Nevoid melanoma
Nevoid melanoma
Nevoid melanoma is a rare histologic subtype of vertical growth phase melanoma, which on low-power inspection may be (and often is) confused with a banal melanocytic nevus.1–5 It can be equally challenging to recognize clinically on patient skin examinations as well.6 Diagnosis depends on a high index of suspicion and careful attention to cytological detail including a thorough search for dermal mitotic activity. A practical or functional definition of nevoid melanoma is the ‘diagnosis of a nevus which one later regrets’.
Because nevoid melanoma is commonly misdiagnosed as a banal nevus, subsequent delay in appropriate treatment is common, with potentially devastating consequences.1,2,7–12 Confusion with a banal nevus is most probably a reflection of too cursory an inspection of a ‘nevus,’ frequently at scanning magnification. Grossly, there are no particular distinguishing features, most lesions being clinically described as verrucous to dome-shaped variably pigmented nevi or non-specific papules or nodules. Follow-up information indicates a recurrence rate of 50%, a metastasis rate of 25–50%, and a mortality rate of at least 25%.12
Histologically, on low-power examination nevoid melanoma may present as a warty/verrucous or dome-shaped lesion (the former pattern in an elderly patient is itself a clue to the diagnosis, as nevi in the elderly are more often dome-shaped papulonodules) (Figs 26.57 and 26.58).
The verrucous variant has a rather characteristic histologic appearance presenting as an often asymmetrical, poorly circumscribed, warty lesion
with hyperkeratosis and marked papillomatosis. The epidermis frequently appears attenuated with loss of the rete-ridge pattern. In nodular tumors, the epidermis is similarly thin and stretched directly over the surface of a dense dome-shaped tumor cell population. Junctional activity in either variant is often minimal and limited to atypical cells distributed predominantly along the basal layer of the epidermis. Very occasionally, more obvious in situ melanoma may be seen.
At medium-power examination, diffuse and, less often, nested growth patterns may be encountered (Figs 26.59 and 26.60). In the latter there is often considerable variation in nest size accompanied by little tendency for diminution in nest size with depth.
The infiltrating tumor cells are small, epithelioid melanocytes (reminiscent of type-A nevus cells) with pale staining or eosinophilic cytoplasm and round to oval vesicular nuclei with small eosinophilic nucleoli. Although the low-power impression may suggest maturation with depth, closer inspection
1332 Melanoma
A
B
invariably shows this to be false (Fig. 26.61).13 Pleomorphism, while subtle, is typically present and mitoses (frequently multiple) can invariably be identified, often within the deeper aspect of the tumor. Pigmentation, although variable, is sometimes seen in the deeper reaches of the dermal component and in a minority of cases, tumor-infiltrating lymphocytes are present. Occasionally, perineural infiltration is present (Figs 26.62 and 26.63). A single report describes a case with Homer-Wright type rosettes.14
Verrucous variants must be distinguished from keratotic melanocytic nevi, the most important histologic discriminants being the lack of maturation, subtle pleomorphism, and mitotic activity.15 Others have termed
1333 Histologic variants of melanoma
A
B
B
A
very similar lesions ‘papillomatous nevoid’ melanoma.16 Very occasionally, melanoma metastatic to the skin from another cutaneous site can present with a nevoid appearance.17
Immunohistochemistry may be of help in distinguishing between nevoid melanoma and a banal nevus.18 In our experience, demonstration of elevated proliferative activity using MIB-1 and sometimes cyclin D1 can be particularly valuable (Figs 26.64 and 26.65). Banal nevi show only very scattered positive cells in the superficial part of the dermal component, whereas in melanoma they may be numerous and present throughout the thickness of the lesion. It is important not to confuse positive lymphocytes
with melanoma cells when viewing MIB-1 stained sections. Double or dual staining with MIB-1 and a melanocytic marker such as MART-1 can be particularly valuable. Correlation with the hematoxylin and eosin stained section is always advised. HMB-45 can also sometimes be useful. Dermal nevi are only positive in the most superficial part of the nevus as a counterpart to morphological maturation, whereas in melanoma positive cells may be identified throughout the depth of the tumor.
