Angiotropic and angiomatoid (pseudovascular) melanoma
Angiotropic and angiomatoid (pseudovascular) melanoma
cases.14,15 Angiotropism can also be seen in nevi, particularly congenital melanocytic nevi.16
Exceptionally, melanoma may show blood-filled dilated spaces lined by endothelium-like tumor cells reminiscent of angiosarcoma (angiomatoid melanoma).17–22 Intraluminal tufting may result in pseudoglomeruloid structures.18
Angiotropism has been described in only a few cases of vertical growth phase melanoma.1–5
Histologically, this rare manifestation of melanoma is characterized by the growth of melanoma cells within or along the walls of vessels, principally veins, but usually without showing evidence of intravascular invasion.1,6 While a relatively rare occurrence, interobserver concordance is high when standardized diagnostic criteria are applied.7 More recently, this phenomenon has been suggested as a type of vascular invasion and shown to be associated with a poor prognosis, perhaps even brain metastases in some cases.8,9 It is also independently correlated with the presence of microsatellites in primary cutaneous melanoma.10 Some contend that this pericytic association may represent an extravascular mechanism for local or regional metastasis.11,12 Angiotropism has also been described in epidermotropic and other metastatic melanomas.13 A recent mouse model study indicated that inflammation induced by UV exposure can promote angiotropism and proposed this as a means of metastasis also relevant to humans in some
Metaplastic melanoma (melanoma with heterologous differentiation)
Exceptionally, melanoma is associated with heterologous metaplastic elements, including bone and cartilage.1–6 Mostly, these have complicated acral lentiginous lesions (particularly arising in a subungual location) although examples have also been described in primary desmoplastic melanoma, mucosal melanoma, and melanoma arising in a congenital nevus.6,7 It can also be seen in metastatic melanoma, both with or without being present in the cognate primary lesion.8,9 From the limited available literature, these tumors are high grade (due to thickness at presentation) with frequent metastases and considerable mortality. Histologically, they usually present as sarcomatoid lesions with osteoid and to a lesser extent chondroblastic differentiation (Figs 26.89 and 26.90). A number of these cases represent osteosarcomatous differentiation, i.e., osteoid deposition in association with malignant cells, and/or chondrosarcomatous differentiation.10,11 Too few cases have been reported to be certain whether heterologous differentiation
1342 Melanoma
under the name of pigmented epithelioid melanocytoma. There is certainly morphological overlap with malignant blue nevus, but genomically these two entities are distinct and we believe that they represent independent histologic entities based on this and differences in their natural history. The original term of animal-type melanoma was coined to reflect the similarity of these tumors to melanocytic lesions occurring in horses and a variety of experimental animal models – so-called equine melanotic disease.1,2 This is a condition in which aging gray horses lose their pigmentation and develop melanocytic tumors particularly around the external genitalia, undersurface of tail, breast, and lip mucosa. Subsequent development of melanoma in these animals is an important complication.
Clinical features Around 200 cases of this seemingly rare tumor have been documented, mostly as single case reports.3 Although the age range is quite wide, the majority of lesions have arisen in patients in the second to fourth decades.4–7 There is no recognized sex or site predilection. Most present as 1.0 cm or more diameter, brown, blue-black or black nodules or plaques clinically thought to represent melanoma.8 These tumors can occur sporadically or as part of the autosomal dominant Carney complex where these tumors have traditionally been termed epithelioid blue nevus.9 Carney complex consists of spotty skin pigmentation, and a variety of unusual endocrine and non-endocrine tumors such as myxomas, pigmented nodular adrenocortical disease, calcifying Sertoli cell tumor and psammomatous melanotic schwannomas. This complex is associated with germline inactivating mutations in the protein kinase A regulatory subunit, PRKAR1A on chromosome 17q.10,11 The unrelated Carney triad is a distinct condition comprised of gastrointestinal stromal tumor, pulmonary chondroma, and extra-adrenal paraganglioma driven by succinate dehydrogenase (SDH) definiciency.12,13
influences prognosis. Certain properties of mesenchymal stem or precursor cells suggest a pluripotency that includes neural crest, osteogenic, and chondrogenic potential and may help explain the existence of this melanoma variant.12 Some cases have been shown to express immunohistochemical markers of master regulatory genes for osseous and cartilaginous differentiation such as SATB2 and SOX9.6,9
Unusually, melanoma may undergo smooth muscle and rhabdomyoblastic differentiation.13–16 Case reports of melanoma showing ganglionic and ganglioneuroblastic differentiation have been documented.17–19
There are very occasional reports of conventional and desmoplastic melanoma containing osteoclast-like giant cells (Fig. 26.91).20–25
Rhabdomyosarcoma has been documented in a congenital nevus, including a giant form.26–28
Pigmented epithelioid melanocytoma (pigment synthesizing melanoma; animal-type melanoma)
An enigmatic lesion with many names, including pigment synthesizing melanoma, animal-type melanoma, melanoma with prominent pigment synthesis, equine type melanoma, and low-grade hypermelanotic dermal melanoma, this exceedingly rare variant of melanoma is now recognized by the WHO
Prognosis seems to be better than that of an ordinary melanoma of equivalent thickness and it has been proposed that it may be regarded as a low-grade variant of melanoma. A recent meta-analysis of around 190 cases seems to confirm this notion, but that study was hampered by limited follow-up for the reported cases and the lack of uniform diagnostic criteria.3 Nonetheless, this study showed that with a median Breslow thickness of 3.8 mm and 16% ulceration, there were only six patients with distant metastases and five patient deaths. Sentinel lymph node positivity rates were notable at 41% of the 78 patients undergoing this procedure, but subsequent progression was uncommon. Thus this tumor has a markedly superior prognosis to conventional melanoma.
