Spitzoid melanoma
Spitzoid melanoma
The diagnosis of Spitz nevus, and in particular its distinction from melanoma, is one of the most difficult areas in dermatopathology.1–3 Spitz nevus is predominantly a lesion of children and young adults, whereas melanoma occurs most often in the middle aged and elderly. There is therefore a tendency when encountering a spitzoid lesion in a child to automatically try to categorize it in the benign group merely on the basis of the age.4 Overreliance on age is a dangerous practice, since although rare, melanoma occurring in childhood and showing spitzoid features has been well documented
1335 Histologic variants of melanoma
B
A
B
A
may be tainted with Spitz nevi containing unusual features. The descriptions in the literature and use of these categories highlight the diagnostic difficulties presented by Spitz nevi and spitzoid melanoma.
Mones and Ackerman20 have emphasized involvement of the deep dermis or subcutaneous fat by a vertically orientated tumor showing only mild asymmetry on scanning magnification. Other clues include uneven melanin distribution, often at the base of the tumor, variability in size and shape of the dermal nests and fascicles, confluence of nests and fascicles to form diffuse sheets of tumor cells, and diminution or loss of adnexae. They also make the point that the superficial features can be virtually indistinguishable from Spitz nevus. Consumption of the overlying epidermis is a helpful
feature pointing to melanoma as opposed to Spitz nevus when present, though some question its usefulness.21,26,27 It is important to emphasize that this feature is useful when the thinning of the epidermis is continuous but usually not when it is focal.
Immunohistochemistry may be of value. Thus 50% or more of tumor cells in spitzoid melanoma may express proliferating cell nuclear antigen (PCNA) whereas in Spitz nevus, usually less than 5% of cells are positive.28 A similar staining pattern is noted with MIB-1 where less than 2% strongly favors nevus and greater than 10% strongly favors melanoma with others factors impinging more strongly between these two thresholds.29,30 HMB-45 expression in the deep dermal component would favor a diagnosis
1336 Melanoma
of spitzoid melanoma.29,31 Amplification of the p-arm of chromosome 11 where the HRAS oncogene resides is seen in a subset of Spitz nevi; this change is not encountered in melanoma and thus this finding may be helpful in distinguishing Spitz nevi and melanoma.32–35 Comparative genomic hybridization and FISH assays can be used to make this determination. The distinction between Spitz tumor and atypical Spitz tumor is not always well informed by such assays, but can be helpful when characteristic melanoma deficits are present.36,37 As for spitzoid melanoma, 6p25 and/or 11q13 gains or 9p21 deletions on FISH favor malignancy while no FISH abnormality or 6q23 deletions are associated with less aggressive behavior or benignancy.38 Spitzoid melanomas generally lack mutations in genes such as BRAF and NRAS common in some other melanoma subtypes in some studies, but not others.39,40 This may illustrate the difficulty in histologically defining what amounts to a spitzoid melanoma versus a standard melanoma. Spitz lesions can also show inactivation of the tumor suppressor BAP1 (BRAF V600 mutations can also be seen with BAP1 loss) as well as rearrangements in ALK, RET, ROS, BRAF, NTRK1, and RET. These features can be seen in both benign and malignant Spitz tumors.38,41–48
change in recurrent and primary disease. The phenomenon does not have prognostic significance.1–15
Signet ring cell change is characterized by a large pale or eosinophilic cytoplasmic globular inclusion or vacuole, which compresses the nucleus to the edge of the cell (Fig. 26.71). This appearance may affect a melanoma in part or constitute the whole of the lesion. The periodic acid-Schiff (PAS) stain is variably weakly positive (diastase resistant) but an Alcian blue reaction is consistently negative.1,2,11 The nature of the PAS-positive material is unknown. The signet ring appearance is due to excess intermediate filament presenting as an intracytoplasmic ‘mass’ or vacuole.
The signet ring cells contain vimentin and may express S100 protein and HMB-45 although the latter two can be patchily distributed and occasionally absent altogether.2,4,16 Diagnosis in such a case is then dependent upon finding more typical melanoma cells with appropriate immunocytochemistry elsewhere in the specimen. Signet ring cell melanoma must be distinguished from other signet ring cell tumors, particularly mucin-containing adenocarcinoma and lymphoma. To this end, antibodies to LCA, keratin, EMA, and CEA should invariably be included in the immunocytochemistry panel.