FISH and comparative genomic hybridization (CGH) studies will often show findings similar to conventional melanoma and thus are frequently helpful in the diagnosis of nevoid melanoma.5,19
1334 Melanoma
While one must always be wary of missing nevoid melanoma, it is also important not to overdiagnose melanoma in nevi. This diagnostic reversal can also have untoward clinical and medicolegal consequences.20
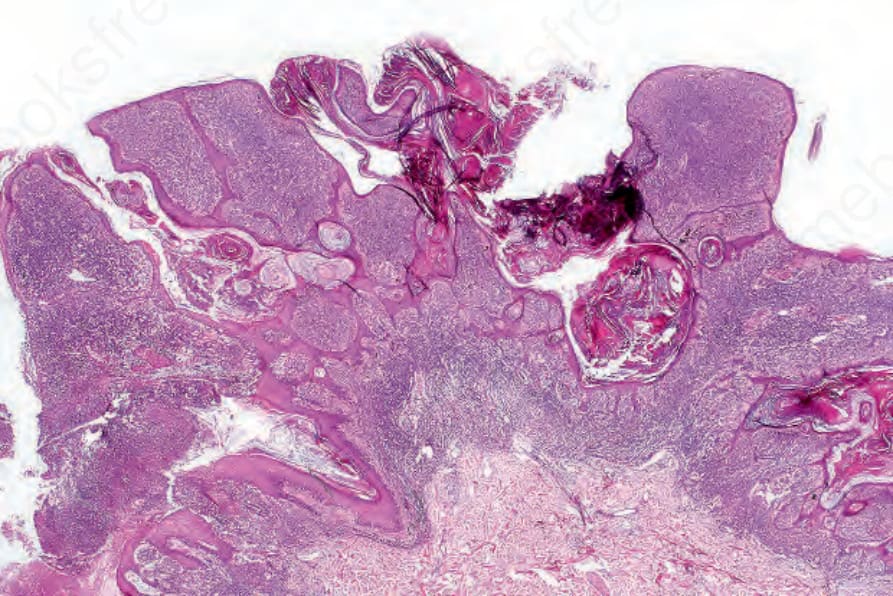
Fig. 26.57 Verrucous nevoid melanoma: verrucous nevoid lesions in the elderly should be viewed with suspicion.
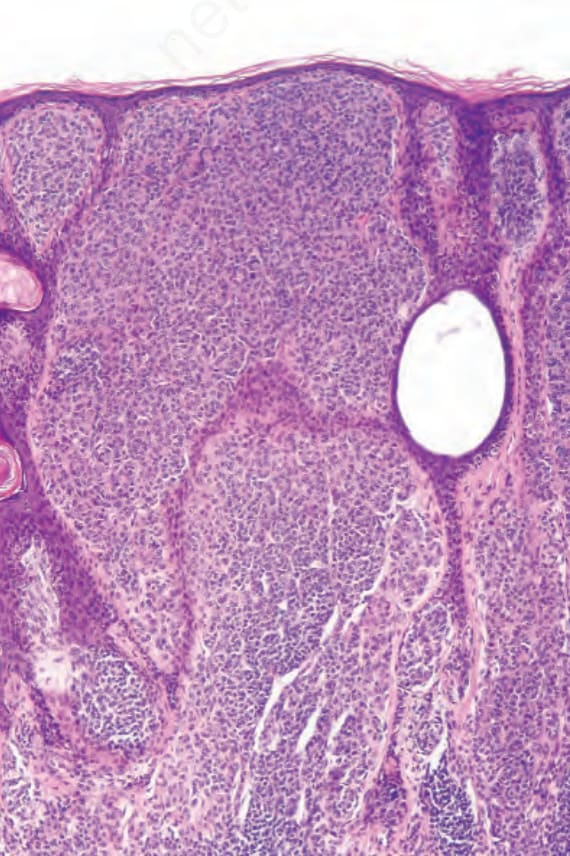
Fig. 26.59 Nevoid melanoma: expansion of the papillary dermis by a diffuse nevoid population with stretching and thinning of the associated epidermis may be a clue to the diagnosis.
