Small cell melanoma
Small cell melanoma
The term ‘small cell melanoma’ is often a source of confusion.1–3 In the literature it has been applied to a variety of different lesions. It has been used as a synonym for nevoid melanoma as defined above.4,5 It has also been utilized in the context of a high-grade variant of childhood melanoma. Such tumors, which present on the scalp or developing in a congenital nevus, are highly aggressive.6,7 Other authors have employed the term to describe a tumor occurring in adults, which mimics lymphoma, cutaneous neuroendocrine carcinoma, or metastatic undifferentiated carcinoma.8–11 It has been used in the Australian and UK literature to describe a low-grade variant of melanoma arising on the sun-damaged skin of middle-aged males.12,13 A recent study indicates that a small cell component in cutaneous melanoma is a independent poor prognostic indicator.14
in the literature. This being said, age is a revealing variable with most Spitz-like features in young children being benign, but the same features in adults, particularly older adults, are much more likely to be associated with malignancy.5,6 There have thus been a number of papers describing melanomas with features reminiscent of Spitz nevus (spitzoid melanoma, malignant Spitz nevus) and diagnostic criteria to afford their distinction have been proposed and extensively discussed.7–20 Agreement between expert dermatopathologists in assessing malignancy in atypical spitzoid melanocytic tumors is quite poor.21 Agreement on what should be considered spitzoid or Spitz-like is also suboptimal.22 Given this uncertainty, treatment recommendations from pathologists can show considerable variance.22
Features that may favor a diagnosis of spitzoid melanoma include large size, deep dermal penetration, parakeratosis, epidermal atrophy (as opposed to the marked hyperplasia typical of Spitz nevus), asymmetry and lack of circumscription, pagetoid spread at the edge of the lesion (pagetoid spread in the center of the nevus is quite common in a Spitz nevus), absence of Kamino (eosinophilic) bodies, dusty pigmentation, dermal nests larger than the junctional ones, a diffuse (non-nested) dermal component, an expansile rather than infiltrating lower border, lack of maturation, nuclear pleomorphism and hyperchromatism, conspicuous mitoses, deep mitoses, and atypical mitoses (Figs 26.68–26.70).7,9,15,23 In a meta-analysis, Walsh and coworkers15 found the following to be the most useful and consistently applied criteria:
• symmetry,
• uniformity of nests from side to side,
• Kamino bodies,
• brisk mitotic rate,
• mitoses close to the base of the lesion,
• abnormal mitoses. A recent study by 13 experts of 75 cases confirmed the usefulness of all these factors excepting Kamino bodies and adding ulceration as a feature favoring malignancy.21 Thus the presence of the first three and absence of the second three argue for a diagnosis of Spitz nevus and vice versa. Spatz and coworkers16 have devised a grading system for dividing atypical Spitz nevi into low-, medium-, and high-risk categories (of being frankly malignant). This is based on age, diameter, involvement of subcutaneous fat, presence or absence of ulceration, and mitotic rate. The category of atypical Spitz with uncertain biological (or malignant) potential has also been much discussed.24,25 This concept is often applied to spitzoid lesions as many diagnosticians find these tumors challenging to definitively categorize as wholly benign or malignant in a subset of cases. Cases in this category may not represent neoplasms with the full biological potential of standard melanoma; however, this category
In our view, small cell melanoma should be distinguished from nevoid melanoma. We reserve the term for a high-grade melanoma, presenting as a small blue cell tumor reminiscent of type-B nevus cells. It is characterized by a monotonous population of cells with minimal cytoplasm and round to oval hyperchromatic nuclei, often containing prominent nucleoli (Figs 26.66 and 26.67). Mitoses are frequently conspicuous and karyorrhexis is common. The tumor cells are sometimes aggregated into elongated expansile nests but may also present as a diffusely sheeted infiltrate.15 Maturation with depth is not apparent. A pseudorosette pattern has been documented.15
In recurrent tumors where junctional activity is no longer apparent, and in metastatic disease, small cell melanoma can be easily confused with a poorly differentiated carcinoma, a lymphomatous infiltrate, and neuroendocrine carcinoma.8–10,16 Appropriate immunocytochemistry should readily solve the problem.
