Melanoma in children
Melanoma in children
Clinical features Melanoma is extremely rare in children; less than 1% of all melanomas present in childhood.1–20 Historically, many so-called examples have likely represented misdiagnosed Spitz nevi.13 As a consequence, pathologists and clinicians are extremely reluctant to make the diagnosis, with resultant delay in treatment and potentially devastating consequences. Although exceptionally the tumor may develop in utero (complicating a large congenital nevus or arising de novo) or be acquired transplacentally (from a maternal melanoma), the majority are acquired and may be related to sun exposure during childhood.4,14,21 Predisposing conditions include xeroderma pigmentosum, dysplastic nevi, familial melanoma, melanoma-pancreatic cancer syndrome, giant congenital nevi, neurocutaneous melanosis (leptomeningeal melanoma), prior irradiation, Li-Fraumeni syndrome, and immunodeficiency.3,4,14,22–27 Melanoma arises in up to 12% of giant congenital nevi (i.e., those that measure 20 cm or more in diameter) and this can occur during childhood or later adult life.28–30 It has been suggested that childhood melanoma can be segregated into three distinct categories based on the age of diagnosis: congenital melanoma which occurs in utero up to birth; infantile melanoma that presents after birth up to 1 year of age; and childhood melanoma that occurs after 1 year of age to puberty.31 Some include in the childhood melanoma category patients up to the age of 18, but such upper age ranges are clearly arbitrary.32
The sexes are affected equally and tumors are more common in the second than the first decade.9 The majority of childhood melanomas have developed in Caucasians.7 Lesions arise on the trunk and extremities, with only 20% affecting the head and neck.5 Many childhood melanomas are not easily recognized clinically.13,33 Sometimes, however, clinical features similar to those described in adults – including increase in size, change in color, and onset of bleeding – may be encountered.14,17
Some earlier reports suggested that the prognosis of melanoma in children might be favorable.34 In our experience, however, childhood tumors behave no differently from adult ones with the possible exception of spitzoid melanomas in very young patients as discussed further below. This is also generally borne out in the more recent literature.4–6,13,18,35–37 Overall, childhood melanoma should therefore be treated in much the same way as adult tumors and, when appropriate, sentinel lymph node mapping and biopsy are recommended.4,6,13,38–40 The majority of children present with stage 1 disease with a 5-year disease-free survival rate of 77%.4,7 Crude survival figures for the largest series reported to date are 71% overall, 64% males, 81% females.9 Some, but clearly not all or even most in some series, melanomas of childhood exhibit Spitz-like histology.41 These cases may have a more favorable outcome than in adults, particularly in patients aged 11 or less, but this finding is not universal.41–44 This could be due to inappropriate assignment of Spitz nevi, albeit atypical, to the melanoma group; however, even such tumors metastatic to lymph nodes appear to have a better prognosis.45,46 Clearly, more study is required. Nonetheless, mortality is encountered within this age group. Spitzoid melanoma is discussed in more detail in the section above.
Histologic features Melanoma in children may arise within the context of a precursor lesion such as a banal, congenital, or dysplastic nevus or it may present de novo. Melanoma arising within a giant congenital nevus presents most often as a dermal, sharply delineated nodule composed of tumor cells showing obvious cytological features of malignancy (Figs 26.116–26.118).30 Although all the common subtypes may be encountered, superficial spreading and nodular melanoma variants are most frequently seen (Figs 26.119–26.123). Particular subtypes that often cause diagnostic difficulty include small cell melanoma, spitzoid melanoma, and malignant blue nevus.7,11,47 These are all described under variants of melanoma (see above).
Cytogenetic features detected by FISH are similar to those seen in adult superficial spreading melanoma.48 BRAF mutations can be seen in freestanding cases while NRAS mutations are seen in the cases associated with congenital nevi.49,50 UV damage signatures are commonly encountered and
TERT promoter mutations are common, excepting the cases arising in congenital nevi.49
As with adult melanoma, the most important prognostic indicators are Breslow thickness and presence of ulceration. Melanoma in children should be reported in exactly the same way as adult melanoma.51
Differential diagnosis Clinicopathological correlation is of great importance when considering a diagnosis of melanoma in a child, particularly in the first few years of life. Significant cytological atypia affecting junctional and dermal components accompanied by pagetoid spread and mitotic activity is not uncommon in congenital nevi, especially those affecting neonates.