Although Smith and coworkers10 suggested that malignant Spitz nevus might represent a tumor that rarely spread beyond the draining lymph nodes, subsequent papers have suggested that the tumor is often no different from any other melanoma and therefore has the same risk of systemic spread and an identical mortality.15,28,49 Spitz-like lesions that metastasize to lymph nodes in children do appear to be less aggressive than traditional melanoma in children and adults. Metastasis of Spitzoid lesions in adults appears to bear the same prognosis as that of other metastasizing melanoma. Some authors recommend sentinel lymph node biopsy in problematical spitzoid lesions to help establish a diagnosis of melanoma in addition to adding prognostic information, though this approach is not without controversy.19,50–56 Patients younger than 11 years of age with spitzoid melanoma may have a better prognosis than older adolescents and adults, but this finding has not been universal.49,56
Cytological diagnosis of signet ring cell melanoma (by fine needle aspiration and from a peritoneal effusion) has been documented.8,10
Signet ring cells have also exceptionally been described in banal and Spitz melanocytic nevi.6,17,18
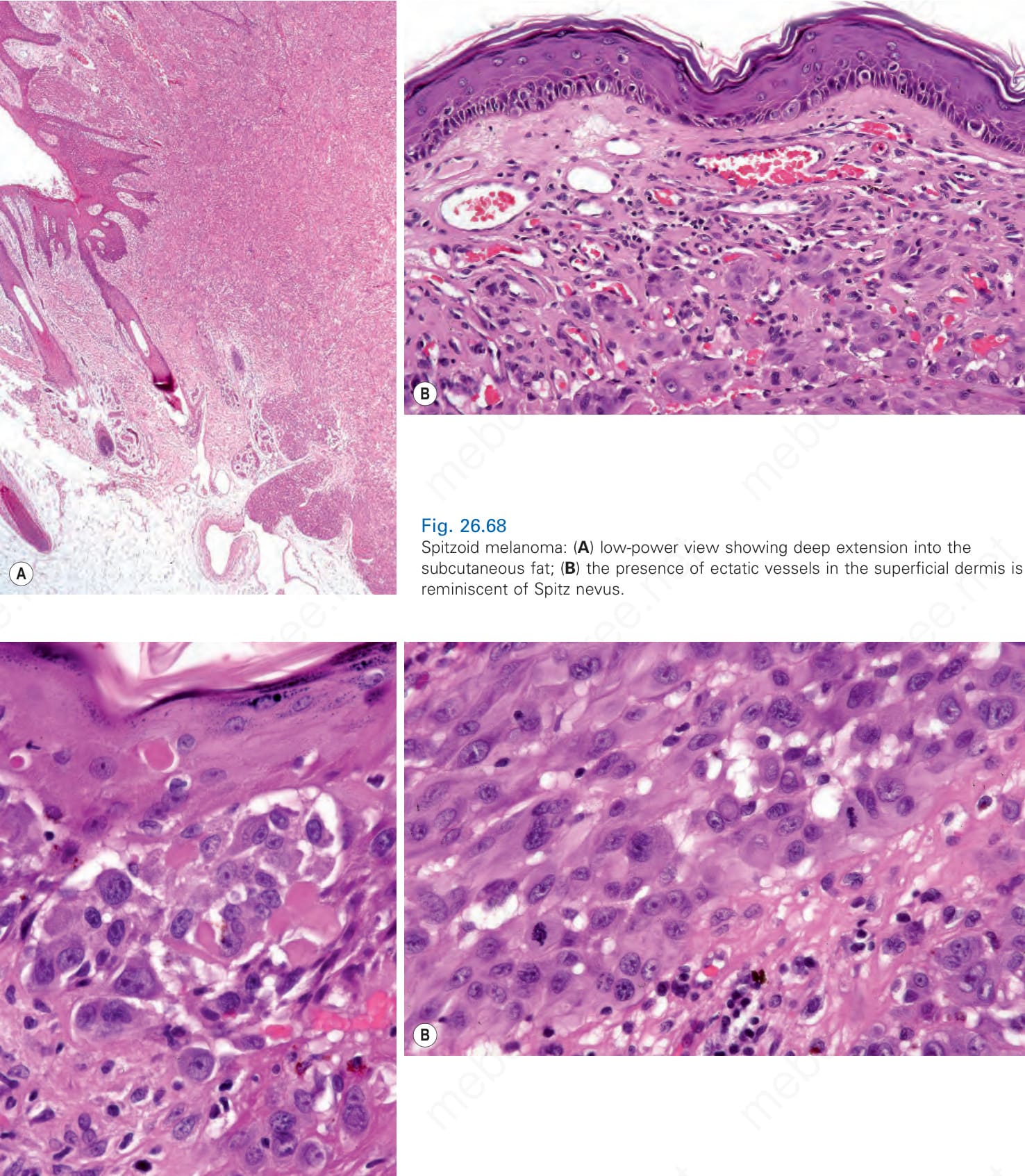
Fig. 26.68 Spitzoid melanoma: (A) low-power view showing deep extension into the subcutaneous fat; (B) the presence of ectatic vessels in the superficial dermis is reminiscent of Spitz nevus.