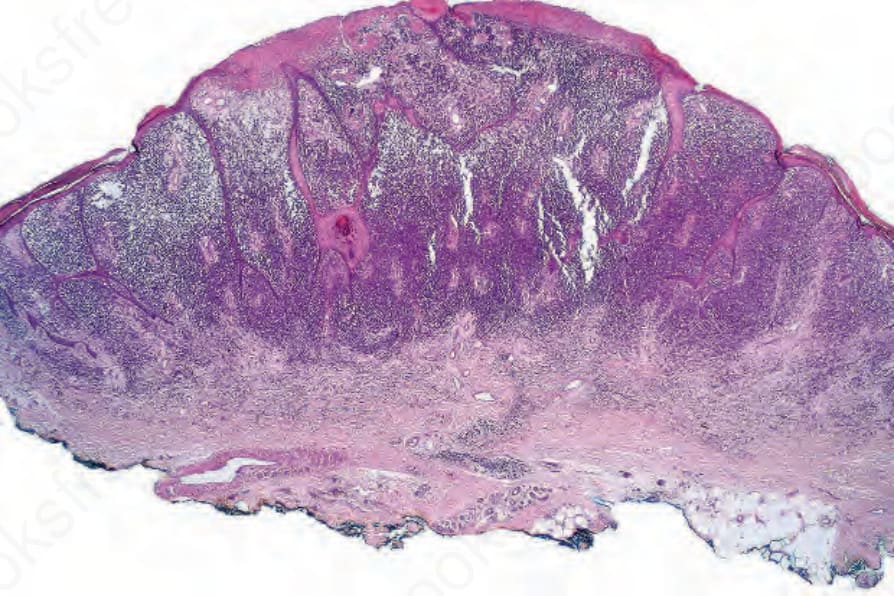
Fig. 26.66 Small cell melanoma: this variant of melanoma simulates type-B nevus cells at low-power magnification, the tumor cells being small and deeply basophilic.
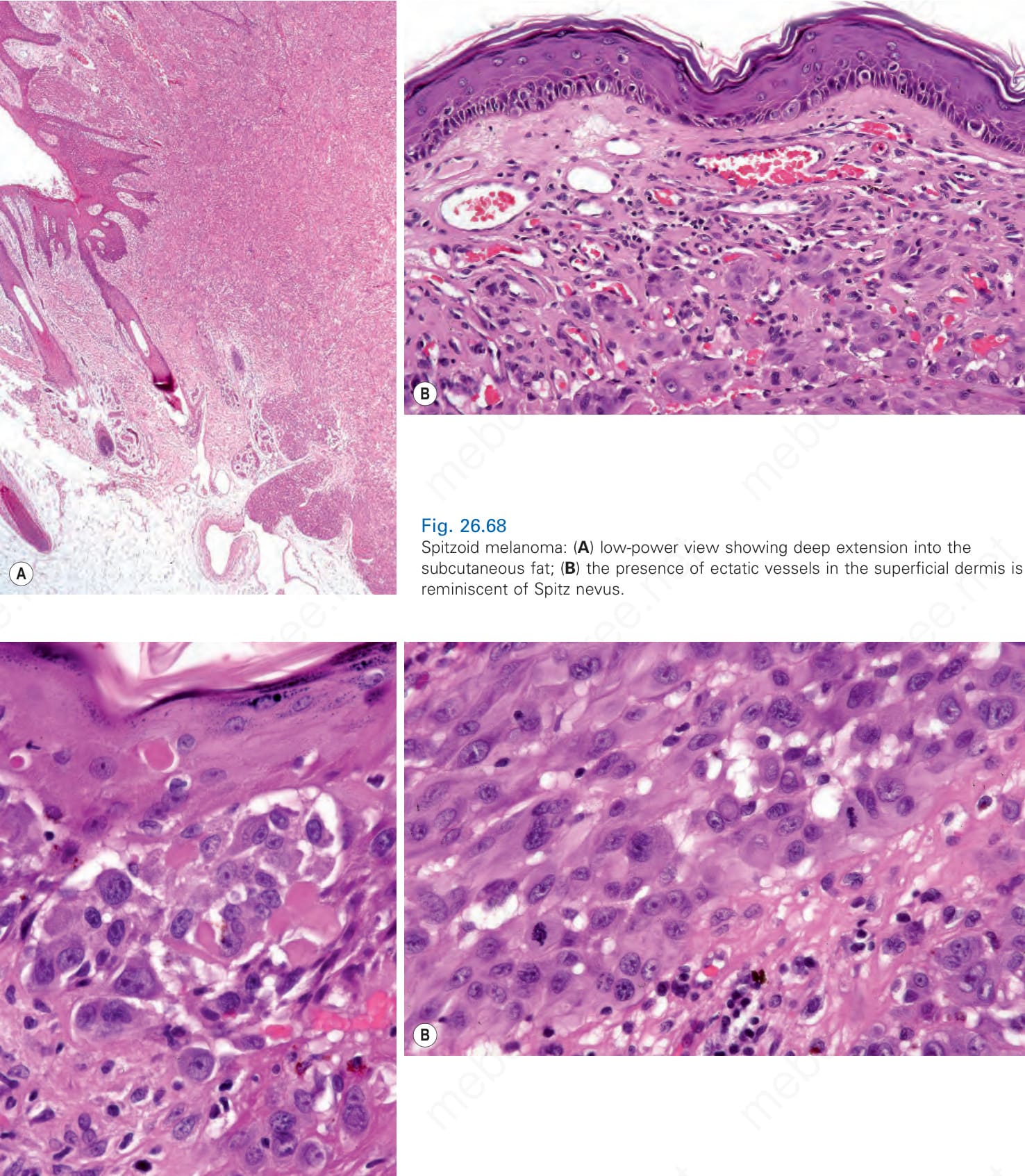
Fig. 26.68 Spitzoid melanoma: (A) low-power view showing deep extension into the subcutaneous fat; (B) the presence of ectatic vessels in the superficial dermis is reminiscent of Spitz nevus.