Immunohistochemistry of melanoma
Immunohistochemistry of melanoma
Immunohistochemistry is a valuable adjunct to histology in the diagnosis of melanoma, particularly in amelanotic, epithelioid, and spindled cell variants and their distinction from undifferentiated carcinomas and mesenchymal tumors.1–3 Owing to problems of specificity and sensitivity, it is prudent to use two or even three ‘melanoma markers’ in such problematical cases. Using these markers as part of a panel looking at multiple lines of differentiation is also of practical use, such as inclusion of keratins to exclude epithelial tumors. In morphologically challenging cases, a panel of stains that supports the ultimate diagnosis by their pattern of reactivity or nonreactivity is very helpful. The role of immunohistochemistry is to provide supportive data. It should rarely if ever be used as the sole criterion by which a diagnosis of melanoma is achieved.
S100 protein remains the yardstick in the immunohistochemical diagnosis of melanoma.4–6 Although there are now substantial numbers of new markers available, none as yet, in isolation, measures up to S100 protein. However, S100 protein lacks specificity and there are very exceptional S100 protein-negative melanomas, virtually all metastatic.7,8 In cases where the diagnosis remains in doubt, use of a battery of immunohistochemical markers may be of great value.1
A
S100 protein is a calcium binding F-band protein, isolated from brain. It is variably positive in 94–100% of primary and metastatic melanomas.1,2 In addition to melanocytes, Schwann cells, myoepithelial cells, adipocytes, chondrocytes, macrophages, Langerhans cells, and tumors derived thereof, express S100 protein. Staining of Langerhans cells can sometimes be a problem, particularly when assessing the extent of intraepidermal melanocyte spread. In such instances, the addition of MITF, SOX10, HMB-45, or MART-1 may be helpful. S100 protein may also be expressed in a number of breast carcinomas and undifferentiated carcinomas.5,6 The most commonly employed antibody against S100 is a purified rabbit polyclonal antibody against S100 protein purified from bovine brain. More than 20 members of this family exist and monoclonal antibodies are available for many of them. While not well established in large series, there may be some selectivity of the isoforms between melanoma and other traditionally S100 protein reactive neoplasms in the differential diagnosis.9
B
HMB-45 reacts with the cytoplasmic premelanosome glycoprotein gp100 and is less sensitive than S100 protein.9 It is expressed by 80–86% of metastatic melanomas and between 90% and 100% of primary tumors.1,4,9 However, expression is often more focal than with S100. Sensitivity diminishes in spindled cell variants and it is usually negative in desmoplastic melanoma (see below).10,11 The junctional and superficial dermal components of banal nevi also react with HMB-45 but the deeper dermal nevus cells are generally negative. This differential staining pattern may be of value in confirmation of pre-existent banal nevus cells associated with a melanoma and in particular their distinction from small cell and nevoid melanoma, which are typically positive in a patchy fashion in the deepest nests of cells (Fig. 26.54). It is very important to remember that this pattern is lost in cases where melanocytes are pigmented as the latter are positive for HMB-45. Dysplastic nevi are similarly labeled. Blue nevi and deep penetrating nevi are also HMB-45 positive.1 Spitz nevi are often HMB-45 positive in the superficial aspect of the lesion and this is usually, but by no means always, lost with depth. This finding may be of value in its distinction from spitzoid melanoma in which staining is typically present throughout the tumor. Although it is more specific than S100 protein, HMB-45 also reacts with the group of perivascular epithelioid cell tumors (PEComas) including angiomyolipoma, lymphangiomyomatosis, and clear cell sugar tumor of the lung.12,13
Sertoli cell, and granulosa cell tumors, and tumors in the PEComa group of lesions including angiomyolipoma, lymphangiomyomatosis, and clear cell sugar tumors of the lung in addition to melanoma.18,19 It has a similar sensitivity to S100 protein in epithelioid melanomas but is less sensitive in spindled cell tumors and is not usually expressed in the desmoplastic variant. A study has shown evidence that diminished MART-1 expression correlates with increasing tumor thickness, reduced disease-free interval, and increased patient mortality.18 MART-1 expression has also been demonstrated in compound, dermal nevi and Spitz nevi with the exception of neurotized variants.15–17
MART-1 (Melan-A) is a melanosomal differentiation antigen recognized by autologous cytotoxic T cells.14–20 Some antibodies raised to this protein (e.g., A103) label a variety of lesions including adrenocortical, Leydig cell,
Antityrosinase antibody (e.g., T311) appears to be less sensitive than either S100 protein, HMB-45, or Melan-A (A103).21–26 It does not appear to label desmoplastic melanoma. Cocktails of HMB-45, MART-1, and antityrosinase antibodies are used by some to increase sensitivity for detection of melanocytic differentiation.27
Microphthalmia transcription factor (MITF) is a transcriptional regulator important for tyrosinase expression.28 It is strongly positive in nevi and epithelioid melanoma.29–31 Sensitivity is reduced in spindled cell and desmoplastic variants.32 Spitz nevi and neurotized banal nevi show diminished expression. The specificity of MITF is low and this limits its use in the differential diagnosis of mimickers of melanocytic lesions. Its main use is in the evaluation of intraepidermal melanocytes as the staining is nuclear and other cells that reside in the epidermis are not positive for this marker.
