Syringotropic mycosis fungoides
Syringotropic mycosis fungoides
Differential diagnosis Granulomatous MF can be distinguished from granulomatous slack skin in which the infiltrate is usually much denser and regularly involves the subcutis. The granulomata are generally less well formed, and there is more lymphophagocytosis in the latter. The loss of elastic tissue is typically focal in granulomatous MF, and very prominent in granulomatous slack skin. However, histologic overlap may be seen and reliable distinction relies on clinical correlation.11,29
Granulomatous inflammation has been described as a feature in a range of other cutaneous lymphomas, and these must also be considered in the differential diagnosis. These include subcutaneous panniculitic T-cell lymphoma, Sézary syndrome, small/medium pleomorphic T-cell lymphoproliferative disorder, primary cutaneous anaplastic (CD30+) large cell lymphoma, angioimmunoblastic T-cell lymphoma (AITL), peripheral T-cell lymphoma
Clinical features Syringotropism in MF is a very rare occurrence, usually manifesting as small papules arising in a background of patch or plaque stage disease. Less often, it may present de novo.1–12 It most frequently accompanies the folliculotropic variant of MF.3,7,8,12,13
The so-called syringolymphoid hyperplasia presenting with localized alopecia and anhidrosis is likely to represent a form of syringotropic T-cell lymphoma.1,2 In rare cases, biopsies show subtle changes with no evidence of lymphoid atypia, and these patients should be monitored carefully with repeat biopsies for evidence of lymphoma.8,9
Syringotropism in MF is seen most frequently in males (12 : 5).12 In general, lesions are localized, presenting as erythematous or brown patches and plaques with superimposed papules, often accompanied by localized hair loss (Fig. 29.64).10,12 Ulceration and scarring are not uncommon. Hypoesthesia and anhidrosis may be seen.1–3,5 Because of the deep-seated
1424 Cutaneous lymphoproliferative diseases and related disorders
nature of the infiltrate, response to skin directed therapies may be poor and localized radiotherapy required.12
Histologic features Lesions are characterized by dense lymphoid infiltrates surrounding and infiltrating the sweat gland and ductal epithelium (Figs 29.65–29.67). In those patients in whom a diagnosis of lymphoma is apparent, there are conspicuous atypical lymphoid cells with enlarged, irregular, and hyperchromatic nuclei. The sweat gland epithelium may be hyperplastic, and frequently the lumen is obliterated (Fig. 29.68). Follicular mucinosis or folliculotropic MF is sometimes present and in those lesions arising in a background of typical MF, an atypical superficial dermal infiltrate with epidermotropism is seen.
was accompanied by a storiform spindle cell proliferation.2 Clinically, the latter lesions were reminiscent of scleromyxedema.2 Whether this represents a genuine variant or coincident expression of two disorders is uncertain.
The lymphocytes express CD2, CD3, CD4, and CD45RO.4,6 Loss of CD7 has been documented.5,10 Keratin immunohistochemistry can be of value in highlighting destroyed sweat gland epithelium. TCR gene rearrangements assists in making the diagnosis.5,8,12

Fig. 29.64 Syringotropic mycosis fungoides: distinct papules are present on this patient’s arm. By courtesy of H. Naeem, MD, Harvard Medical School, Boston, USA.
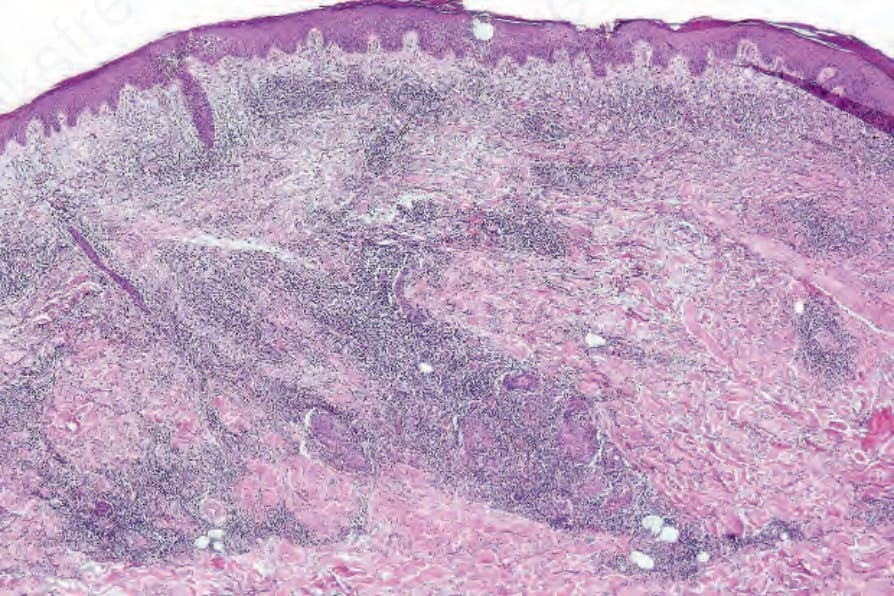
Fig. 29.65 Syringotropic mycosis fungoides: low-power view showing a distinctly nodular lymphoid infiltrate.
