Folliculotropic mycosis fungoides
Folliculotropic mycosis fungoides
Clinical features Folliculotropic MF is a rare, biologically distinct variant of MF characterized by follicular infiltrates of cerebriform T cells, often with sparing of the epidermis. While a number of cases are associated with follicular mucinosis, this is not a prerequisite for making the diagnosis,1–3 despite earlier reports suggesting that lymphomas with and without this feature should be regarded separately.4–6 The disease has been described under different names including follicular MF,5–10 pilotropic MF,4,11 folliculotropic MF,2 MF
1425 Distinct variants of mycosis fungoides
presenting with follicular mucinosis,12 MF-associated follicular mucinosis,13 and basaloid folliculolymphoid hyperplasia with alopecia.14
that folliculotropic MF is generally more refractory to treatment, with lower rates of complete remission. However, even when treated more aggressively at the outset, outcomes are poor,1 and there may be intrinsic differences in tumor cell biology that contribute to outcome.14,16
Follicular MF is more common in middle aged to elderly males.1–3 It has predilection for the head and neck, particularly the face and scalp, although lesions are frequently seen on the trunk.1–3 Involvement of the limbs may also be seen. Most patients present with patches, plaques, or grouped papules (Figs 29.69–29.73).1–3 Tumor stage lesions may also be encountered.2,3 Intense pruritus and alopecia are common. Less frequent are acneiform lesions such as comedone-like cysts, pustules, or milia.1,3 Some patients present with spiky keratosis. In lesions associated with sweat gland involvement, hypohydrosis may also be a feature.15 Mucinorrhea and erythroderma are rarely seen.3
The principal reason for distinguishing folliculotropic MF as a specific entity is because it is more difficult to treat than classic MF and has a higher incidence of disease progression with worse prognosis. Early-stage folliculotropic MF has a significantly poorer progression-free, disease-free, and overall survival than classic MF and displays outcomes more similar to those seen in tumor stage MF.1–3,16,17 This may in part be due to the fact
Histologic features and pathogenesis The pathogenesis of folliculotropic MF is unknown, although it has been speculated that folliculotropism is mediated through intracellular adhesion molecule 1 (ICAM-1) expression by follicular epithelium and lymphocyte function-associated antigen (LFA-1) expression by the lymphoid cells.4 Gene expression profiling studies have also shown that folliculotropic MF cases tend to express genes associated with inflammation and pathways involved with epidermal proliferation, and to cluster with cases of typical MF of advanced stage with poor prognosis.14
The defining histologic feature of this variant is infiltration of hair follicle epithelium by medium to large cerebriform cells (Figs 29.74–29.81).1,3 Collection of acid mucopolysaccharides within the involved follicles (follicular mucinosis) is present to varying degrees but is often absent.1,3 Other histologic features include basaloid follicular hyperplasia, granulomatous inflammation, numerous eosinophils in and around hair follicles, and follicular
1426 Cutaneous lymphoproliferative diseases and related disorders
1427 Distinct variants of mycosis fungoides
cystic change even with formation of epidermoid cysts and comedone-like lesions.1,16,17 Basaloid follicular hyperplasia refers to the proliferation of basaloid cells extending from follicles, or complete basaloid transformation of hair follicles with infiltrating atypical lymphocytes.1,18 Granulomatous inflammation is usually secondary to ruptured hair follicles. Other non-specific changes may be seen including neutrophilic pustular lesions, syringotropism, prominent interface dermatitis of the follicular epithelium or epidermis, and epidermotropism involving nonfollicular epithelium.16,17 Not infrequently, blast cells are numerous, and large cell transformation may be seen in some cases.1,3
The neoplastic lymphocytes in folliculotropic mycosis fungoides usually have a T-helper phenotype. Blast cells, when present, are often CD30 positive.1,3
Differential diagnosis Folliculotropic MF must be distinguished from lichen planopilaris, pseudolymphomatous folliculitis, eosinophilic folliculitis, follicular lymphomatoid papulosis, and follicular mucinosis/alopecia mucinosa.5
In lichen planopilaris, there is a bandlike infiltrate, colloid bodies are conspicuous, and atypical folliculotropic lymphocytes are lacking. It may be difficult to distinguish folliculotropic MF from pseudolymphomatous folliculitis. In the latter, the hair follicles have an activated appearance, destruction of hair follicles is absent, and lesions tend to be solitary and resolve spontaneously.19 Although PCR was originally said to show polyclonal patterns of gene rearrangement, examples of ‘clonal pseudolymphomatous folliculitis’ have been described.20 Follicular mucinosis may be present incidentally or in conditions such as eosinophilic folliculitis of both Ofuji disease and HIV-associated cases, but atypical folliculotropic lymphocytes are not present.21,22 Clinical features are more helpful in distinguishing follicular lymphomatoid papulosis from folliculotropic MF, in particular, the presence of crops of spontaneously regressing papules.2

Fig. 29.69 Folliculotropic mycosis fungoides: this patient shows a large abdominal scaly patch. By courtesy of H. Naeem, MD, Harvard Medical School, Boston, USA.