Histologic features Pigmented epithelioid melanocytoma is characterized histologically by a very dense infiltrate of heavily pigmented melanocytes, typically filling the
1343 Histologic variants of melanoma
tumors previously termed pigment synthesizing melanoma.14–16 While these lesions appear to have metastatic potential to involve lymph nodes, their outcome is favorable compared to stage-matched cases of traditional melanoma.3 More and longer-term study of this entity and the above-mentioned spectrum will be insightful.
Loss-of-function mutations in PRKAR1A are common. Gene fusions with PRKCA encoding protein kinase Cα can also be seen in pure melanoma.17 In cases of combined nevi with conventional features and an area resembling pigmented epithelioid melanoma, BRAF V600 mutations can be seen with the PRKAR1A mutations. Cases with characteristic activating GNAQ or GNA11 mutations would be better regarded as blue nevus or blue nevus-like melanoma rather than pigmented epithelioid melanocytoma. Use of the standard multi-color FISH assay to assess for malignancy in pigmented epithelioid melanocytoma has been reported as helpful in a few cases, but should be interpreted with caution given the alternative genetics of this tumor.18,19
papillary and reticular dermis and often spilling over into the subcutaneous fat (Fig. 26.92). The epidermis may be atrophic or hyperplastic. A small number of cases are not purely intradermal but display a junctional component (Fig. 26.93). In cases with a junctional component, tumor cells are plump and dendritic and do not tend to exhibit pagetoid spread. Tumor cells are spindled, polygonal, or rounded and are distributed in a fascicular or nodular growth pattern, sometimes displaying a focal storiform appearance.6 Dendritic processes may be identified. The tumor cell cytoplasm typically contains abundant fine to coarse melanin granules, which commonly obscure the nuclear morphology. Examination of bleached sections can be helpful. The cytoplasm of tumor cells is pale, and nuclei appear enlarged and sometimes hyperchromatic. A single prominent basophilic nucleolus is often seen. Although there is cytological atypia, tumor cells display little variation throughout the tumor (Fig. 26.94).6 Mitoses are typically sparse. The latter and the uniformity of tumor cells allow distinction from malignant blue nevus. Perineural infiltration may be present but lymphovascular invasion has not been described.
