Chronic actinic dermatitis
Chronic actinic dermatitis
Clinical features Chronic actinic dermatitis (CAD) (actinic reticuloid, photosensitivity dermatitis) is a rare chronic photosensitivity reaction of unknown pathogenesis that is of particular importance because it may resemble a lymphoma.1–5
The disease occurs predominantly in middle aged or elderly males.6,7 Young adults of either sex, however, may also be affected.5,8–11 In addition to Caucasians and Asians, CAD sometimes presents in the black population.11–13 The prevalence in Scotland has been estimated as 16 per 100 000.14 A history of allergic contact dermatitis, chronic atopic dermatitis, seborrheic dermatitis, or polymorphous light eruption is not uncommon.5,15 Indeed, a preliminary diagnosis of contact allergy is often documented before the significance of the photosensitive component is realized. Patients develop an intensely pruritic, scaly, erythematous eruption, which is initially limited to the sun-exposed areas, particularly the face, back of the neck, and the hands.1,7 However, lesions also develop on covered sites. Involvement of the eyelids may point toward an allergic contact reaction.5 With further progression, edematous, lichenified, thickened plaques and smooth-topped papules develop (Figs 29.180 and 29.181).6 In severe cases, lesions may become confluent on exposed areas, giving rise to a leonine facies. Patients
with CAD are prone to episodes of erythroderma, which may resemble Sézary syndrome, and in some cases there is palmoplantar involvement.15 Circulating Sézary cells are common and sometimes present in high numbers (2.5–18% of white cells), particularly in erythrodermic patients when a reversed helper/suppressor T-cell ratio is commonly found.2,16–19 Lymphadenopathy is frequently present. Improvement of the photosensitivity may occur over time, and rarely there is also resolution of the contact allergy.20 A case associated with adult T-cell leukemia has been reported.21
Pathogenesis and histologic features CAD is associated with sensitivity to ultraviolet (UV) B (290–320 nm), UVA (320–400 nm), and parts of the visible spectrum (400–700 nm).16 Patients
1459 Chronic actinic dermatitis
also commonly show evidence of contact allergy, and sesquiterpene lactone mix, composite oleoresins, rubber components, potassium dichromate, sunscreens components (benzophenone, butyl methoxydibenzoylmethane, and ethylhexyl benzophenone), fragrances including musk ambrette, and, most recently, p-phenylenediamine, parthenium, and xanthium have been incriminated.6,22–24 Occasional patients are HIV positive.7 It has been suggested that impaired antigen recognition and increased levels of antigen-specific suppressor T cells, which develop as a consequence of UV hypersensitivity, may result in a state of chronic low-grade antigen stimulation and the subsequent development of an atypical cellular immune reaction.25
The histologic features are variable. Biopsy specimens from less severely affected patients may show only the features of a chronic dermatitic process: parakeratosis, acanthosis, spongiosis, and a superficial perivascular chronic inflammatory cell infiltrate.1,7,16 In patients with more extensive involvement, there is commonly a very dense cellular infiltrate involving the papillary and reticular dermis, sometimes extending into the subcutaneous fat (Fig. 29.182).6,7 The infiltrate is composed of lymphocytes, histiocytes, and variable numbers of eosinophils and plasma cells (Figs 29.183 and 29.184). Multinucleate stellate myofibroblasts are common, and occasionally giant cells are a conspicuous feature.7,16 The latter appear to be particularly related to foci of elastolysis.6 Of importance is the occasional finding of large atypical and hyperchromatic cerebriform lymphoid cells and large transformed cell forms, which can raise the suspicion of a cutaneous lymphoma.6 Mitoses can be conspicuous. The epidermis may show exocytosis, but Pautrier microabscess-like features are only rarely evident (Fig. 29.185). Fibrosis of the superficial dermis is a common manifestation.
