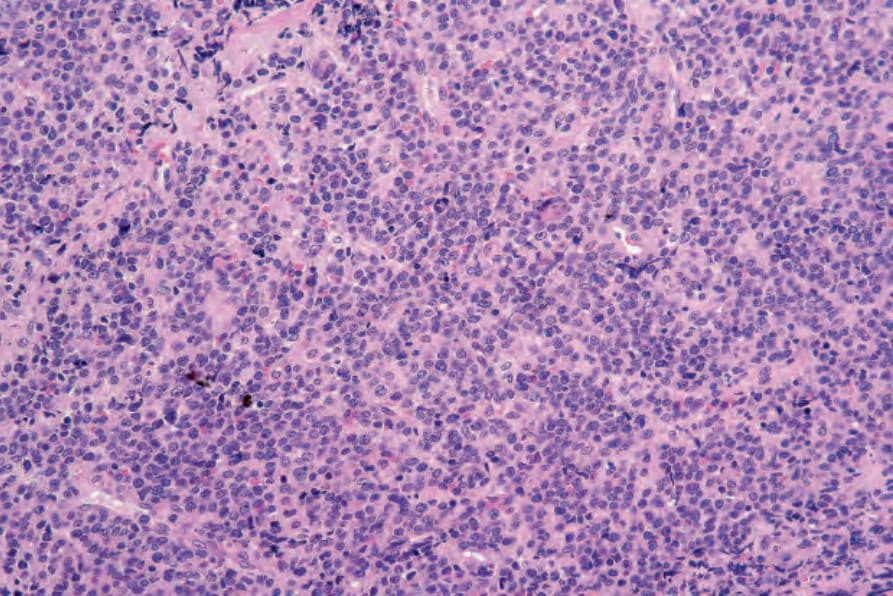
Fig. 29.218 Mantle cell lymphoma: this lesion presented in the subcutaneous fat. The tumor consists of a monomorphic population of lymphoid cells with hyperchromatic nuclei. By courtesy of G. Pinkus, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, USA.
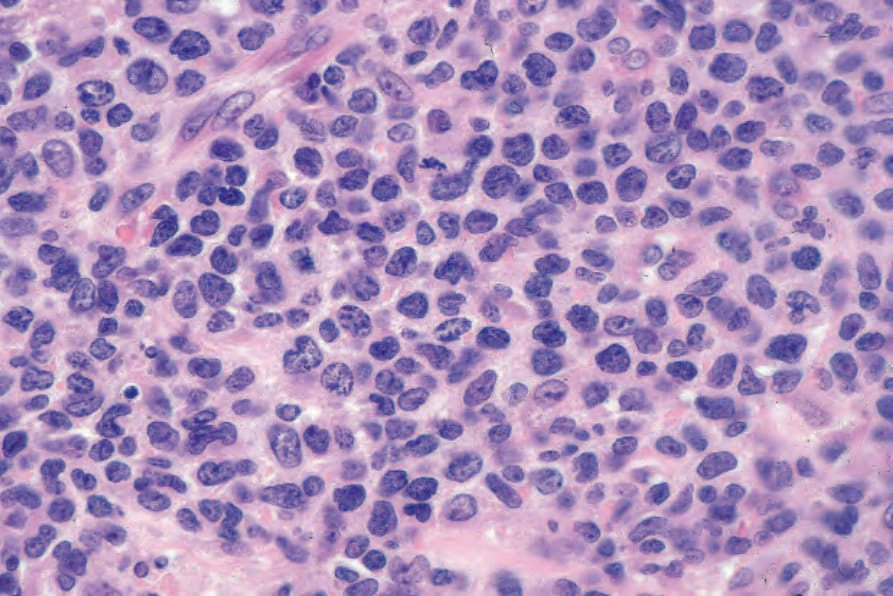
Fig. 29.219 Mantle cell lymphoma: nuclei are irregular. Note the mitosis. By courtesy of G. Pinkus, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, USA.
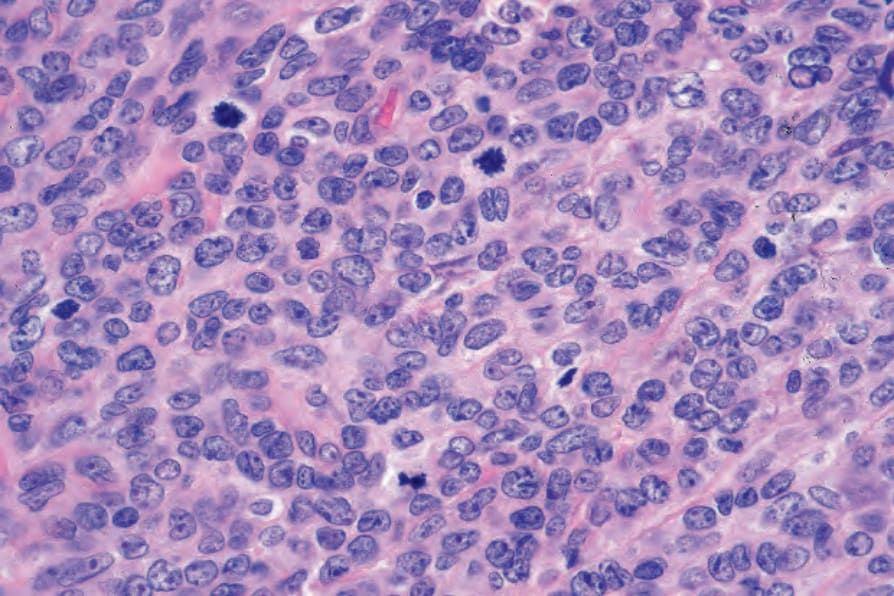
Fig. 29.220 Mantle cell lymphoma: in this field, nucleolated forms are present, and there are multiple mitoses. By courtesy of G. Pinkus, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, USA.