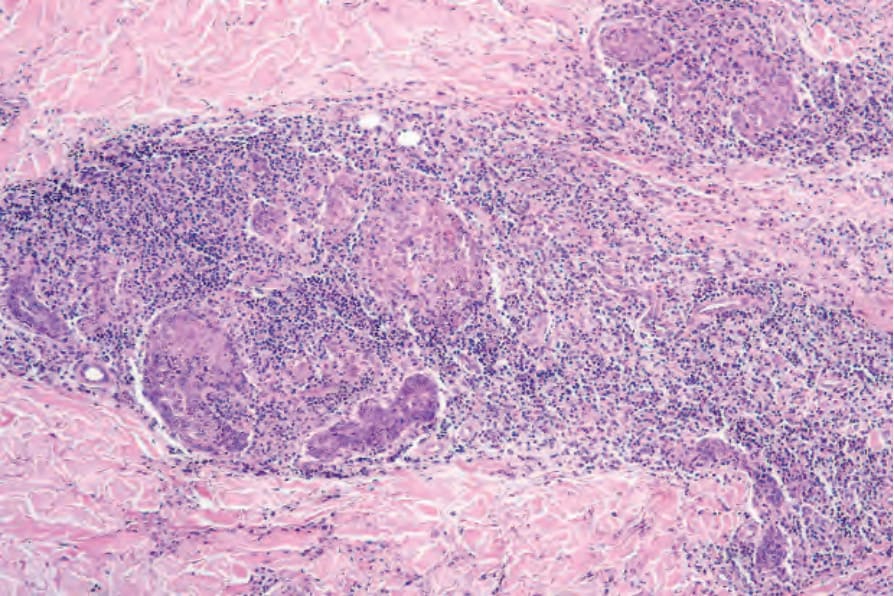
Fig. 29.66 Syringotropic mycosis fungoides: the infiltrate is centered on hyperplastic sweat glands.
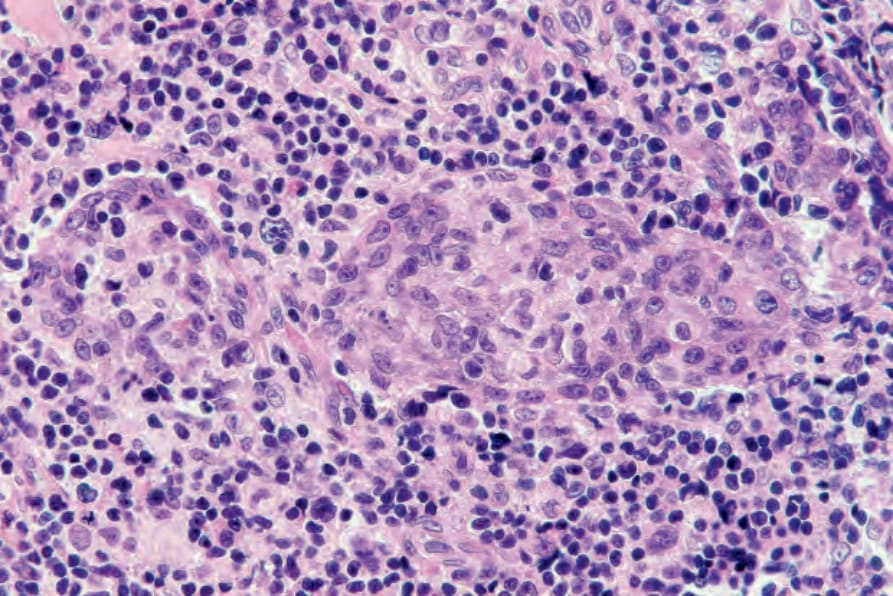
Fig. 29.67 Syringotropic mycosis fungoides: the lymphocytes have infiltrated the sweat gland epithelium.
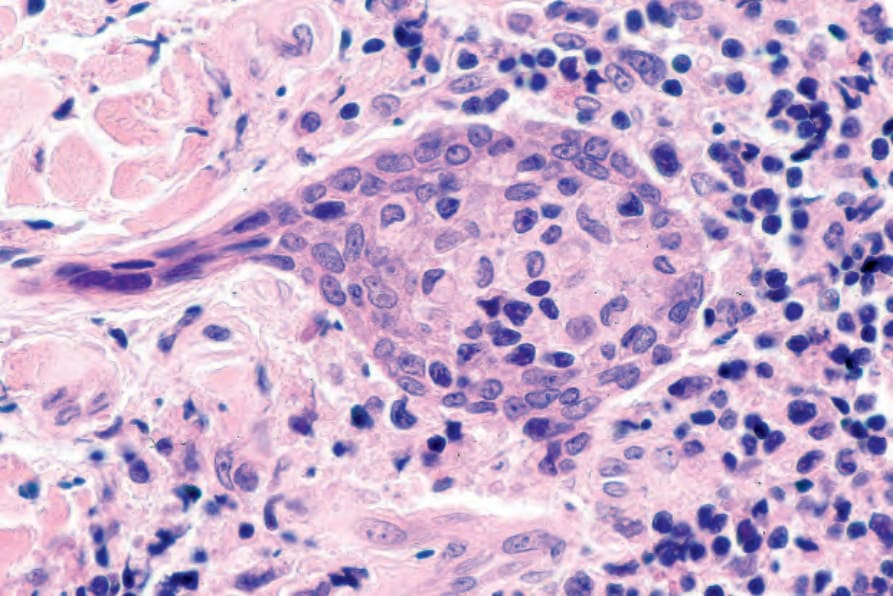
Fig. 29.68 Syringotropic mycosis fungoides: in this field, there is marked hyperplasia of the sweat gland epithelium.