Adult T-cell leukemia/lymphoma
Adult T-cell leukemia/lymphoma
Clinical features Adult T-cell leukemia/lymphoma (ATLL) is a systemic disease induced by human T-cell leukemia virus type 1 (HTLV-1) with variable clinical manifestations, and frequent skin involvement. It was first described on the island of Kyushu in southwestern Japan.1–3 It also occurs in the Caribbean,
1446 Cutaneous lymphoproliferative diseases and related disorders
northeastern South America, southeastern United States, Central Africa, and the Pacific basin.4,5 Cases are occasionally diagnosed in the rest of the United States and Europe as a consequence of immigration.6 The disease predominantly affects adults, pediatric cases being rare.7
There may be a prodromal phase, but once established, four variants are recognized: acute, chronic, smoldering. and lymphomatous:1,2,8
• Acute ATLL (55%): This is the most common subtype, usually presenting with an abrupt onset, and is characterized by a leukemic phase. Hypercalcemia, with or without lytic bone lesions, constitutional symptoms, and raised LDH are typical. A very high white cell count, numerous circulating neoplastic lymphocytes, neutrophilia, and eosinophilia are common. Skin lesions are present in about 50% of cases, and there may be lymphadenopathy and hepatosplenomegaly.
• Chronic ATLL (20%): A lymphocytosis may be present with few circulating atypical lymphoid cells. Hypercalcemia is absent and serum LDH is normal or only slightly raised (less than or equal to twice the upper limit of normal). Skin lesions, including an exfoliative rash, may occur and there may be mild lymphadenopathy and/or splenomegaly.
• Smoldering ATLL (5%): The lymphocyte count is normal but >5% of circulating lymphocytes are abnormal T cells. Hypercalcemia is absent. Skin and pulmonary involvement are frequent. Lymphadenopathy or hepatosplenomegaly are absent. Serum LDH is normal or only slightly raised (less than or equal to 1.5 times the upper limit of normal).
• Lymphomatous ATLL (20%): Peripheral blood involvement is seen in this variant, the disease being characterized by prominent lymphadenopathy, usually of advanced stage. Hypercalcemia is less frequent than in the acute form of the disease, but skin lesions are common. Cutaneous lesions are reported in 43–72% of cases and may be seen in all forms of the disease, but are less common in the lymphomatous subtype (Figs 29.145 and 29.146).2,9–13 Skin lesions are somewhat heterogeneous, presenting as papules, nodules, tumors, plaques, or erythema/erythroderma.10,14,15 Rarely, pompholyx-, keloid-, and granuloma-like lesions and hyperpigmented, purpuric, vesicular, and bullous lesions are seen.10,16,17 A cutaneous variant, in which monoclonal lymphocytes proliferate in skin only, has been proposed.14,18–20 This is because such cases are associated with a poorer prognosis than smoldering ATLL (the category in which most would currently be grouped), but a much better outcome than the other variants.14,21
whilst those with eryhtroderma have a particularly poor outcome.1,2,22 The median survival for acute and lymphomatous variants ranges from around 2 weeks to 1 year while patients with chronic and smoldering forms can survive for up to 2 years or longer.1,23 Death is usually due to infection, hypercalcemia, or tumor burden.
Pathogenesis and histologic features ATLL develops only in HTLV-1 infection and the malignant cells contain integrated HTLV-1 provirus, providing strong support for a causative role.24 HTLV-1 is transmitted via peripheral blood (intravenous drug abuse, sexual intercourse), blood products, or from mother to child transplacentally or via breast milk. However, a relatively low proportion of infected individuals go on to develop ATLL, the cumulative risk for males being 6.6% and for females 2.1%.24,25 There is also a long latent period, most cases seeming to follow transmission by breastfeeding, with the average age of a Japanese patient being 60 years.24,26 This implies that an as-yet unidentified cofactor is necessary for transformation.