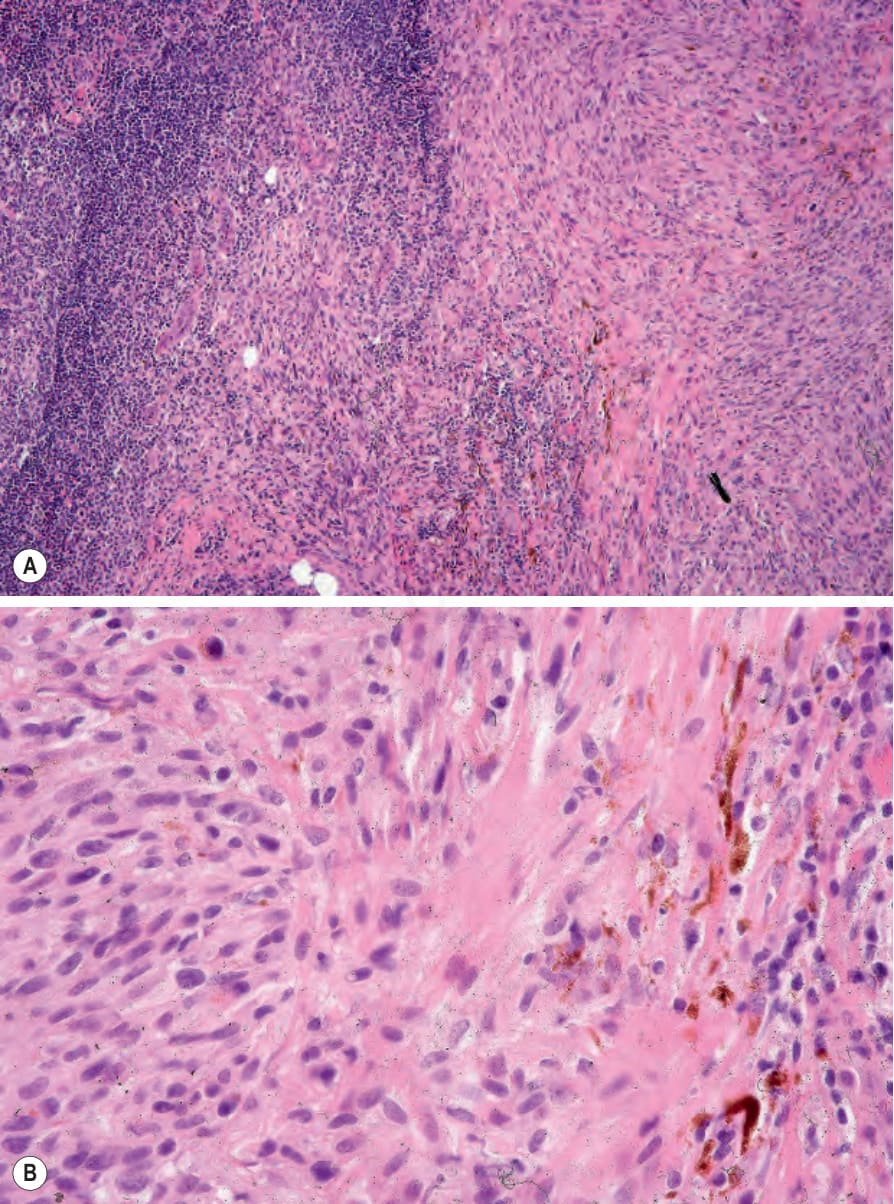
Fig. 26.88 (A, B) Malignant blue nevus: the sentinel node contained metastatic melanoma. A small number of dendritic cells are present. This is the same case as illustrated in Figures 26.81–26.84.
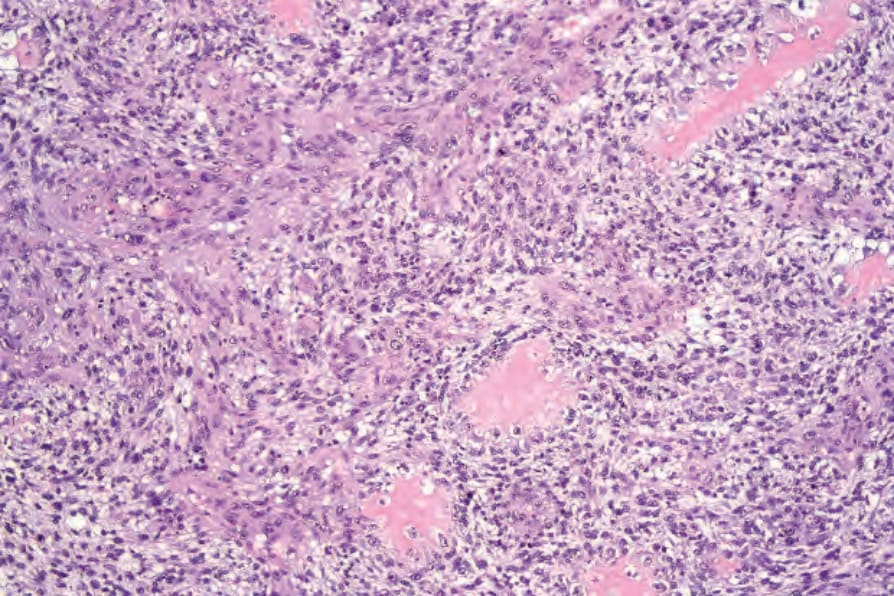
Fig. 26.89 Metaplastic melanoma: multiple deposits of osteoid are present in association with malignant cells in this amelanotic melanoma.