The monoclonal antibody, SM5-1, was created by a subtractive immunization protocol using human melanoma samples and binds a variant of
fibronectin.33,34 Initial reports indicated that its sensitivity is similar to S100 protein with improved specificity for other traditionally S100 protein reactive, but the antibody also reacts with hepatocellular carcinoma and breast cancer cells.26,35 This antibody is not widely used for clinical diagnosis.
SOX10 is a transcription factor that is a critical regulator of melanocytes.36–38 Antibodies raised against it represent another marker of melanocytic and Schwann cells and tumors derived from the neural crest.39 While it lacks specificity and stains other cells it is equally sensitive and more specific than S100 protein in relevant differential diagnoses with soft tissue neoplasms.40,41 It is also useful in desmoplastic melanoma, though expression has also been noted in scars.42–44 It has gained widespread use as a sensitive marker for melanoma, often used in combination with other melanocytic markers.45 It has been suggested to be more specific than other melanocytic markers in the setting of determining melanocytic density in chronically sun-damaged skin where misleading false-positive rates are noted with other markers.46 A role has also been suggested in evaluation of sentinel lymph nodes.47
1329 Immunohistochemistry of melanoma
The bar is high for inclusion of new markers as standards for melanoma in clinical practice. All antibodies have a natural history of decreasing specificity with study of additional tumor types and new antibodies are not as far down this curve as older antibodies, creating potential for misinterpretation if the new reagents are used alone.
Melanoma cells can express epithelial markers including keratins, EMA, and CEA.2,48–50 Keratin, particularly those of low molecular weight, may be identified in as many as 10% of melanomas, both on frozen and on paraffin-embedded sections.2 CEA is commonly encountered if polyclonal antibodies are utilized.49,50 Metastatic disease more often shows such aberrant staining patterns than primary tumors. Diagnostic difficulties are unlikely to be encountered provided S100 protein and/or other melanoma markers have been included in the antibody panel. SMA and desmin are very rarely expressed in melanoma with the exception of the desmoplastic variant where, as in most spindle cell tumors, SMA can be detected to varying degrees.51 One study with dual labeling for S100 protein and SMA in desmoplastic melanoma indicates that the SMA reactivity may be in accompanying stromal myofibroblasts.52
Melanoma cells can express histiocytic markers such as CD68 (KP1) in 80% or more of tumors.53,54 Mac 387 and α1-antitrypsin may also be positive. This is of particular significance since the distinction between tumor cells and histiocytes, particularly in sentinel lymph node specimens, can sometimes be problematical. In addition, distinguishing between balloon cell melanocytic lesions and xanthomatous infiltrates may require immunohistochemical confirmation, particularly if no residual recognizable melanocytic component is visible. In such circumstances, positive melanocytic markers are obviously of major diagnostic importance.