Ultrastructural examination of specimens from patients with CAD have demonstrated large numbers of Sézary-type cells.2,3,19
The lymph nodes usually show the features of dermatopathic lymphadenopathy, but rarely Sézary cells are identified in the paracortical region and sinuses.6
The results of immunohistochemistry are variable. In general, CD4+ helper T cells are more common in the cellular infiltrate in early lesions but, with increasing severity, the CD8+ suppressor subset usually predominates.6,7,16,26,27 IgE-positive dendritic cells are frequently present in the dermal infiltrate.6,27
Although a small number of cases with associated lymphoma have been documented, these may be coincidental.6,28–30 DNA flow cytometry studies have given conflicting results, varying from complete absence of aneuploidy to presence in 63% of patients.25,31 TCR gene rearrangement studies usually resolve this dilemma.32,33 Although occasional cases demonstrate a clonal population, in a more recent study of 12 cases of CAD, no TCR gene rearrangements were identified.33–36 In the largest series published to date, none of the 231 patients with CAD had an associated lymphoma.37
1460 Cutaneous lymphoproliferative diseases and related disorders
Differential diagnosis In the absence of an adequate clinical history, actinic reticuloid may be histologically confused with patch/plaque stage mycosis fungoides or Sézary syndrome. The matter is further complicated by the rare occurrence of erythrodermic cutaneous T-cell lymphomas with severe photosensitivity.38 Histologic points of diagnostic help include the presence of multinucleate stellate myofibroblasts, eosinophils and plasma cells, and the absence of
Pautrier microabscesses in CAD. The CD8+ phenotype of actinic reticuloid contrasts with the CD4+ proliferation characteristic of mycosis fungoides and Sézary syndrome.15,33 Similarly, study of the peripheral blood may reveal a decreased or even reversed CD4:CD8 ratio.32

Fig. 29.180 Chronic actinic dermatitis: marked erythema, edema, and thickening of the skin. From the collection of the late N.P. Smith, MD, The Institute of Dermatology, London, UK.

Fig. 29.181 Chronic actinic dermatitis: prominent lichenification. From the collection of the late N.P. Smith, MD, The Institute of Dermatology, London, UK.
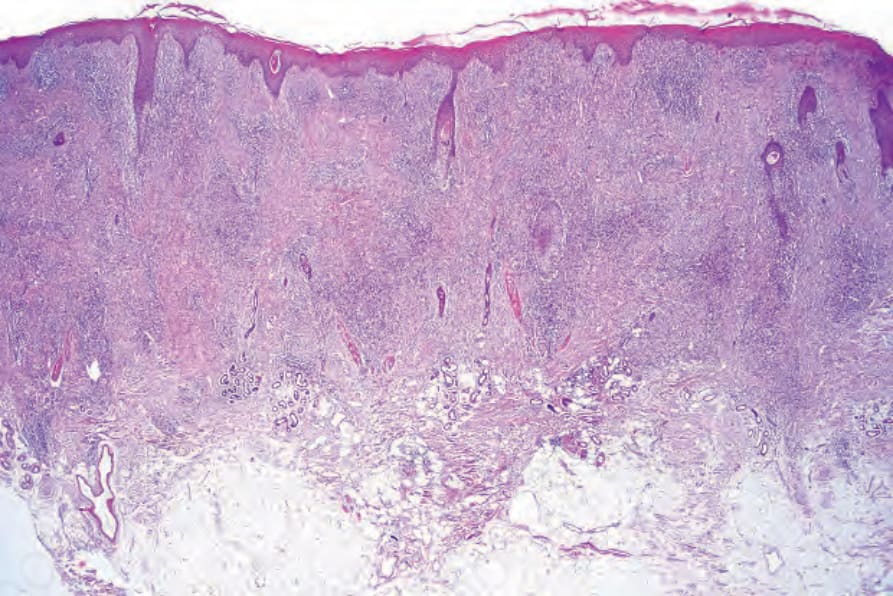
Fig. 29.182 Chronic actinic dermatitis: a dense infiltrate extends throughout the dermis and fibrosis is evident.
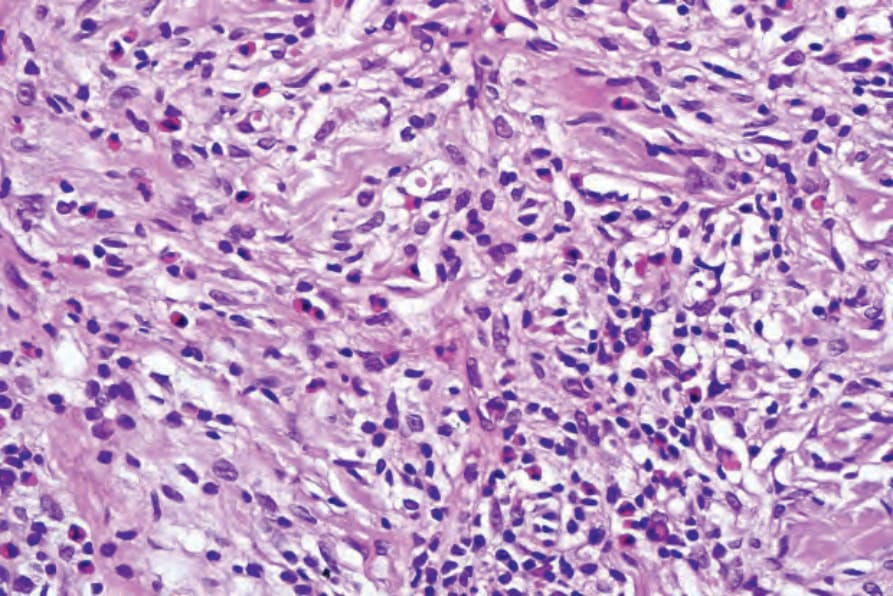
Fig. 29.183 Chronic actinic dermatitis: the infiltrate consists of lymphocytes, eosinophils, and histiocytes.