HTLV-1 proviral DNA is randomly integrated into host cell DNA with transcription of viral genes. Expression of the transcriptional transactivator protein, Tax, and/or the HTLV-1 basic leucine zipper factor seems to be important for transformation. These may act via downstream effects on cell cycle progression and/or apoptosis following activation of the NF-κB pathway.24,26,27
Complex karyotypes are seen in ATLL together with a variety of clonal chromosomal abnormalities.4,28–33 Mutations or loss of function of a number of tumor suppressor genes, including cyclin-dependent kinase inhibitors (p15, p16), p53, and Rb have also been identified, particularly in the lymphomatous and acute variants.34,35 Overexpression of p21 may also occur.36 Recurrent mutations involving the RHOA, TET2, and CCR4 genes have also been demonstrated in a significant percentage of cases.36–39
Many patients have a T-cell-associated immunodeficiency and are immunocompromised. Opportunistic infections, including Pneumocystis jiroveci pneumonia, candidiasis, cryptococcosis, CMV, and strongyloidiasis, are common. Prognosis is related to the clinical subtype, age, serum calcium, and LDH levels and, for cases with cutaneous involvement, the type of skin lesion, those with patches and plaques doing relatively well,
Circulating leukemic cells have characteristic morphology with hyperlobated pleomorphic nuclei that sometimes resemble a clover leaf, with condensed chromatin and inconspicuous nucleoli.40 They contain acid phosphatase, β-glucuronidase, and acid-naphthyl acetate esterase.41 Immunophenotypically, they are helper/inducer T lymphocytes.42
In tissues, a broad spectrum of cytological appearances may be seen including pleomorphic small, medium, and large cell, anaplastic large cell, Hodgkin-like and AITL-like (Figs 29.147 and 29.148).43 Cutaneous lesions may show perivascular, nodular, or diffuse patterns of infiltration.14 In erythematous lesions, tumor cells are located in the upper dermis and are small to medium-sized lymphocytes with mild nuclear irregularity and few mitotic figures. In papules and nodules, a pan-dermal and sometimes subcutaneous nodular or diffuse infiltrate is seen. The lymphocytes are usually of medium to large size with highly irregular nuclear outlines, coarsely
1447 Adult T-cell leukemia/lymphoma
A
clumped chromatin, and sometimes prominent nucleoli. Blast-like cells, cerebriform giant cells, and Reed-Sternberg-like cells are present in some cases, and mitotic figures are frequent. Epidermotropism, with Pautrier microabscesses, may be seen, most frequently in association with perivascular infiltrates and lesions resemble mycosis fungoides or Sézary syndrome.1,5,13,14,42–44 Histiocytes, plasma cells, and sometimes eosinophils are often evident.42,44 Rare cases are associated with follicular mucinosis and granulomas are exceptional.16,45–48
B
In addition to bone marrow, skin, and lymph node involvement, widespread tumor infiltration is commonly present in the lung, liver, kidney, gastrointestinal tract, and central nervous system (CNS), in decreasing order of frequency.16
The cells are usually CD2+, CD3+, CD4+, CD5+, CD25+, and CD7– (Figs 29.149 and 29.150).1,5 CD8+ variants have occasionally been documented, and rarely the tumor cells express both CD4 and CD8.1,42 The large transformed cells may express CD30 but are negative for ALK1 and cytotoxic molecules. The tumor cells also frequently express the chemokine receptor CCR4 and FoxP3, suggesting a relationship to T-regulatory cells.49
Differential diagnosis ATLL may show considerable overlap with mycosis fungoides and Sézary syndrome. The acute onset and typical lack of a patch stage are useful discriminants.5 In cases of doubt, the diagnosis of ATLL may be firmly
1448 Cutaneous lymphoproliferative diseases and related disorders
established serologically or by the identification of HTLV-I sequences in tumor DNA.

Fig. 29.145 Adult T-cell leukemia/lymphoma: in this case, multiple papules are seen on the lips. By courtesy of the Institute of Dermatology, London, UK.

Fig. 29.146 Adult T-cell leukemia/lymphoma: innumerable papules and nodules are present on the arm. By courtesy of the Institute of Dermatology, London, UK.