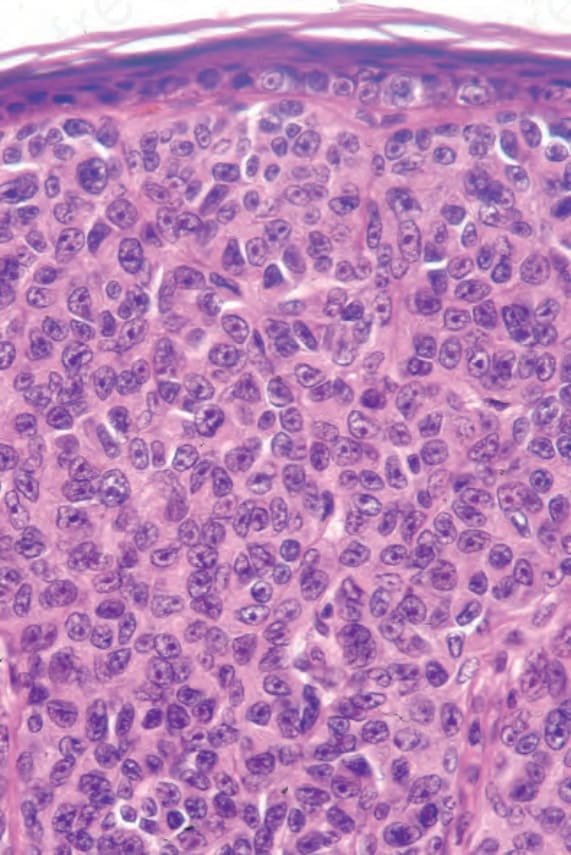
Fig. 26.60 Nevoid melanoma: the tumor cells are very uniform. Nuclei are vesicular and nucleoli prominent. A small number of tumor cells are evident in the overlying epidermis.
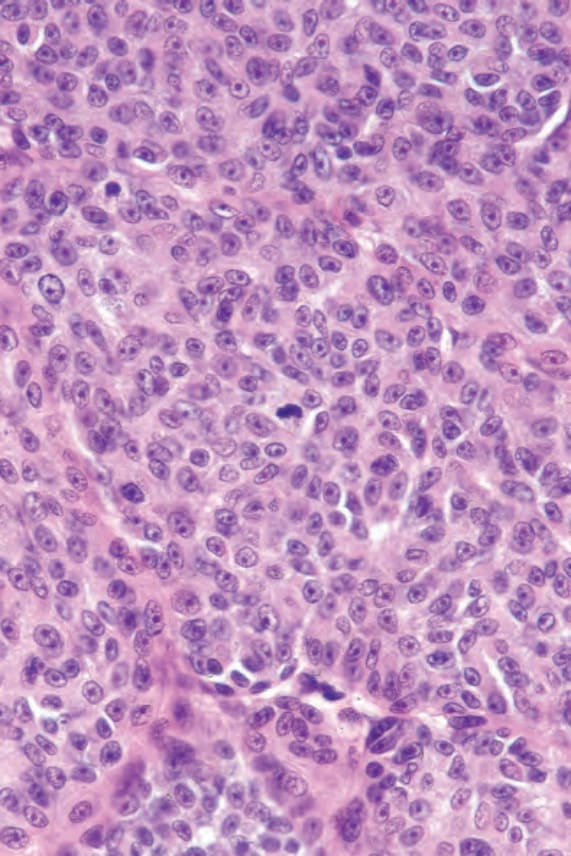
Fig. 26.61 Nevoid melanoma: there may sometimes be a suggestion of maturation with depth. Note the mitosis. This field is taken from the deep aspect of the lesion shown in Figure 26.58.
