Epidermotropic metastatic melanoma
Epidermotropic metastatic melanoma
Metastatic melanoma is common and, in the majority of cases, causes little diagnostic difficulty. Rarely, however, cutaneous deposits are accompanied by epidermal involvement such that distinction from a second or third primary tumor can be extremely difficult, if not impossible, particularly if clinical information is not available (Figs 26.95 and 26.96).1–9 Traditionally, the features in favor of epidermotropic metastatic disease have included a well-circumscribed dermal nodule, widespread lymphovascular invasion, and filling of the papillary dermis by melanoma cells with atrophy of the overlying epidermis.1,10 Typically, the epidermal component is equal in width to, or is less than, the dermal component. A lateral epidermal collarette may sometimes be present. Exceptionally, patients have presented with showers of metastases which, due to extensive lateral spread of the epidermal component beyond the dermal mass or even wholly intraepidermal disease, have histologically been indistinguishable from a primary tumor. In such instances, clinicopathological correlation is essential in establishing a diagnosis of metastatic disease.2,3 A recent study with molecular testing suggests that the genetic relationship of primary melanomas and their potential epidermotropic metastases is complex, with certain cases showing divergent loss of heterozygosity and X-chromosome inactivation patterns consistent with either complex divergent clones or possibly new primaries.11 Additional study is essential as the distinction has important staging implications. Epidermotropic melanoma is a satellite lesion that results in stage III groupings under the 8th edition AJCC, whereas a second primary would be individually staged.12
This is an unusual tumor, which shows some histologic overlap with other dermal dendrocytoses and blue nevus-like melanoma. These lesions form part of the spectrum of pigmented epithelioid melanocytoma, which includes the epithelioid blue nevus associated with the Carney complex and
1344 Melanoma
B
A
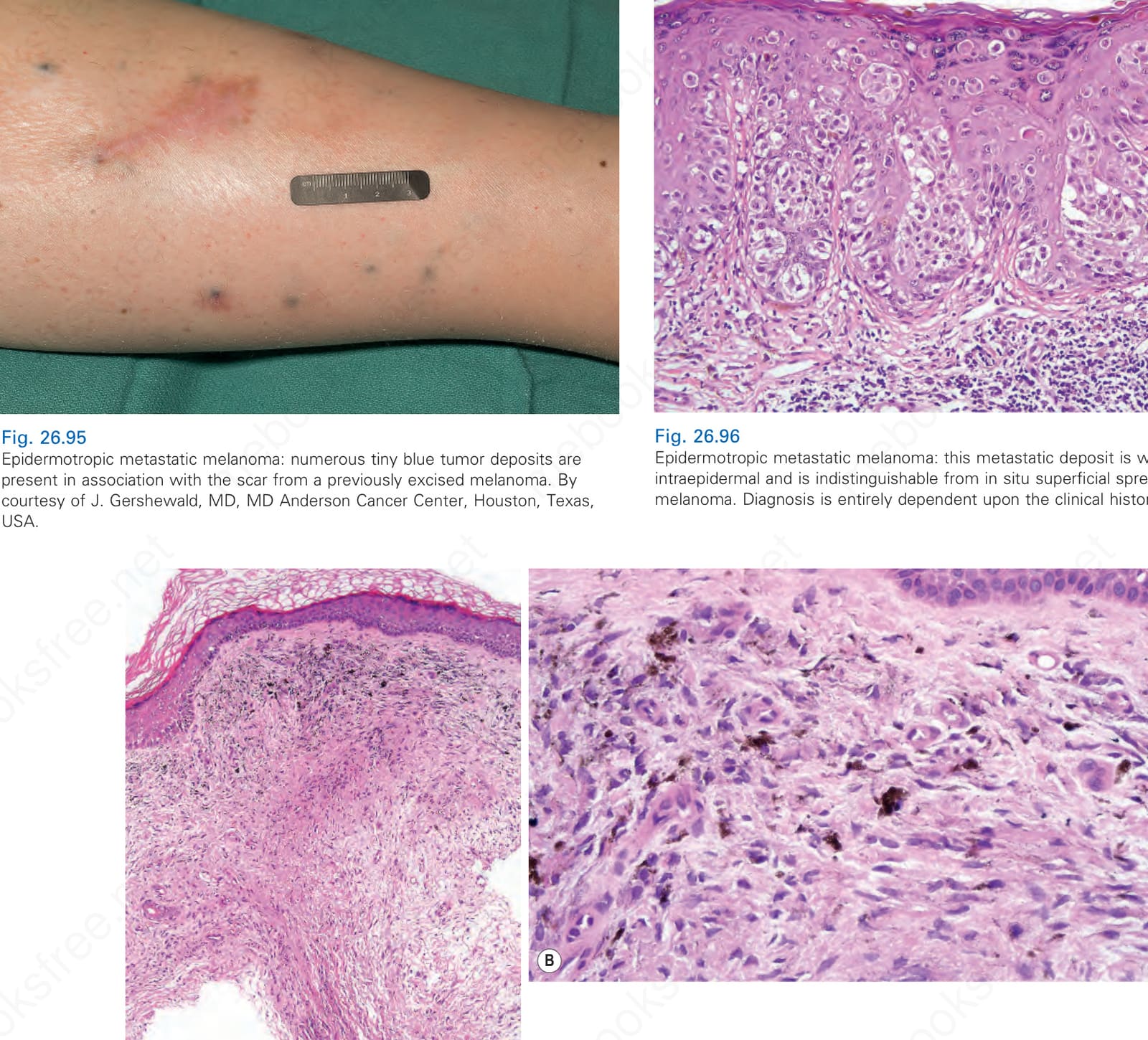
Fig. 26.95 Epidermotropic metastatic melanoma: numerous tiny blue tumor deposits are present in association with the scar from a previously excised melanoma. By courtesy of J. Gershewald, MD, MD Anderson Cancer Center, Houston, Texas, USA.