1351 Basomelanocytic tumor
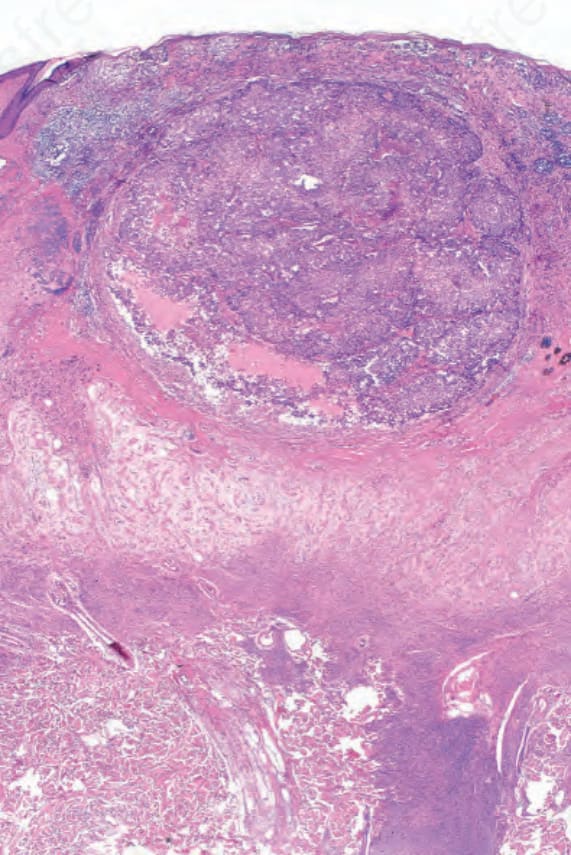
Fig. 26.116 Childhood melanoma: example of melanoma which has arisen in a giant congenital nevus.
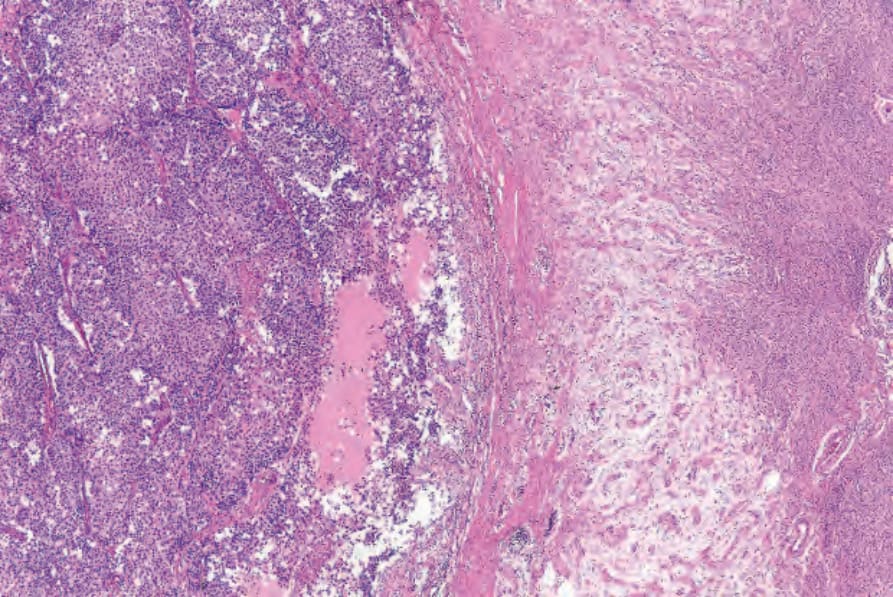
Fig. 26.117 Childhood melanoma: in this view, pleomorphic tumor cells are seen on the left; nevus is present on the right.
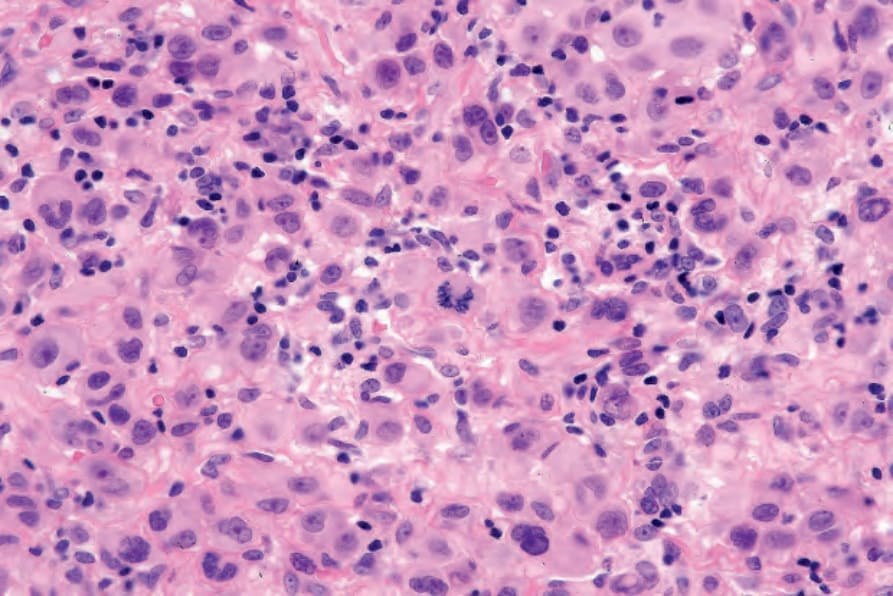
Fig. 26.118 Childhood melanoma: in the center of the field is an atypical mitotic figure.
