Intravascular pseudo-T-cell lymphoma
Intravascular pseudo-T-cell lymphoma
Clinical features Rarely, intralymphatic aggregates of CD30 positive or, less commonly, CD30 negative blastic cells are seen in skin biopsies performed in the setting of trauma or various inflammatory and neoplastic pathologies including lichen sclerosus, hidradenitis suppurativa, and hemangioma.1–6 The behavior appears to be benign with no adverse effects in any of the cases reported so far.
Histologic features A variable number of dermal lymphatics appear dilated by a proliferation of blastic cells that are frequently, but not always, CD30 positive (Figs 29.171–29.173). Other T-cell markers including CD3 and CD4 are usually expressed. B-cell markers are negative. The proliferating cells are usually polyclonal.
Differential diagnosis The differential diagnosis includes intravascular T, NK/T, or B cell lymphoma and intravascular histiocytosis. Clinicopathological correlation, immunophenotyping, and clonality studies are crucial to establish the right diagnosis.
1456 Cutaneous lymphoproliferative diseases and related disorders
the endothelial cells in pseudolymphomatous angiokeratoma appear to express WT1.12
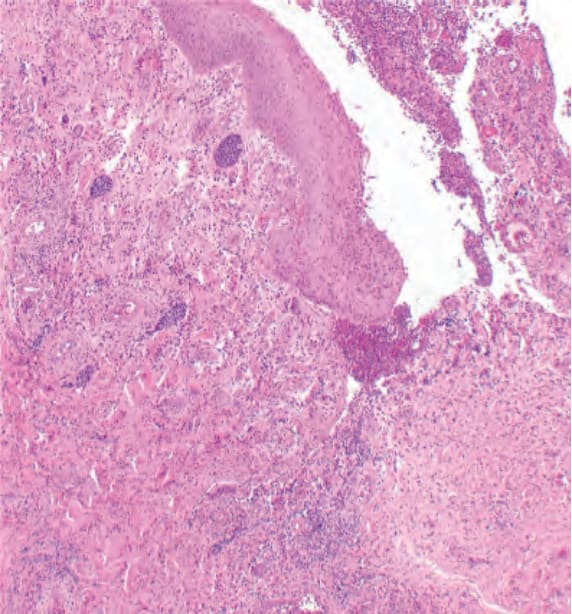
Fig. 29.171 Intravascular pseudo-T-cell lymphoma: numerous dilated lymphatic channels containing blastic lymphoid cells.
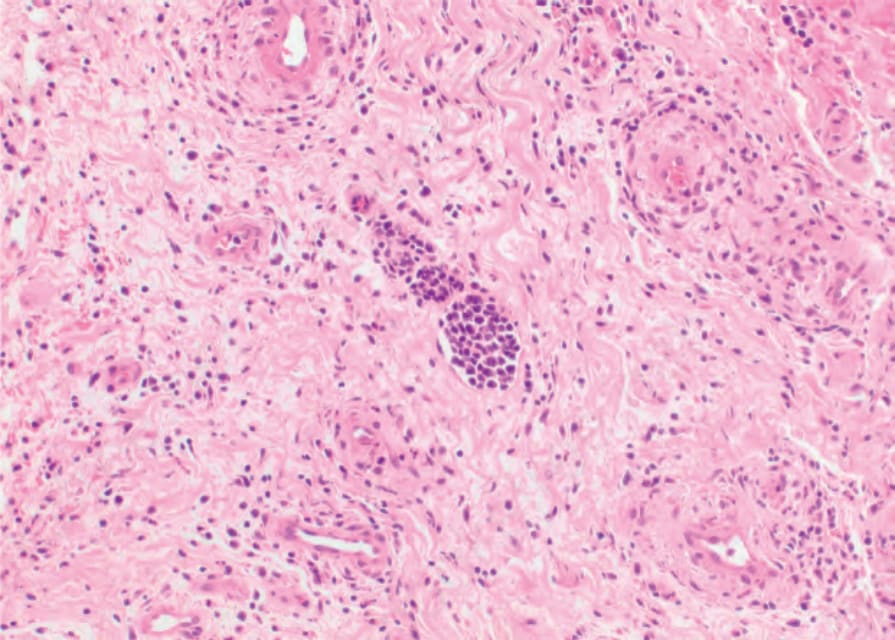
Fig. 29.172 Intravascular pseudo-T-cell lymphoma: closer view of a dilated lymphatic vessel containing blastic lymphoid cells.