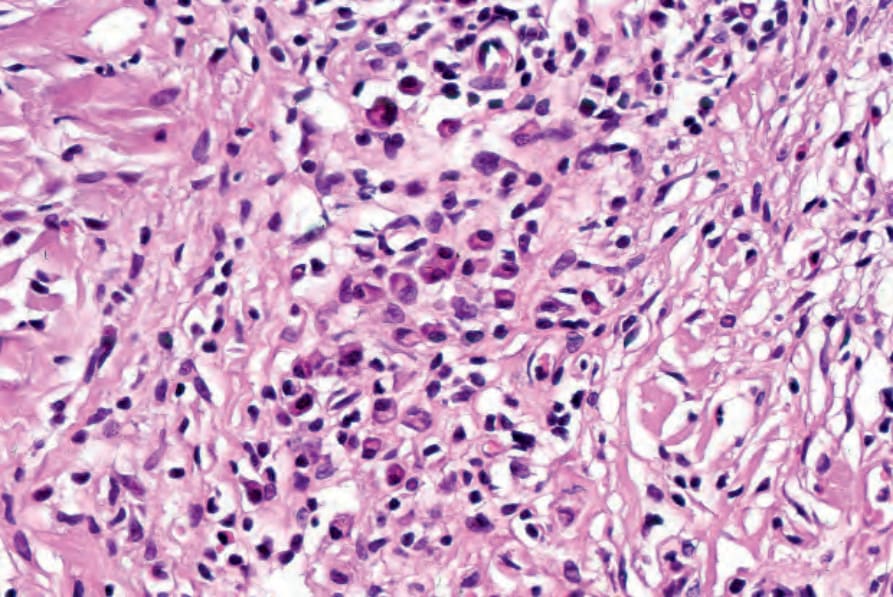
Fig. 29.184 Chronic actinic dermatitis: conspicuous plasma cells are present.
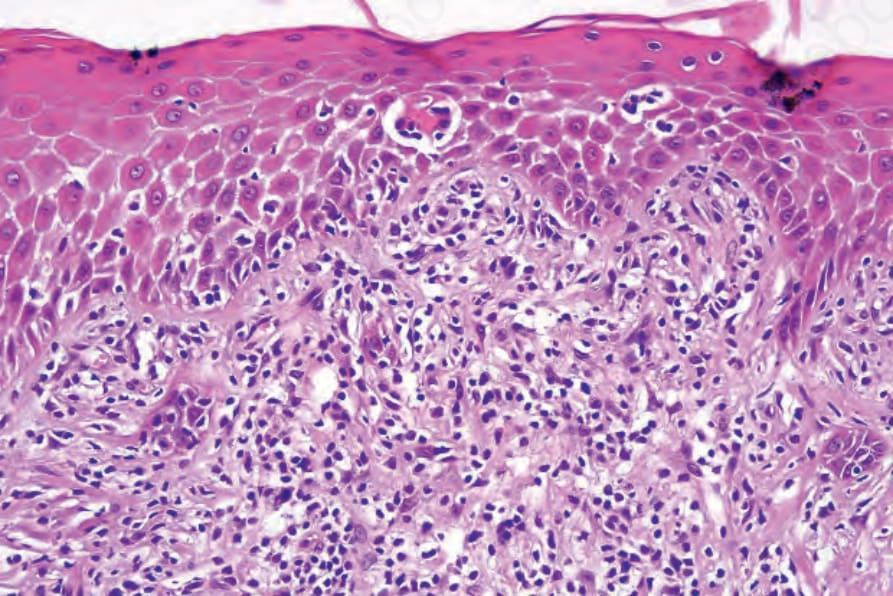
Fig. 29.185 Chronic actinic dermatitis: there is mild cytological atypia. Focal epidermotropism is evident.