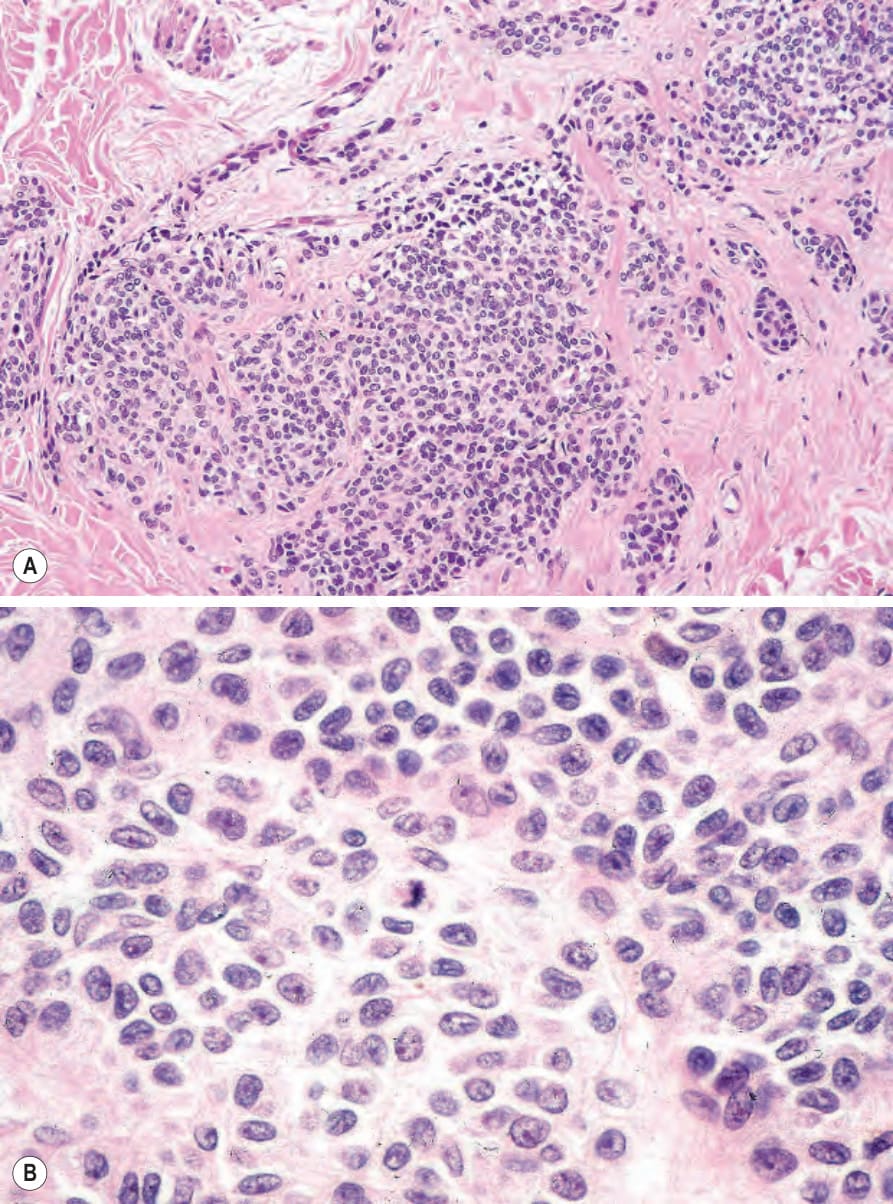
Fig. 26.62 (A, B) Nevoid melanoma: this lesion at low power is suggestive of a congenital nevus. At high-power magnification, multiple mitoses were present.
