Conjunctival nevus
Conjunctival nevus
Clinical features Conjunctival nevus is the most common melanocytic tumor of the conjunctiva, comprising 23% to 29% of conjunctival tumors in several large series.1,2 Conjunctival nevi may be divided into congenital (appearing within the first 6 months of life) or acquired (appearing more than 6 months after birth) types.
In one large series of 410 conjunctival nevi,2 the mean age is 32 years with a wide range of 2–93 years. The majority of patients are Caucasian, and there is equal sex predilection. Most lesions are located on the bulbar conjunctiva (72%) (Figs 27.26–27.28), caruncle (15%), or plica semilunaris (11%). Nevi are rarely found in the fornix, tarsal conjunctiva, or within the cornea; therefore, pigmented lesions in these areas should raise suspicion for PAM or melanoma. Conjunctival nevus most commonly develops near the limbus.1,2 The most common clinical presentation is the appearance of a spot on the eye. Pain is very rare.
nevi are found only early in life and have nests of nevus cells along the interface of the epithelium and substantia propria. Junctional nevus cells generally have abundant cytoplasm. As intraepithelial nevus cells begin dropping off into the substantia propria, dragging surface epithelium with them, nevus cells and intraepithelial inclusions expand the substantia propria. The nevus becomes thicker clinically. A nevus with cells in the epithelium and substantia propria is a compound nevus (Fig. 27.29). The intraepithelial component of a compound nevus should not extend much beyond the lateral edges of the subepithelial component. The presence of melanocytes individually or in nests far beyond the lateral margins of the subepithelial component should raise suspicion for intraepithelial atypical melanocytic hyperplasia, also known as PAM with atypia, which is a precursor lesion for melanoma. Over time, the nevus may become disconnected from the overlying epithelium and reside completely in the substantia propria. This type of nevus is designated as subepithelial nevus (Fig. 27.30) and is analogous to intradermal nevus of the skin. Compared with intraepithelial nevus cells, those in the substantia propria generally have less cytoplasm, especially toward the base, which reflects maturation. Some nevus cells may contain intranuclear cytoplasmic inclusions. Binucleated and multinucleated cells may be identified, and are
Clinically, the tumor is most commonly brown, and less often tan or nonpigmented. Intralesional cysts are present in the majority of lesions. Feeder vessels and intrinsic vessels, which may be prominent in conjunctival melanoma, can be seen in approximately one-third of cases.2
Histologic features Histologically, conjunctival nevi are described as junctional, compound, or subepithelial, which may be considered as stages of evolution.1 Junctional
1374 Tumors of the conjunctiva
is composed of fascicles of spindle nevus cells that are usually oriented perpendicular to the surface and are uniformly and symmetrically arranged. Mitotic figures or brisk expression of MIB-12 in Spitz nevi reflect rapid clinical growth and do not indicate malignancy.

Fig. 27.26 Conjunctival nevus: there is a pigmented lesion on the superior bulbar conjunctiva. Note the cysts within the lesion.
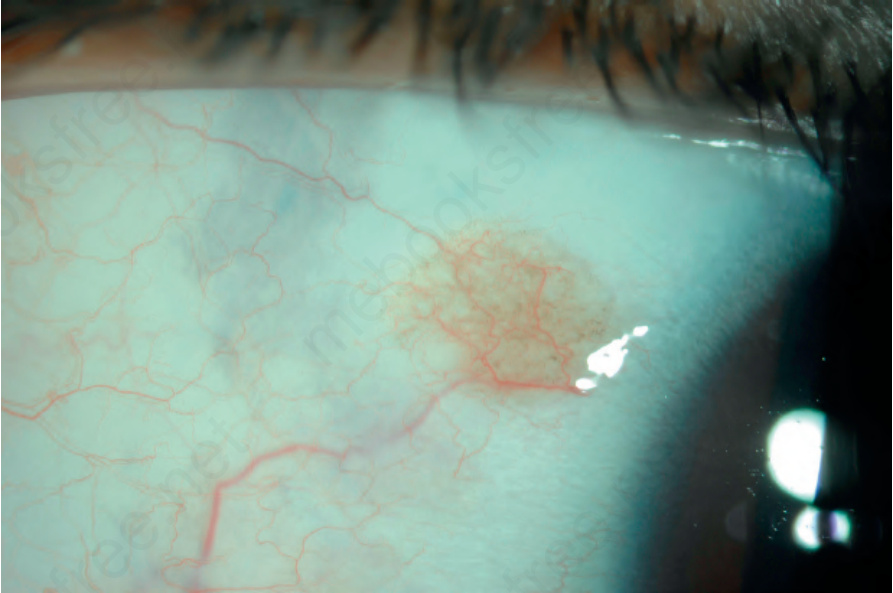
Fig. 27.28 Conjunctival nevus: a circumscribed, lightly pigmented lesion with intralesional cysts is on the bulbar conjunctiva.