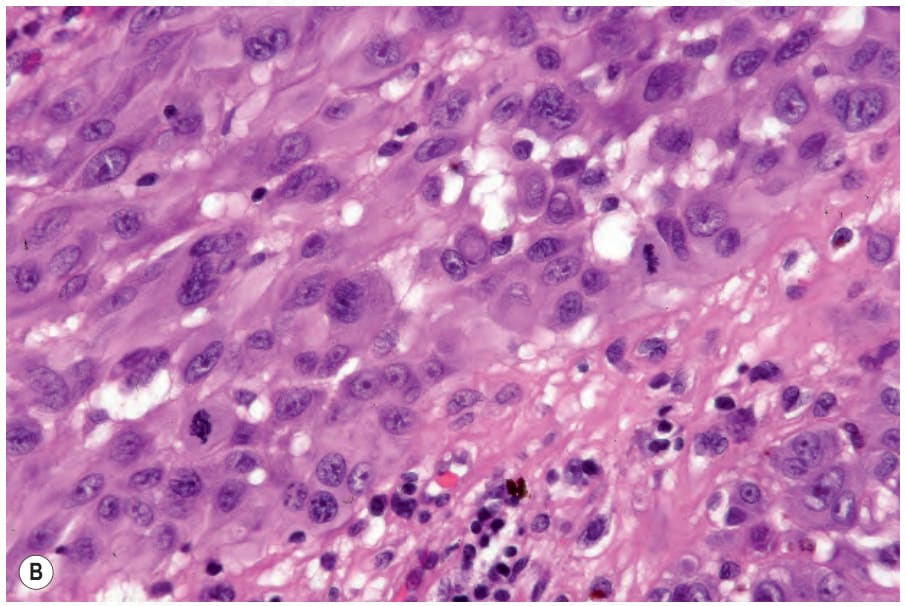
Fig. 26.69 Spitzoid melanoma: (A) multiple Kamino bodies may also mislead the unwary; (B) multiple mitoses, however, should raise a high index of suspicion.
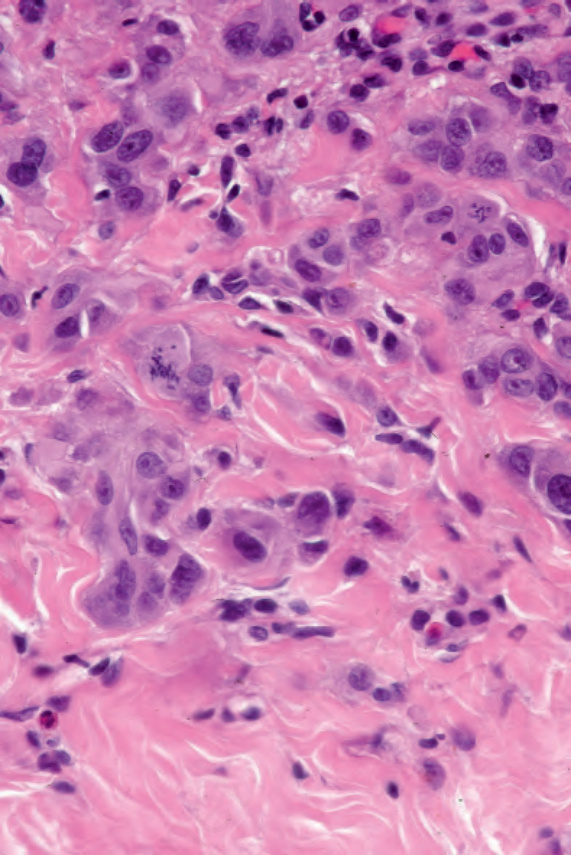
Fig. 26.70 Spitzoid melanoma: deep or abnormal forms are important diagnostic features and are absolute indicators of an unequivocal diagnosis of melanoma. Note that there is no evidence of maturation.
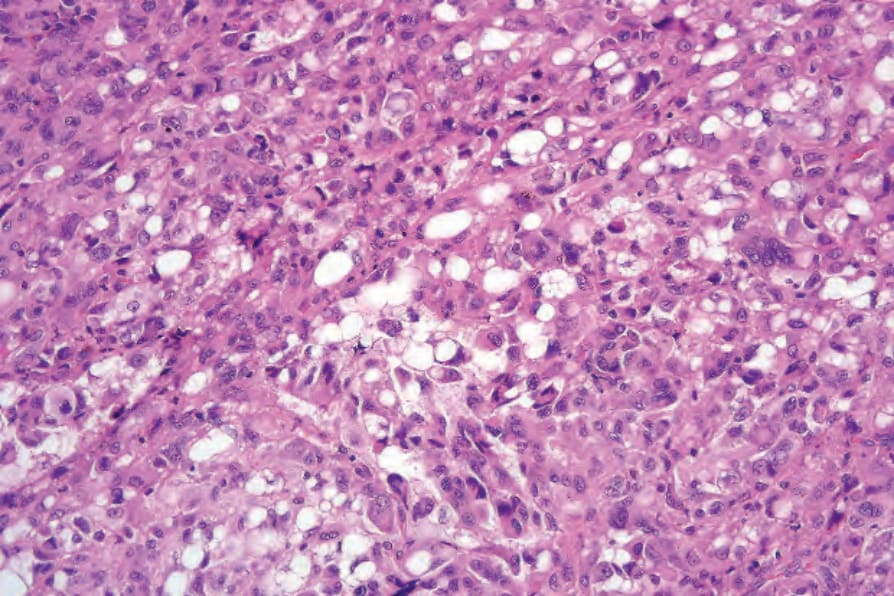
Fig. 26.71 Signet ring cell melanoma: very occasional signet ring melanoma cells are not uncommonly seen in epithelioid melanomas; exceptionally, however, they can constitute the majority of the tumor.