Desmoplastic and neurotropic melanoma — Part 2
Ultrastructural studies have shown that the tumor spindled cells may rarely contain premelanosomes and melanosomes.1,2 Fibroblastic, myofibroblastic, and Schwann cell differentiation, particularly in neurotropic variants (including elongated and interdigitating cellular processes sometimes encircling collagen fibers reminiscent of mesaxon formation, discontinuous basal lamina, and intercellular junctions) have also been documented.19,71,80–83
The genome of desmoplastic melanoma harbors approximately an order of magnitude more mutations than that seen in conventional cutaneous melanoma.84 Most of these are UV-linked. Exome sequencing revealed recurrent NFKBIE promoter mutations, and activation of the MAP kinase and PI-3 kinase pathways through mutations in genes such as NF1, MAP2K1, MAP3K1, EGFR, MET, RAC1, and PIK3CA.84–88 Mutations in BRAF V600 and NRAS G61 were not seen. TERT promoter mutations are common as well.89 Standard multi-probe FISH can be useful to demonstrate desmoplastic melanoma over other mimics.90
been documented.50 Metaplastic bone formation has been described albeit rarely.51 Sarcomatoid dedifferentiation is also rarely noted.49
Immunohistochemically, desmoplastic melanoma expresses S100 protein (94–100%), neuron-specific enolase, and vimentin (Fig. 26.115).3,36–38,40,41 HMB-45 (gp100) may be positive in the superficial papillary dermal tumor cells but more often is totally negative.52–57 The results with MART-1 (melan-A) are variable (24–60% positive), and tyrosinase does not appear to be present in desmoplastic melanoma.58–60 Microphthalmia transcription factor (D5) is of limited value, expression having been documented in from only 35% to 55% of cases.61,62 A relatively new marker, SOX10, is reactive in melanoma, desmoplastic melanoma, and peripheral nerve sheath tumors and can be a very useful marker.63–66 Members of the S100 protein family such as S100A6 may have efficacy in distinguishing desmoplastic melanoma from malignant peripheral nerve sheath tumors, but the diffuse pattern of traditional polyclonal S100 protein expression in melanoma is usually sufficient in this regard.67 Melanoma cell adhesion molecule may be more useful, 82% of tumors in a series of 17 tumors having shown strong expression.68 EMA may be present in up to 43% of tumors but keratin, leu 7, CD31, and CD34 are uniformly negative.48,55,56,68 Smooth muscle actin is often positive, reflecting the myofibroblastic population.55,56,69 Although occasional desmin
Differential diagnosis The diagnosis of desmoplastic melanoma is frequently missed, particularly if only superficial biopsies are available for study. The lesion is commonly misdiagnosed as a reactive process, such as scarring and superficial nodular fasciitis, and deeper lesions may be mistaken for a fibromatosis or even fibrosarcoma. Examples showing storiform morphology have sometimes been confused with atypical fibrous histiocytoma and dermatofibrosarcoma protuberans. Scar tissue may be a particular problem, especially in recurrent lesions.91,92 Pointers towards the latter include horizontal orientation of the fibroblast population, absence of adnexae, loss of the rete-ridge pattern, and vertically orientated dermal blood vessels. Immature scar tissue, however, can be much more problematical and, in the case of re-excision specimens or recurrences, the features may represent an admixture of both.92 Recurrent lesions following surgery may sometimes be associated with marked nerve proliferation in addition to scar tissue. SOX10 and S100 may display positivity in scars and although this positivity can be strong it is usually restricted to a small number of cells.93
Diagnosis is dependent upon an awareness of the condition and often requires the inclusion of a battery of immunohistochemical markers to establish the histogenesis of the tumor infiltrate. In many instances, however, careful scrutiny of the epidermis to detect atypical melanocytic hyperplasia combined with the use of antibodies to S100 protein and pankeratin (to exclude desmoplastic spindled cell squamous carcinoma) will be sufficient to establish the correct diagnosis. Occasionally, in recurrent disease, proliferating neural elements may be admixed with scar and residual tumor with resultant increased diagnostic difficulty. Neurofilament protein, which is expressed by the neural elements but not the melanomatous component, can often be of discriminatory value.
1350 Melanoma
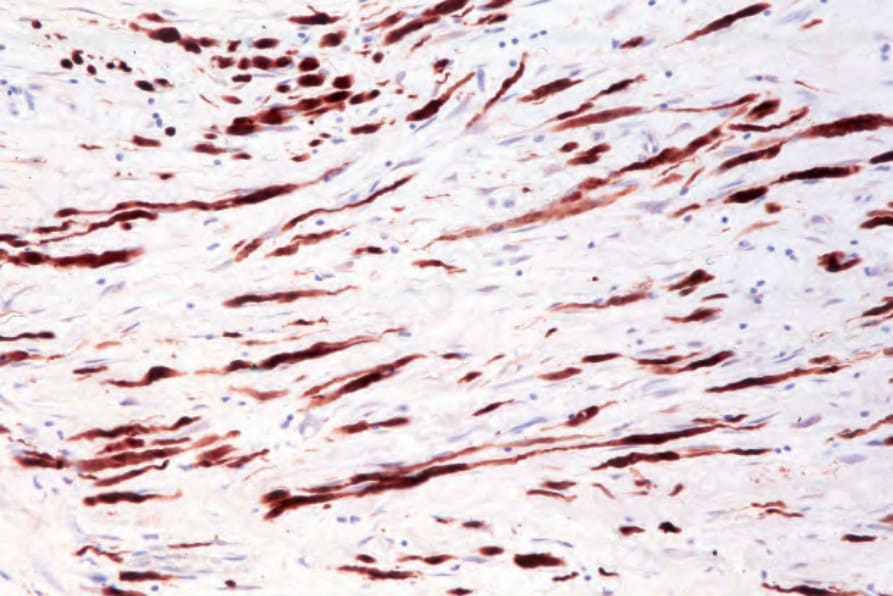
Fig. 26.115 Desmoplastic melanoma: the tumor cells are strongly S100 protein positive.