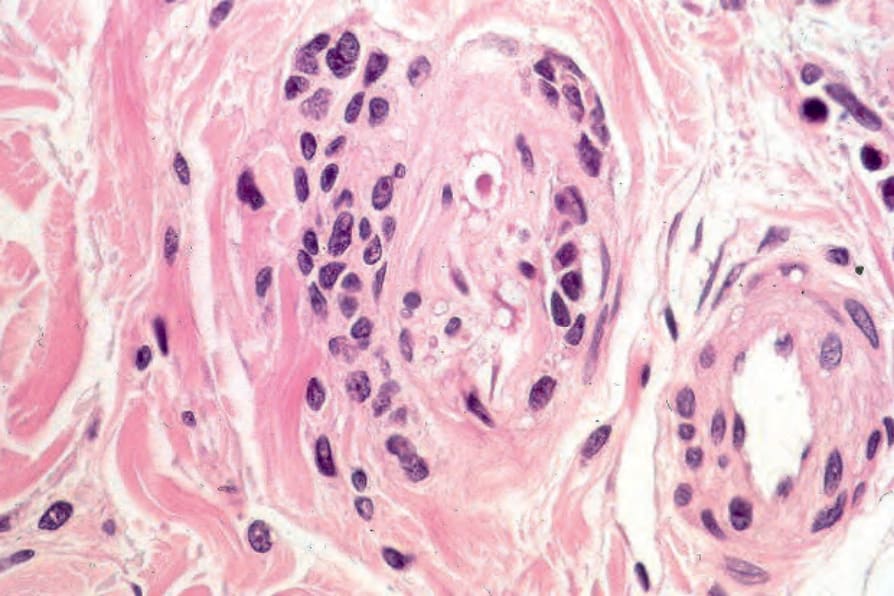
Fig. 26.63 Nevoid melanoma: note the perineural infiltration (same tumor as Fig. 26.64).
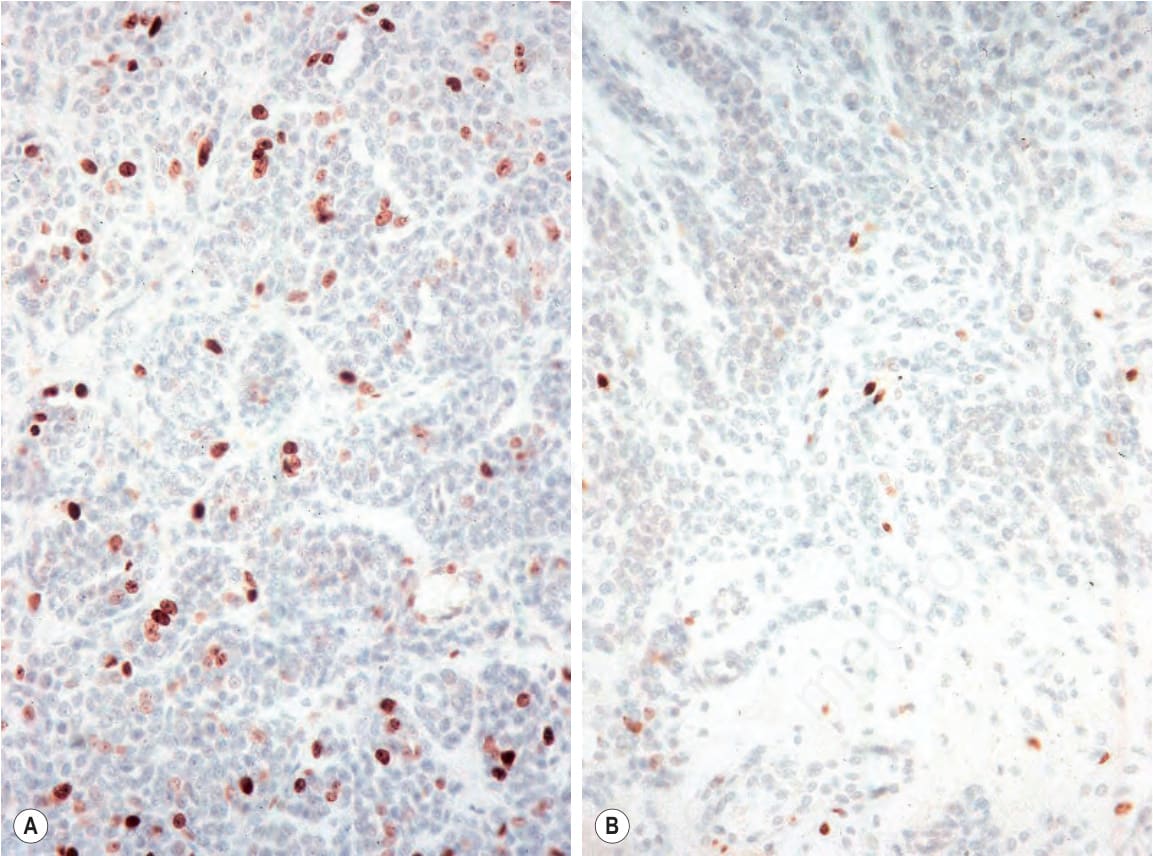
Fig. 26.64 Nevoid melanoma: MIB-1 expression is usually brisk and positively staining nuclei are commonly seen at all levels of the tumor compared with banal nevi in which only very rare positive cells are seen. (A) Nevoid melanoma; (B) banal dermal nevus.