Fig. 29.70 Folliculotropic mycosis fungoides: follicular lesions are present on the legs. By courtesy of H. Naeem, MD, Harvard Medical School, Boston, USA. Reproduced from Liu V and McKee PH. Cutaneous T-cell Lymphoproliferative disorders: approach for the surgical pathologist and clarification of confused issues. Advances in Anatomic Pathology. 2002, 9:79–100, with permission from Lippincott Williams & Wilkins.
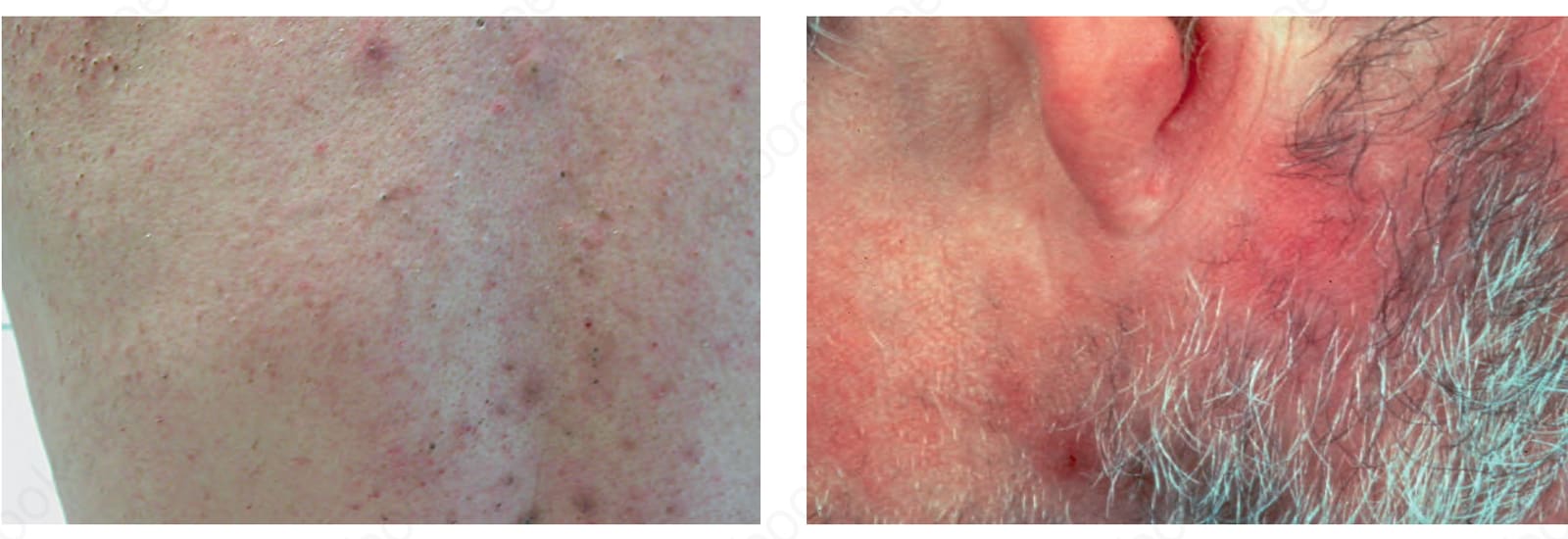
Fig. 29.71 Folliculotropic mycosis fungoides: erythematous lesions are present in the beard area and on the neck. The patient had associated mycosis fungoides. By courtesy of the Institute of Dermatology, London, UK.