There is an ever-expanding range of reputed immunohistochemical prognostic markers.55–57 Most of these lack appropriately powered full multivariate analysis linking the marker with specific outcome such as melanoma-specific mortality supplemented by hazard ratios and do not fully describe the methods utilized as recommended by the REMARK (Reporting recommendation for tumor MARKer prognostic studies) guidelines of the NCI-EORTC or AJCC precision medicine reporting recommendations for tumor marker prognostic studies.58–62 The more useful of these are very briefly discussed below. Few of these are validated to the level necessary for routine application to clinical samples; virtually all are reported in retrospective cohorts with referral and other biases. Use of multiple markers and application of rigorous methods of quantification have efficacy, distinguishing different prognostic groups.63 The markers discussed below are primarily used to help support a diagnosis of melanoma or nevus in the relatively small subset of cases where this determination is challenging on purely histologic grounds.
A
Ki-67 (MIB-1) is a particularly valuable adjunct in the distinction between benign melanocytic nevi (including Spitz nevi) and melanoma.64,65 In nevi, less than 5% of nuclei are positive (and these are usually located in the most superficial aspect of the dermal component) whereas in melanoma 25% or more of cells are labeled (Figs 26.55 and 26.56). Its role in predicting biological behavior is controversial; thus although in earlier studies increased expression in thick tumors was thought to correlate with