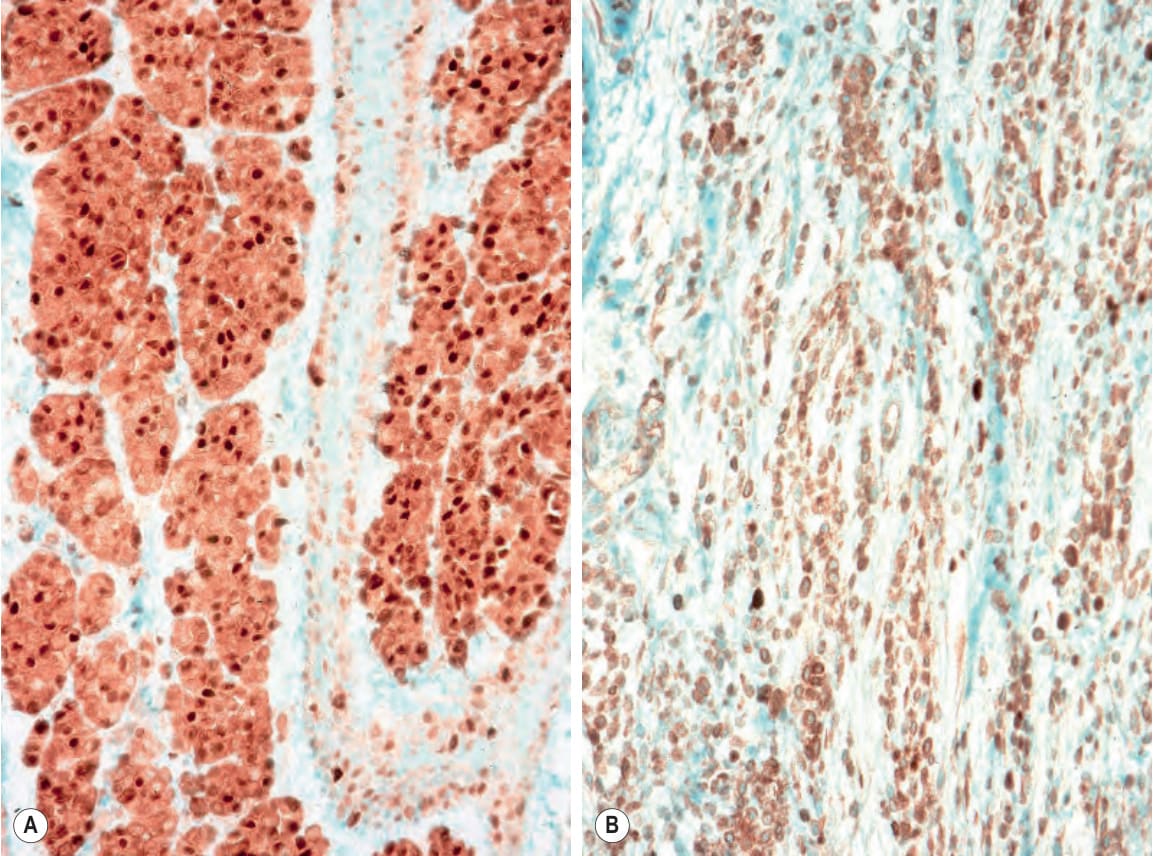
Fig. 26.65 Nevoid melanoma: nuclear cyclin D1 expression is typically brisk and present throughout the depth of the tumor compared to a banal nevus where only scattered cells are positive. (A) Nevoid melanoma; (B) banal nevus.