Fig. 29.72 Folliculotropic mycosis fungoides: grouped follicular papules are present. The patient had associated mycosis fungoides. By courtesy of the Institute of Dermatology, London, UK.

Fig. 29.73 Folliculotropic mycosis fungoides: mycosis fungoides-associated erythematous plaque. By courtesy of the Institute of Dermatology, London, UK.
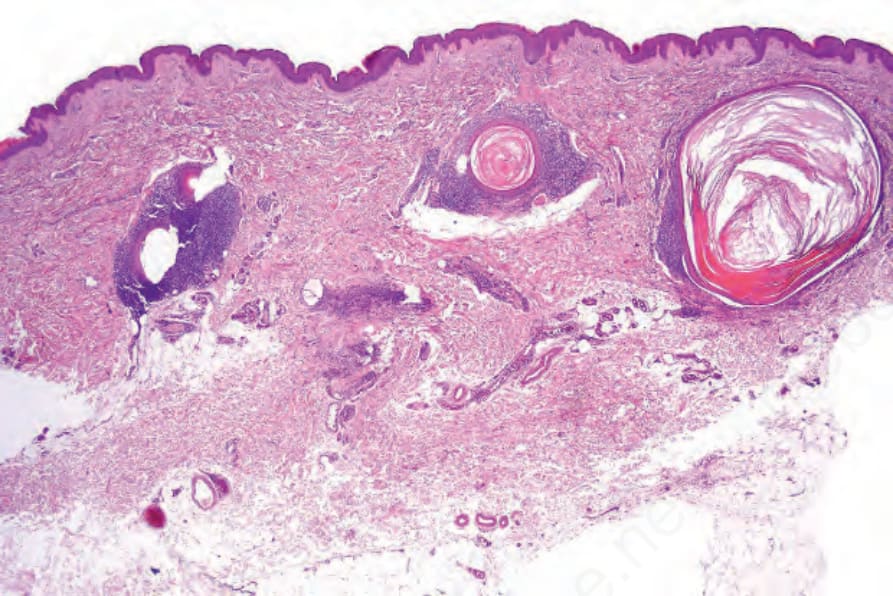
Fig. 29.74 Folliculotropic mycosis fungoides: scanning view showing a folliculocentric lymphoid infiltrate.
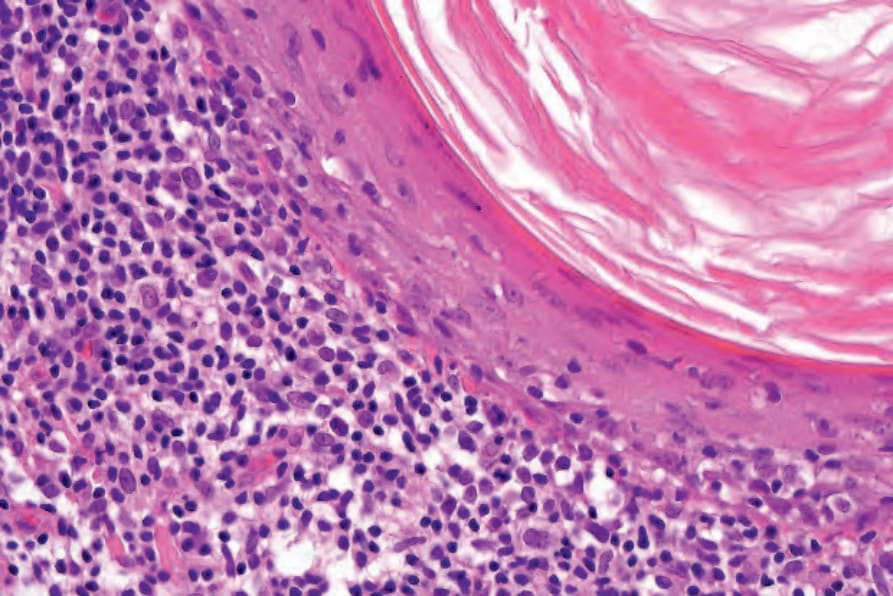
Fig. 29.75 Folliculotropic mycosis fungoides: note the atypical lymphocytes investing the follicle.