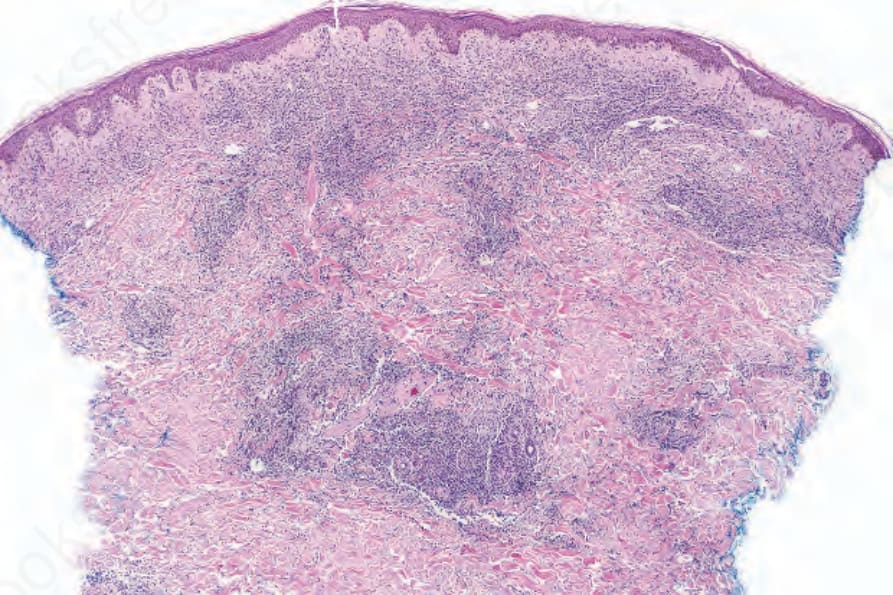
Fig. 29.147 Adult T-cell leukemia/lymphoma: there is a dense infiltrate within the dermis.
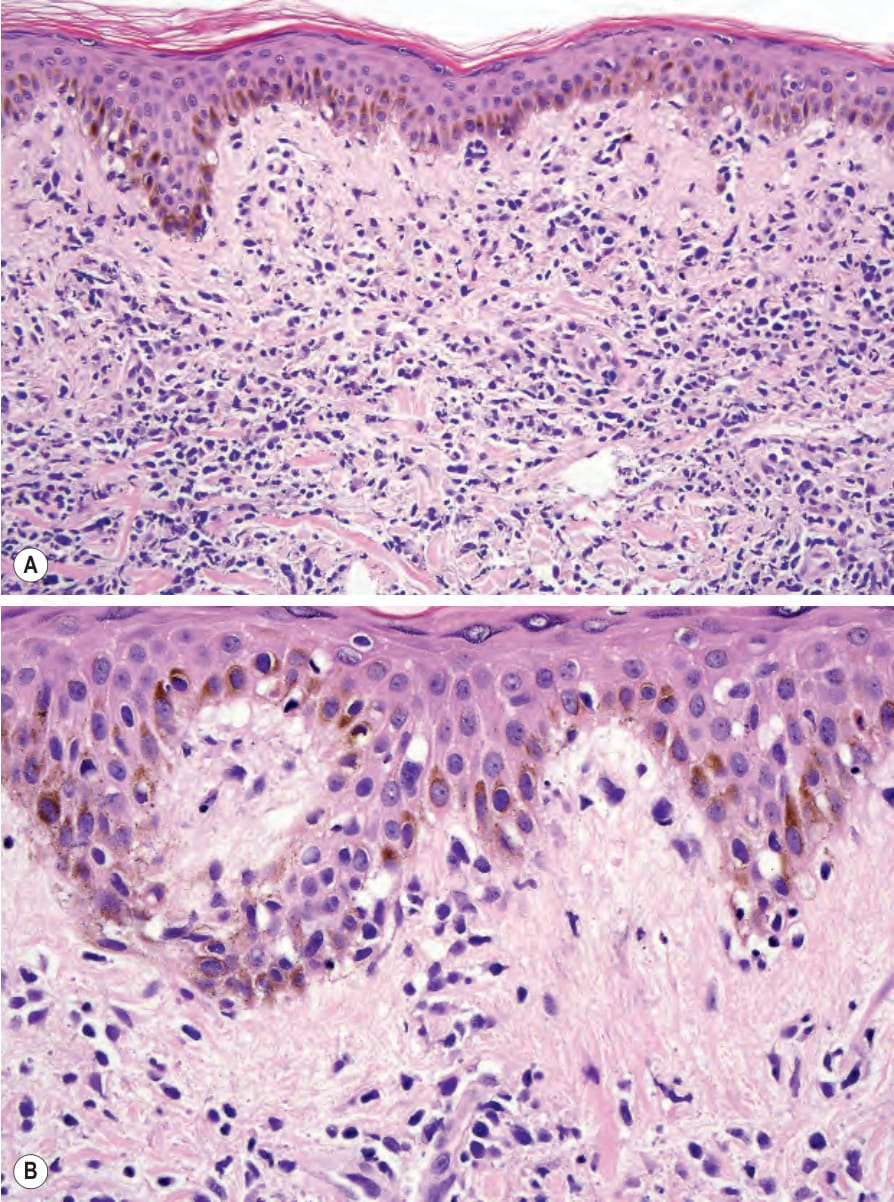
Fig. 29.148 (A, B) Adult T-cell leukemia/lymphoma: the infiltrate is composed of an admixture of small and large pleomorphic lymphocytes. Note the epidermotropism. Distinction from mycosis fungoides depends on clinicopathological correlation.