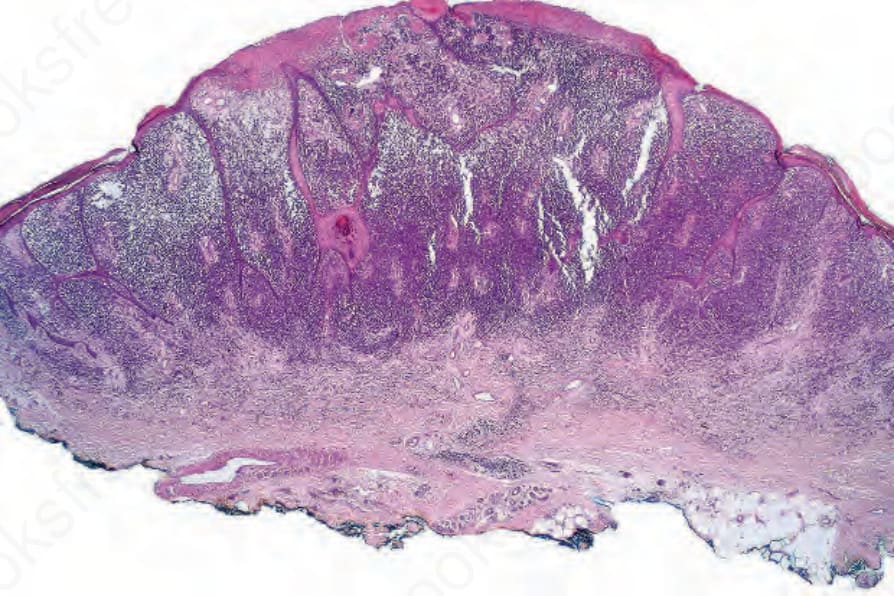
Fig. 26.66 Small cell melanoma: this variant of melanoma simulates type-B nevus cells at low-power magnification, the tumor cells being small and deeply basophilic.
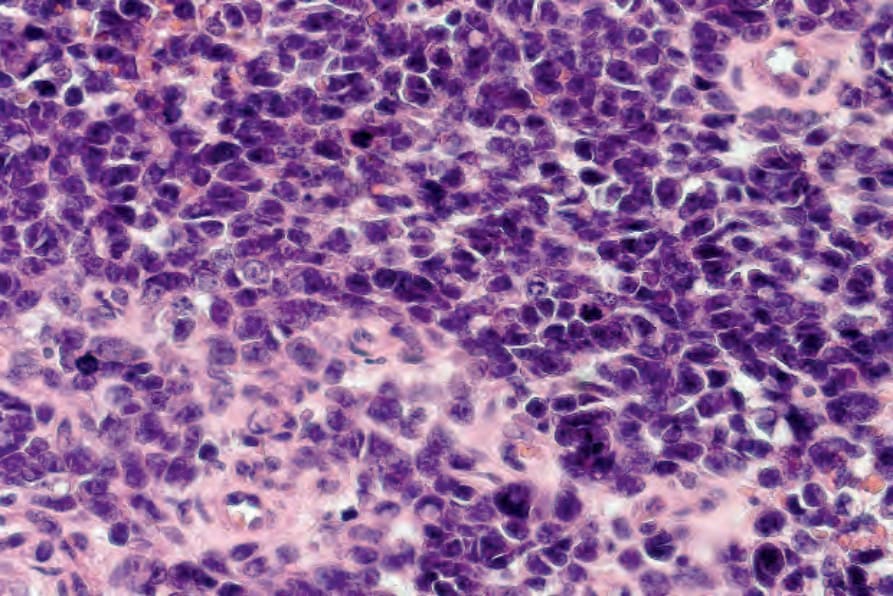
Fig. 26.67 Small cell melanoma: high-power view. The tumor is commonly mistaken for a lymphoma or neuroendocrine carcinoma if melanin pigment or junctional activity is absent.