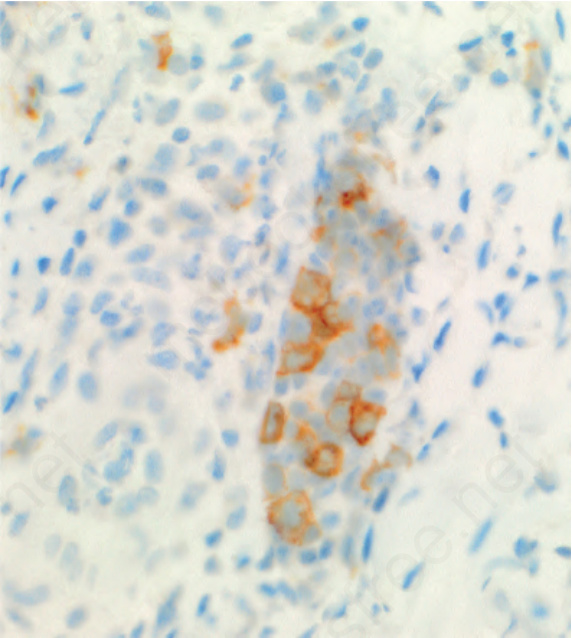
Fig. 29.173 Intravascular pseudo-T-cell lymphoma: many but not all of the blastic cells T cells are positive for CD30.
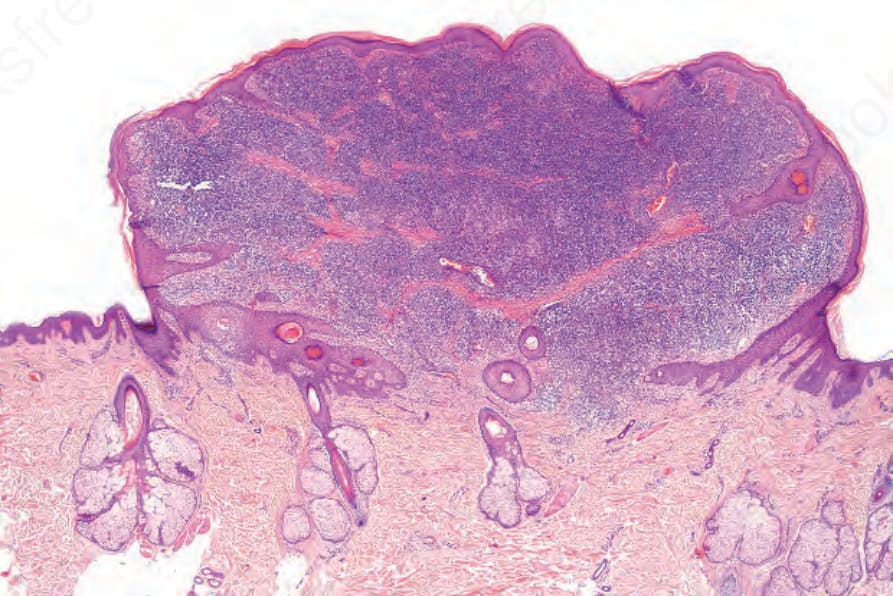
Fig. 29.174 T-cell rich angiomatoid polypoid pseudolymphoma (TRAPP): scanning view of polypoid nodule.
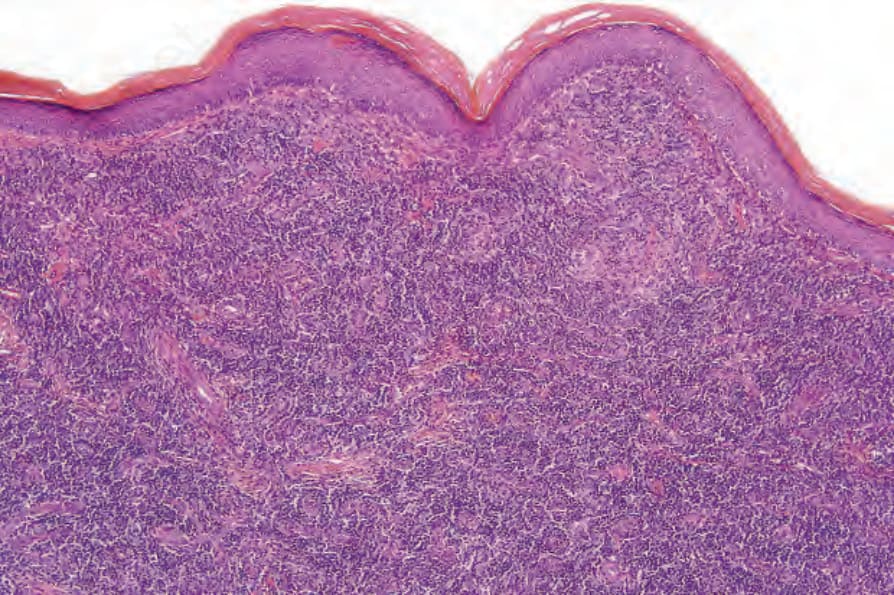
Fig. 29.175 T-cell rich angiomatoid polypoid pseudolymphoma (TRAPP): medium-power view showing lack of epidermal involvement.