B
1330 Melanoma
poor survival, more recently it has been claimed that increased expression in thin tumors (< 1.5 mm) is of greater significance.66–69 A further study indicates that increased MIB-1 reactivity is a poor prognostic factor in terms of disease-specific survival independent of tumor thickness.70 Obviously, there is a proportional, though not exact, relationship between degree of nuclear MIB-1 reactivity and mitotic rate. Mitotic rate is an important determinate of melanoma outcome, though it no longer drives groupings in the 8th Edition of the AJCC staging system.71 How to correlate Ki-67 reactivity with mitotic rates is evolving. Increased Ki-67 expression also correlates with overexpression of p53 protein and loss of p16 (see below).68,70
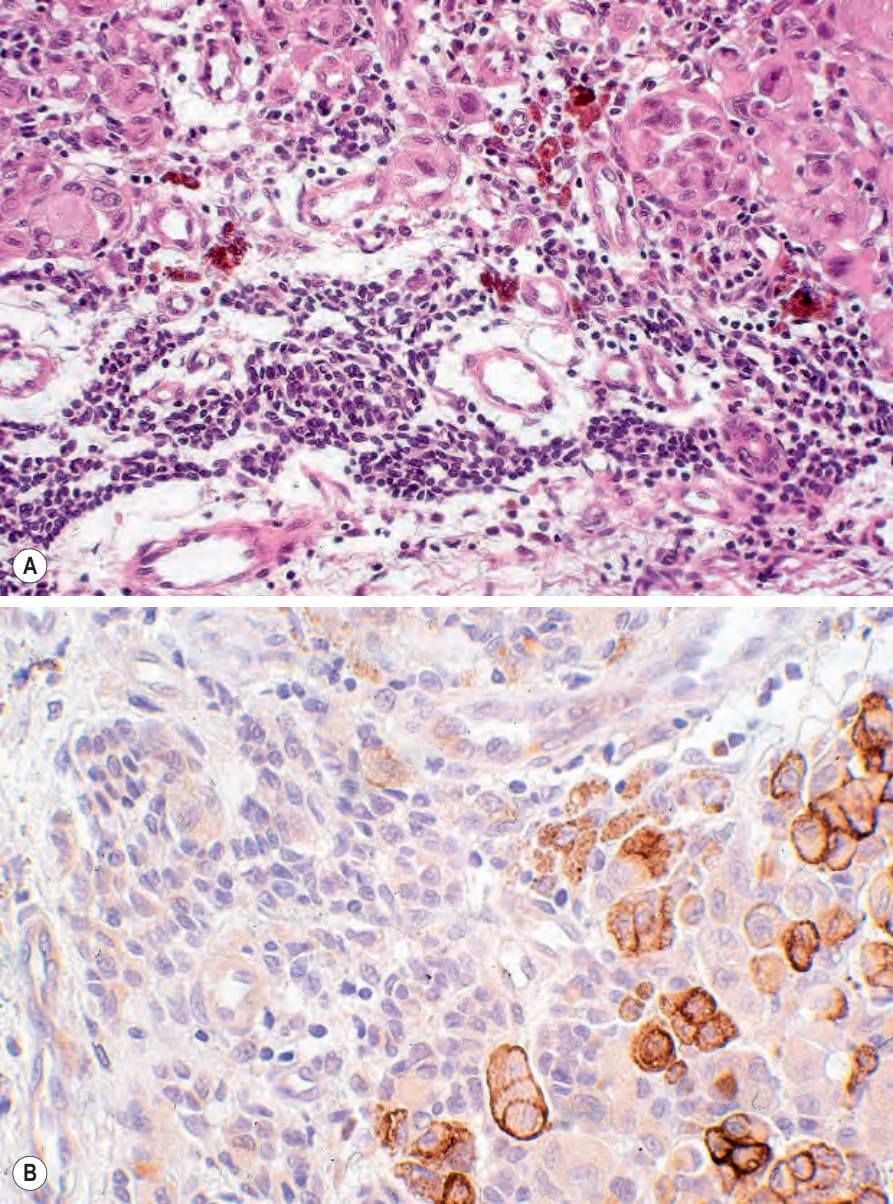
Fig. 26.54 Melanoma: this tumor has arisen in a background of a banal nevus. (A) Compare the eosinophilic, pleomorphic tumor cells with the small basophilic nevus cells; (B) the melanoma cells are HMB-45 positive; the nevus cells are negative.
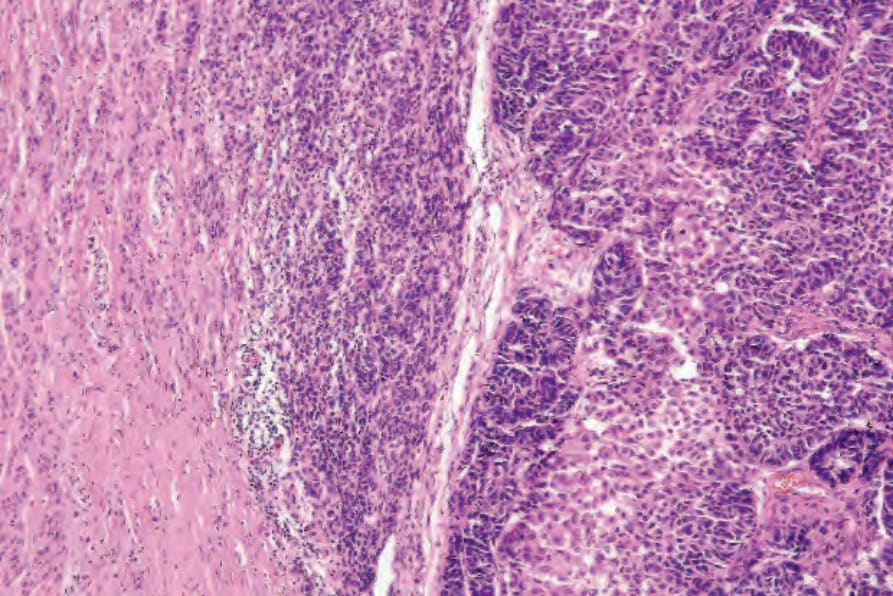
Fig. 26.55 Melanoma: this tumor (right side of field) has arisen in a background of a congenital nevus (left side of field).