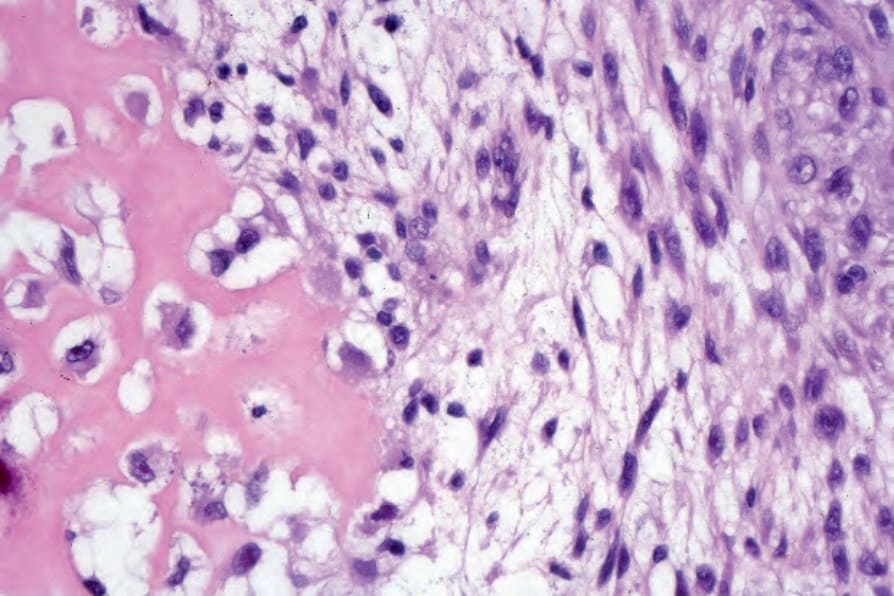
Fig. 26.90 Metaplastic melanoma: high-power view.
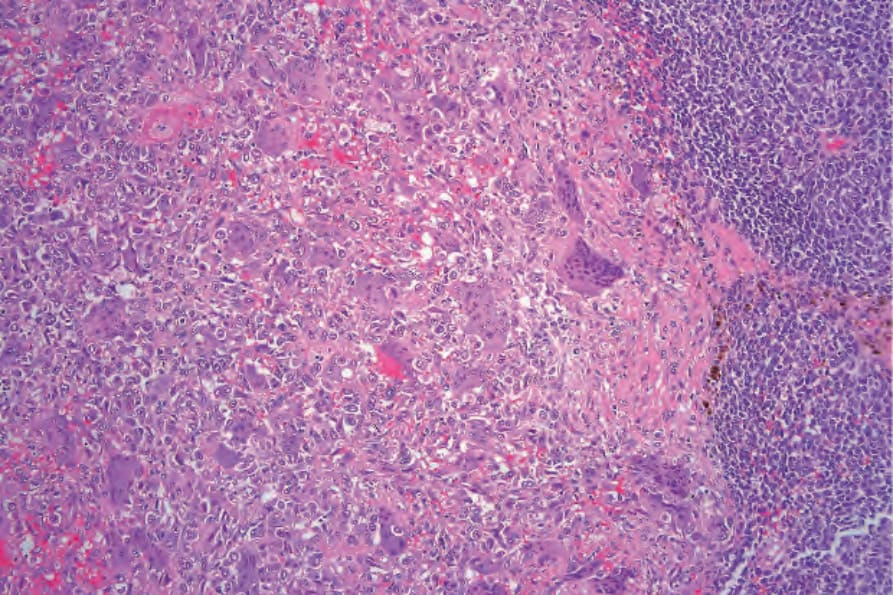
Fig. 26.91 Metaplastic melanoma: this melanoma was associated with an intense osteoclastlike giant cell infiltrate.
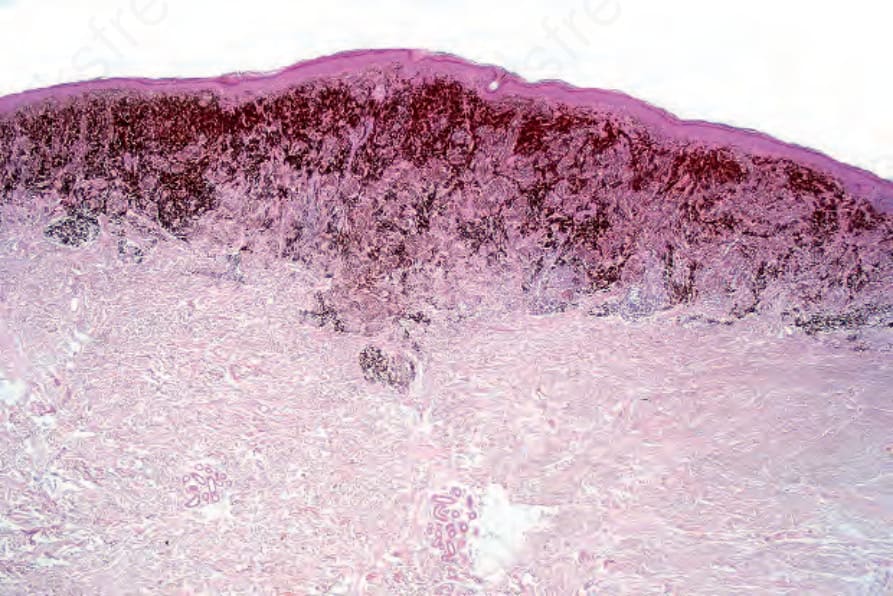
Fig. 26.92 Pigment synthesizing melanoma: this low-power view shows the intense pigmentation typical of this variant.