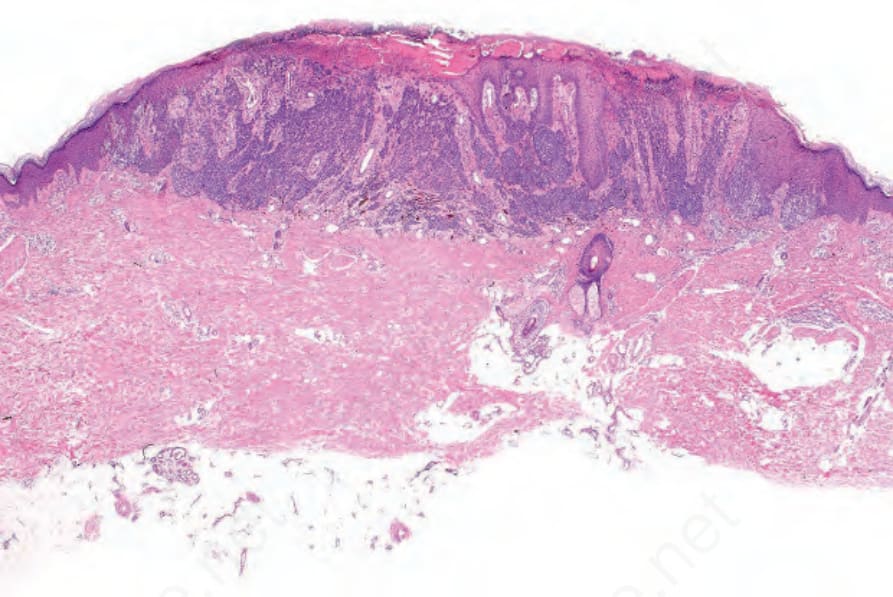
Fig. 26.119 Childhood melanoma: this tumor, which presented as a nodular lesion, arose in a girl aged 13 years. By courtesy of M. Little, MD, University College Hospital, Galway, Ireland.
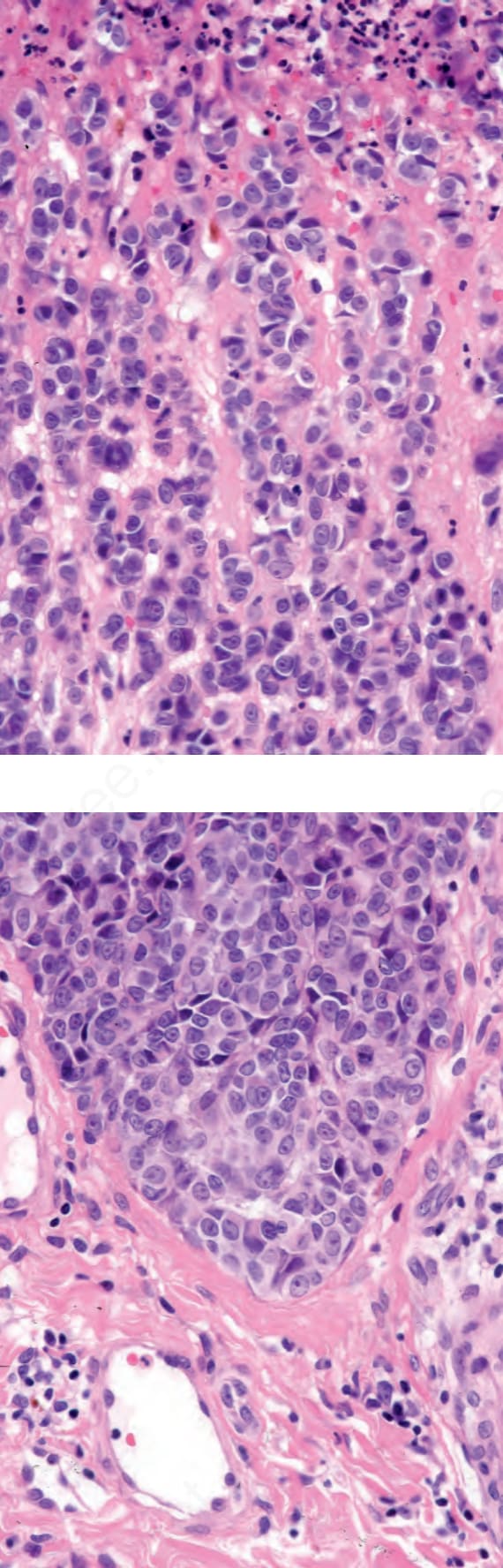
Fig. 26.120 Childhood melanoma: there is surface ulceration. By courtesy of M. Little, MD, University College Hospital, Galway, Ireland.