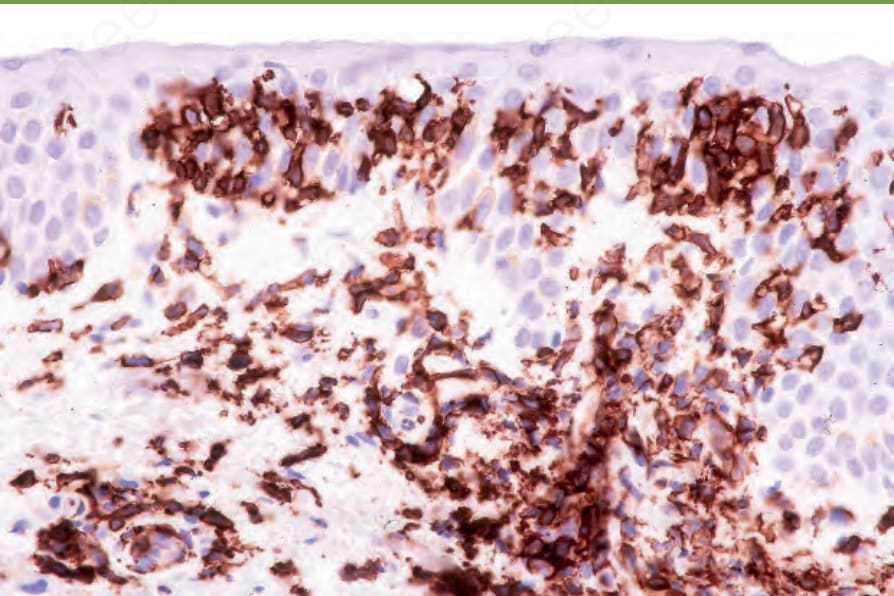
Fig. 29.149 Adult T-cell leukemia/lymphoma: the lymphocytes are CD4+ T-helper cells.
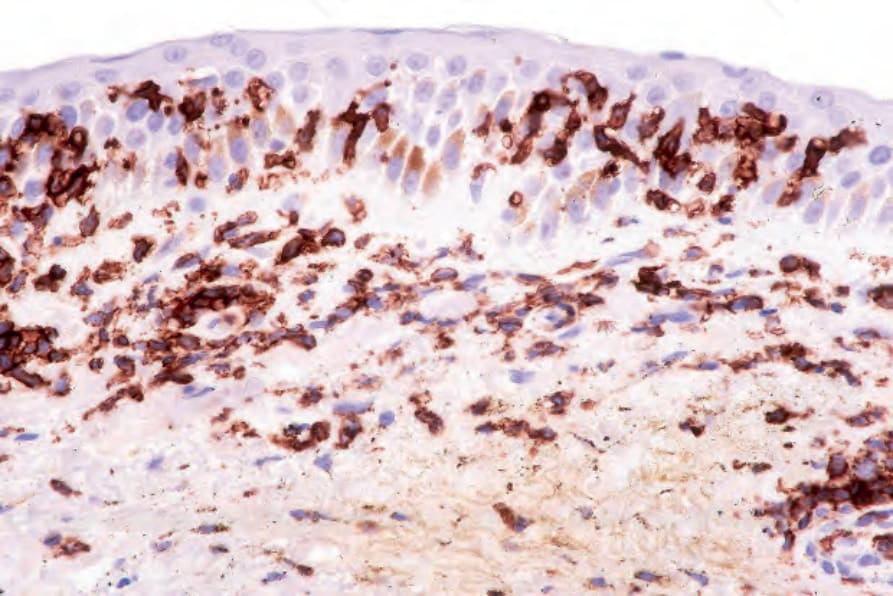
Fig. 29.150 Adult T-cell leukemia/lymphoma: there is uniform CD25 expression.