Pseudolymphomatous folliculitis
Pseudolymphomatous folliculitis
Clinical features Pseudolymphomatous folliculitis is uncommon and presents in the head and neck region as solitary red or violaceous, nonulcerated, solitary nodules, measuring up to 3 cm in diameter.1–6 The sexes are affected equally, and most patients are in their fourth or fifth decade.2,4 Surgery seems to be adequate treatment since only one case of recurring lesions has been reported.4 Even when not fully excised, lesions tend to spontaneously regress.2,3
Pathogenesis and histologic features The etiology in the vast majority of cases is unknown. One case had a history of previous insect bite, in two a history of antecedent trauma, and in another, B. burgdorferi DNA was demonstrated.1,2,4 The striking folliculocentricity and conspicuous dendritic cell population suggest that the condition most probably represents an exuberant hypersensitivity reaction to an as yet unidentified follicular antigen.
the background, there are numerous small blood vessels lined by plump but not epithelioid endothelial cells. These vessels have features of high endothelial venules seen in lymph nodes (Fig. 29.176). The infiltrate consists mainly of CD3-positive lymphocytes, and both CD4+ and CD8+ cells are represented (Figs 29.177–29.179). B cells are sparse. Cytological atypia is not seen. Eosinophils and plasma cells may be seen. Old lesions display some degree of fibrosis.
The salient diagnostic features are the presence of a dense nodular or diffuse folliculocentric infiltrate, together with hyperplasia and distortion of pilosebaceous units.2,4,5 The infiltrate is usually separated from the epidermis by a grenz zone and may involve the subcutis.2–4 It consists of lymphocytes with variable numbers of histiocytes, plasma cells, and, in some cases, eosinophils.1,2,4 The lymphocytes are usually small, although in some cases medium to large lymphocytes are present, either with irregular hyperchromatic nuclei or an immunoblastic appearance.2,4 Lymphoid follicles are rare.4 The histiocytes generally have an epithelioid appearance and are often clustered around infiltrated hair follicles and sebaceous glands.2 Small noncaseating granulomata can be seen.4
Differential diagnosis The main differential diagnosis is with pseudolymphomatous angiokeratoma (APACHE).2–4 Similar lesions have also been described under different rubrics including papular angiolymphoid proliferation with epithelioid features in adults and children (PALEFACE) and angiolymphoid hyperplasia with high endothelial venules (APA-HEL).5,6 There is undoubtedly some overlap with pseudolymphomatous angiokeratoma (APACHE). However, TRAPP occurs on the head and trunk, it presents as a solitary lesion, with adult predilection, and it is always polypoid with an epithelial collarette and lack of interface change.
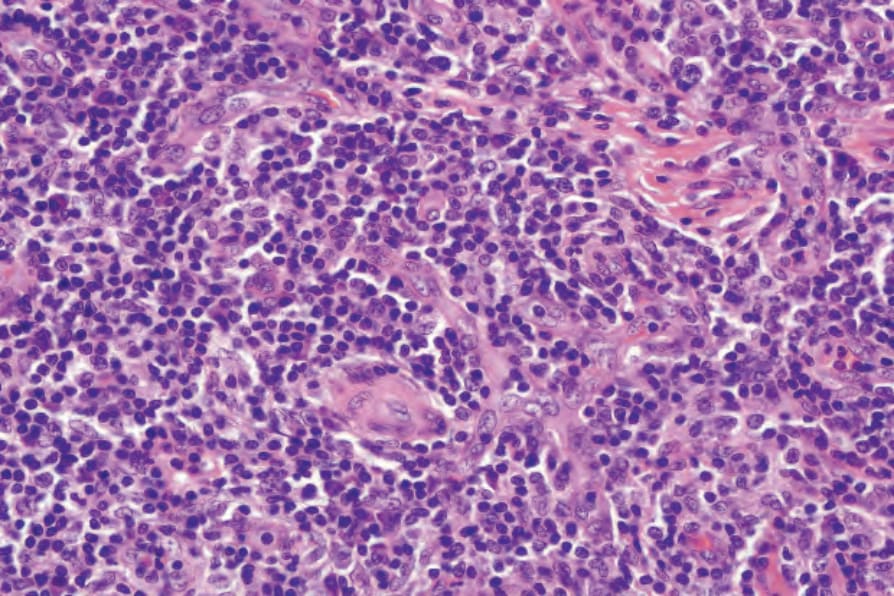
Fig. 29.176 T-cell rich angiomatoid polypoid pseudolymphoma (TRAPP): high-power view of blood vessels and small lymphocytes.