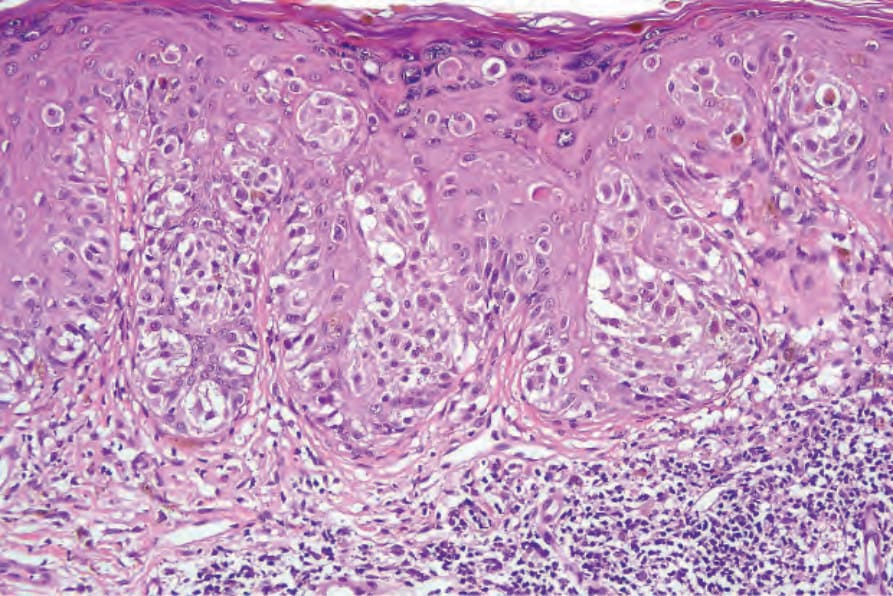
Fig. 26.96 Epidermotropic metastatic melanoma: this metastatic deposit is wholly intraepidermal and is indistinguishable from in situ superficial spreading melanoma. Diagnosis is entirely dependent upon the clinical history.
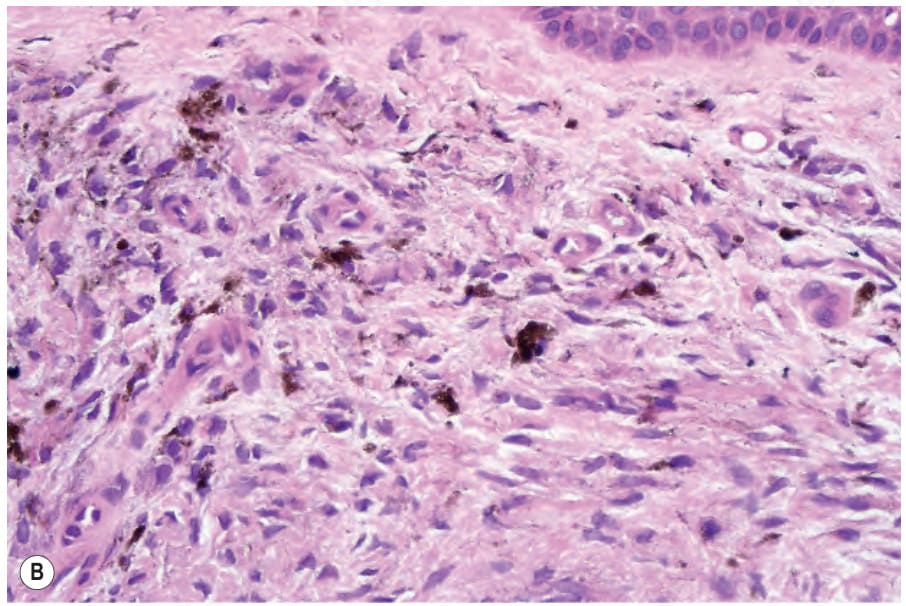
Fig. 26.97 Blue nevus-like metastatic melanoma: (A) at low-power examination, the features could easily be mistaken for a common blue nevus; (B) in addition to pigment-laden melanophages and dendritic cells, there are scattered melanoma cells. Note the multinucleate form with vesicular nuclei and prominent nucleoli. The patient had a melanoma previously excised at this site.