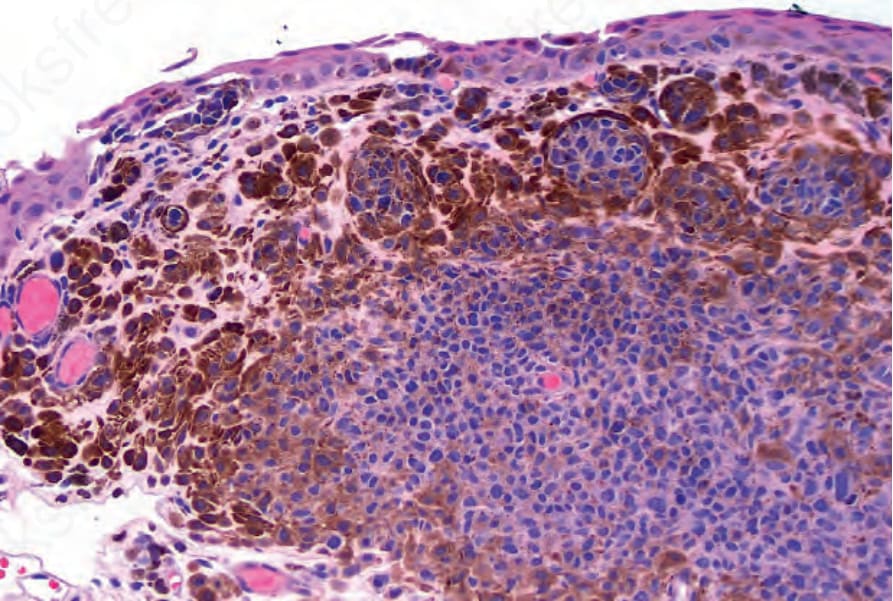
Fig. 27.29 Compound nevus: junctional nests and involvement of the substantia propria is evident.
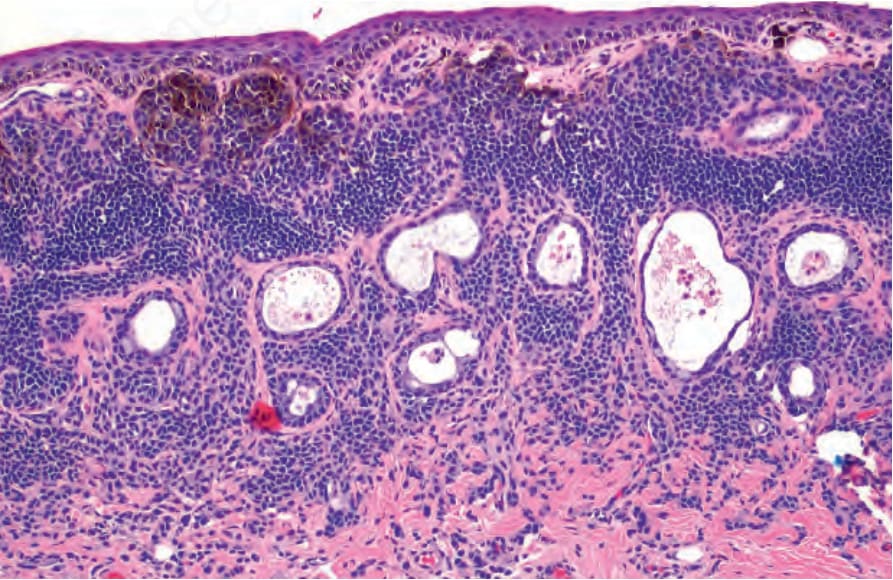
Fig. 27.30 Subepithelial nevus: nevus cells are present in the substantia propria without junctional nests. Epithelial cysts are present within the lesion. Note how there is increased melanin pigmentation of the superficial nevus cells compared to those toward the base.
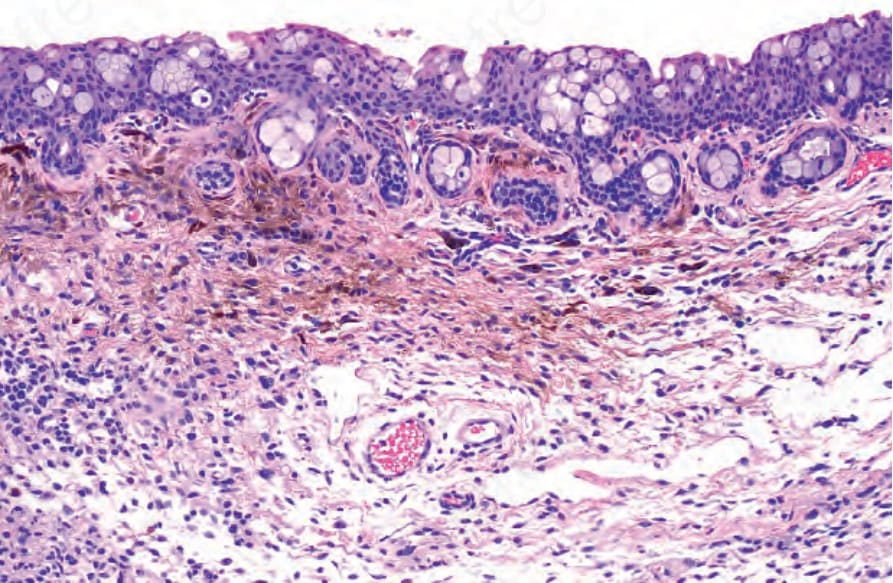
Fig. 27.31 Combined nevus: histology shows nests of common nevus cells and more pigmented spindle and dendritic cells.