Vesiculobullous mycosis fungoides
Vesiculobullous mycosis fungoides
Clinical features Bullous MF is exceptional. Lesions, which may resemble bullous pemphigoid, pemphigus vulgaris, or pemphigus foliaceus, can be generalized, although in some reports there is a predilection for the palms and soles.1–9 Superimposed allergic contact dermatitis following topical therapy may give rise to spongiotic vesiculation.
Histologic features The blisters may be subcorneal, intraepidermal, or subepidermal, although the last are most common (Fig. 29.54).6 They develop as a result of tumor cell infiltration with possible cytokine release rather than as a consequence of a coexistent autoimmune bullous dermatosis. Immunofluorescence is invariably negative.2,4,5
Differential diagnosis Gram stain and periodic acid-Schiff (PAS) should be performed to exclude secondary infection. Vesiculobullous mycosis fungoides must be distinguished from bullous pemphigoid arising in patients with pre-existent mycosis fungoides and sometimes complicating PUVA, ultraviolet (UV) B therapy, or other treatments such as topical methchlorethamine and interferon (IFN)-alpha.10–13
Hyperpigmented lesions have been characterized by marked elongation of the rete ridges with increased pigmentation and conspicuous dermal melanophages superimposed upon the changes of MF.23,26

Fig. 29.53 Hypopigmented mycosis fungoides: patches of variable sizes, some of which appear infiltrated. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
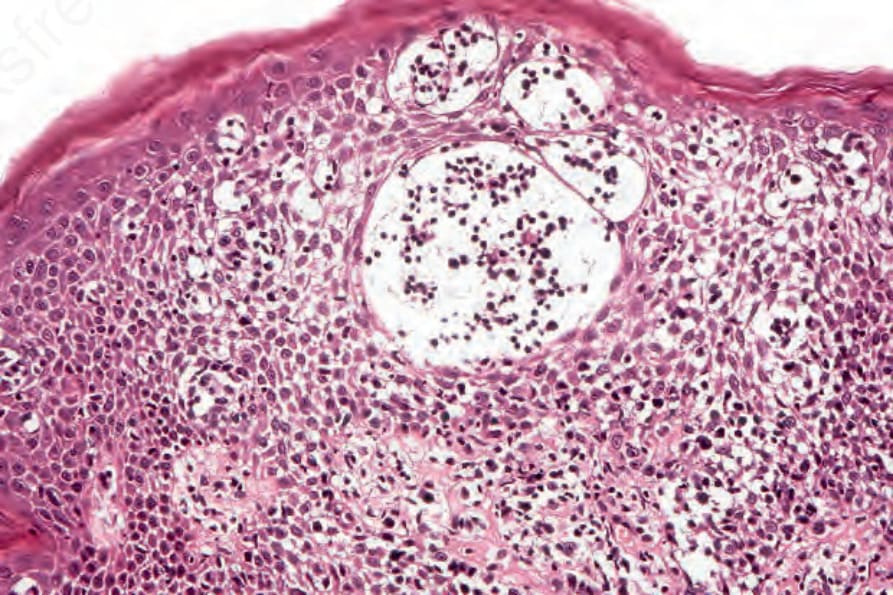
Fig. 29.54 Vesiculobullous mycosis fungoides: intraepidermal spongiotic vesiculation. This may reflect an allergic response to topical treatment. Atypical lymphocytes are present.