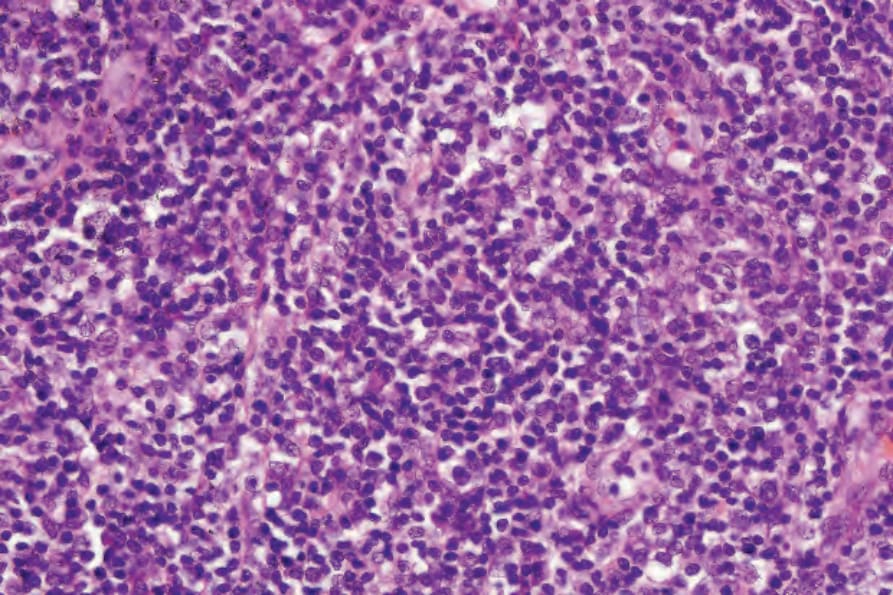
Fig. 29.177 T-cell rich angiomatoid polypoid pseudolymphoma (TRAPP): detailed view of infiltrate.
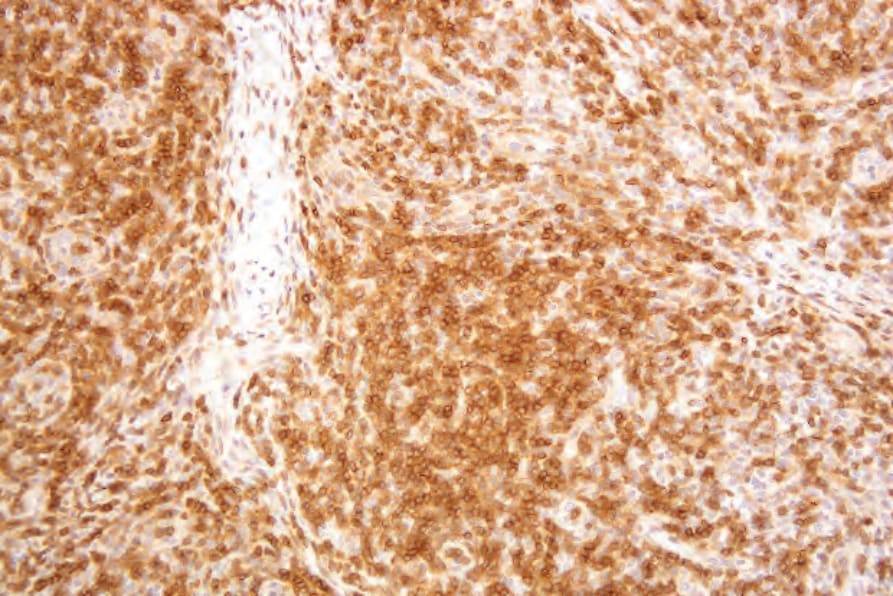
Fig. 29.178 T-cell rich angiomatoid polypoid pseudolymphoma (TRAPP): the lymphocytes express CD3.