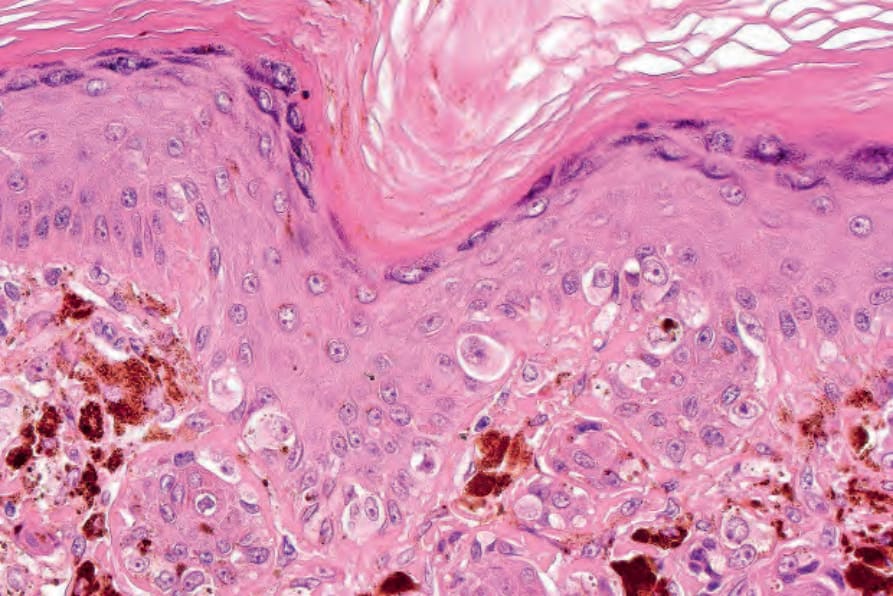
Fig. 26.93 Pigment synthesizing melanoma: scattered tumor cells are present in the lower epidermis.
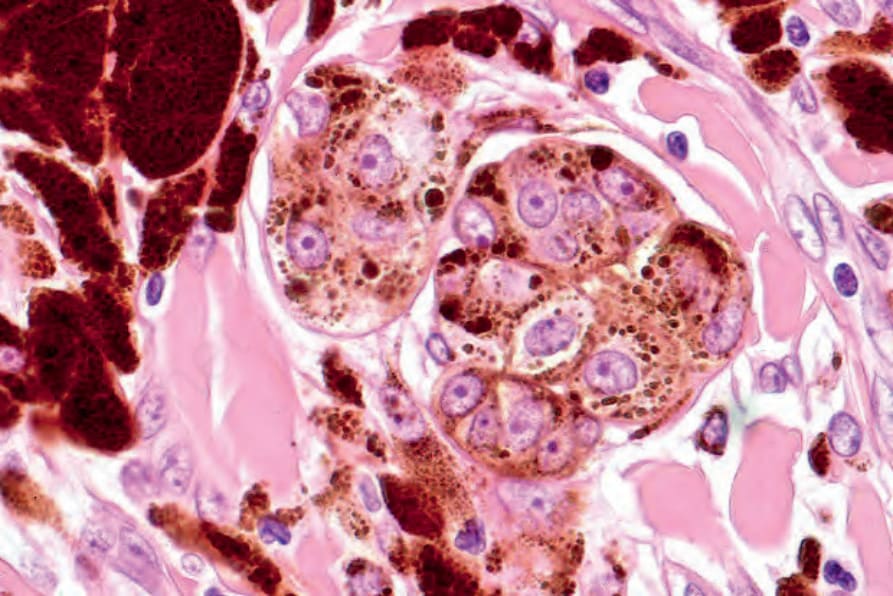
Fig. 26.94 Pigment synthesizing melanoma: the tumor cells are uniform with large vesicular nuclei and prominent eosinophilic nucleoli. Abundant pigment-laden macrophages are present.