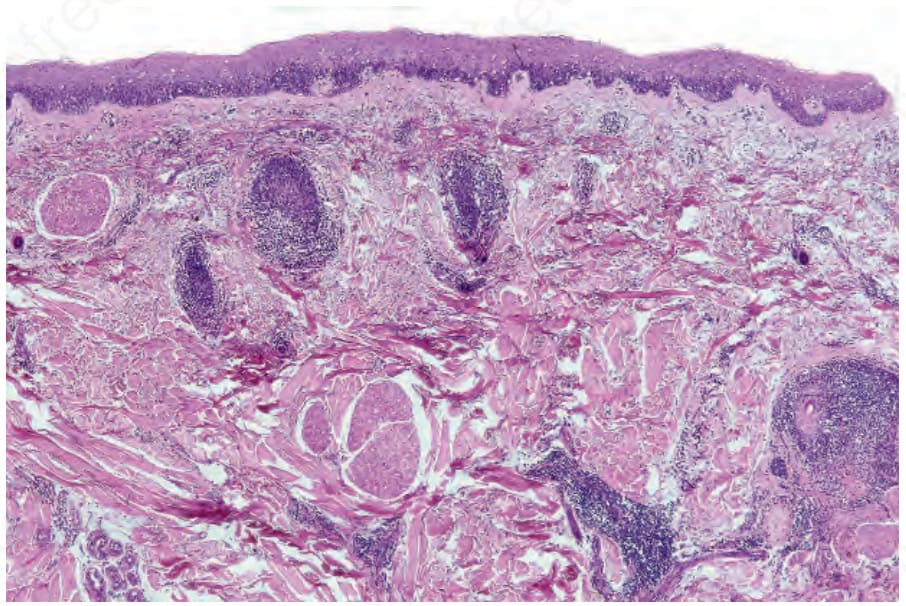
Fig. 29.76 Folliculotropic mycosis fungoides: this specimen comes from the leg. The follicles are ensheathed by an atypical lymphoid infiltrate.
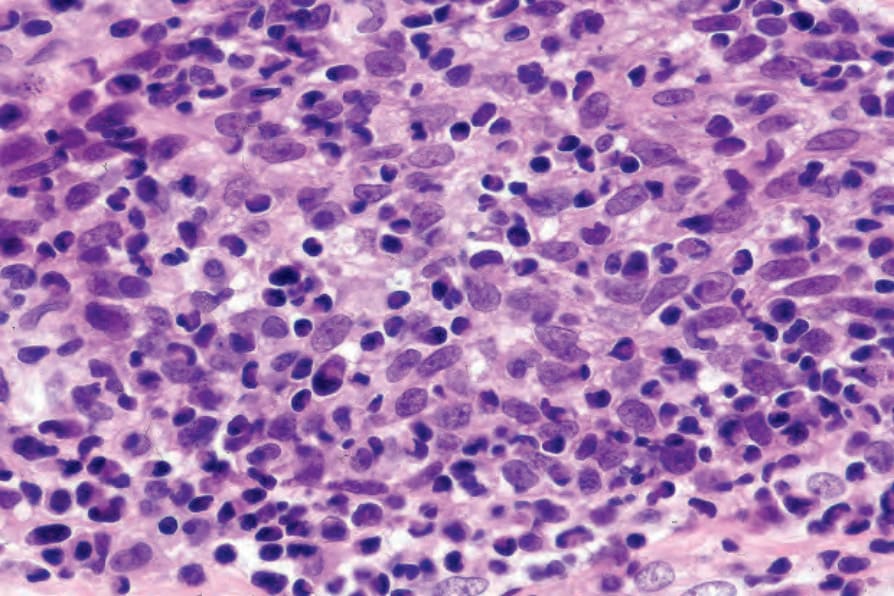
Fig. 29.77 Folliculotropic mycosis fungoides: the follicular epithelium is infiltrated by atypical lymphocytes.
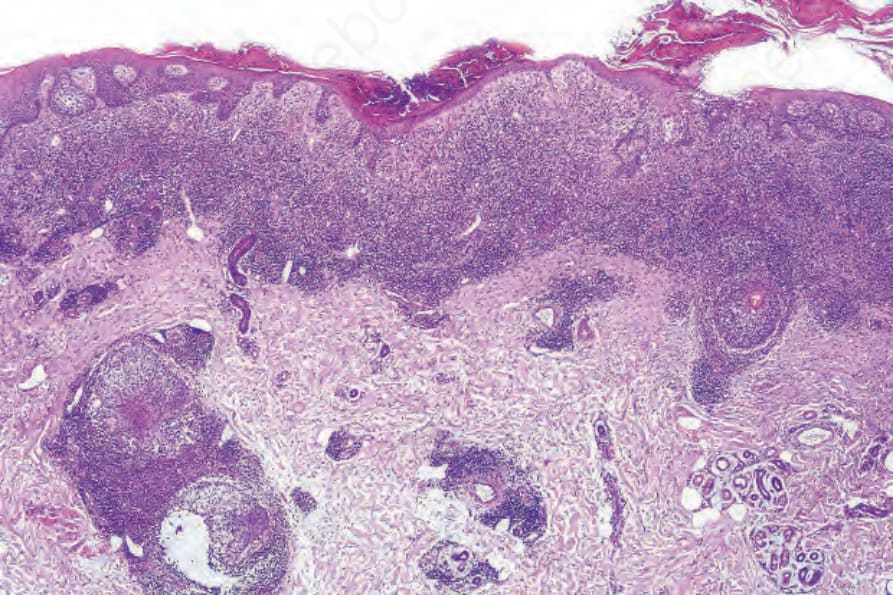
Fig. 29.78 Folliculotropic mycosis fungoides: in addition to a superficial bandlike infiltrate, there is follicular involvement.
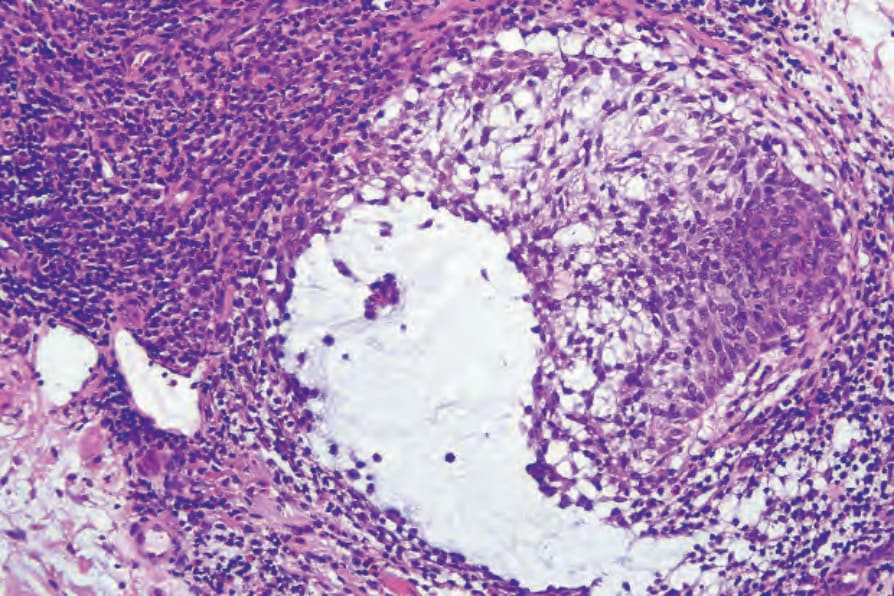
Fig. 29.79 Folliculotropic mycosis fungoides: there is striking follicular mucinosis.