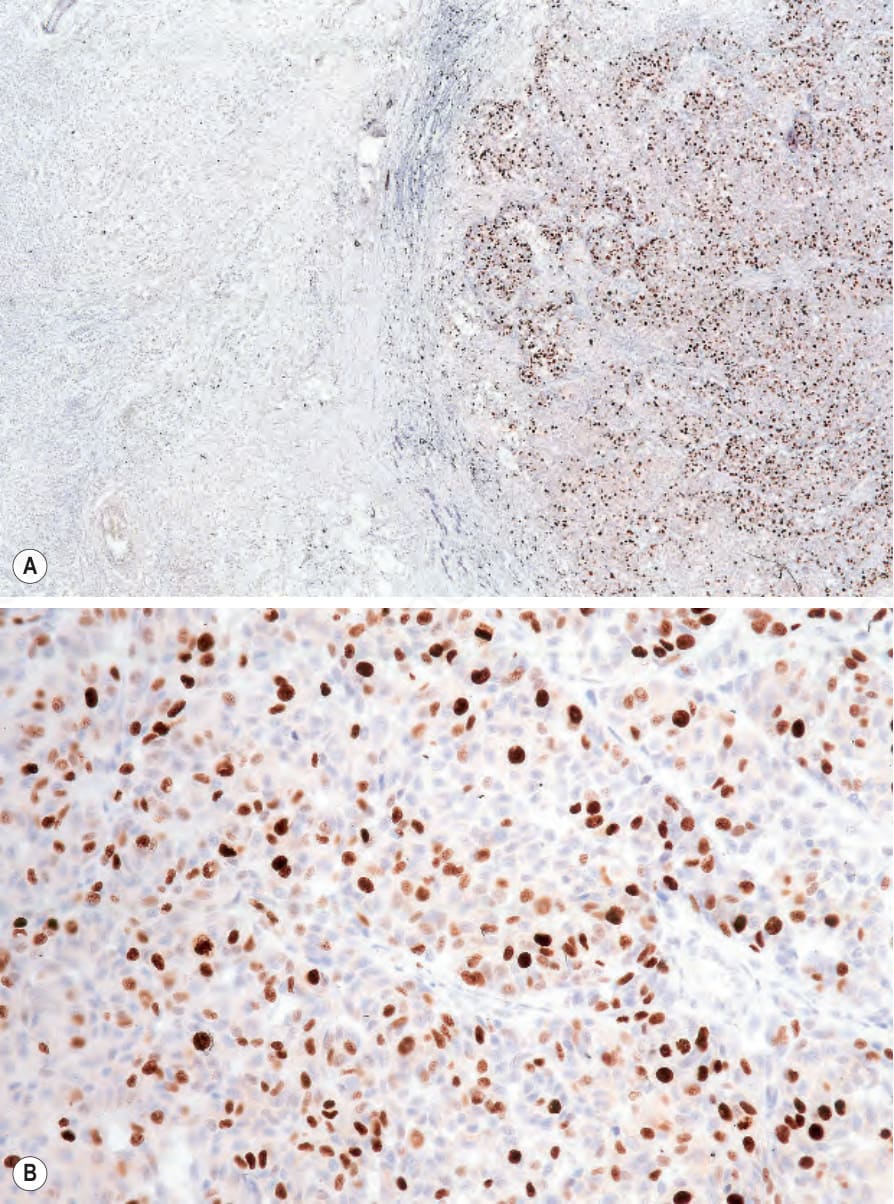
Fig. 26.56 (A, B) Melanoma: the melanoma shows very brisk MIB-1 expression, and the nevus is completely negative.
including some that are U.S. FDA-approved companion diagnostics, but such testing is not currently required to use immune checkpoint inhibitor therapy in melanoma.123 Indeed, melanomas can respond to PD-1 (CD247/ programmed cell death protein 1) inhibitors even if they completely lack membranous PD-L1 expression.124 Most PD-L1 antibodies have very similar staining profiles in melanoma and other tumors as well.125,126 Specific scoring approaches have been suggested and used for clinical trials and in routine practice. Staining for CD8-positive T-cells in melanoma can also be performed and higher levels are associated with increased likelihood of response to immuno-oncological therapy. Approaches for scoring these infiltrates have been suggested, but are not widely employed in routine clinical practice.127–130 These biomarker approaches are used primarily in metastatic disease and their correlation with response is not perfect.131,132 This is an active area of research and a number of genomic and other patient factors have also been associated with patient response. Companion immunohistochemical approaches are not currently used in clinical practice for CTLA-4 (CD152) inhibitors in melanoma. Anti-CTLA-4 therapy is sometimes used in combination with PD-1 inhibitors. PD-L1 expression can inform whether PD-1 monotherapy or combination approaches are employed in melanoma.124 Additional work in this area is likely to produce more associated biomarkers as immuno-oncology expands to a number of emerging novel agents such as inhibitors of IDO1, LAG-3, and others where expression of the protein targets might be associated with treatment efficacy.133,134
Phosphohistone H3 (PHH3) recognizes mitotic figures directly rather than cell cycle like MIB-1 and can assist in more objectively determining mitotic rates which do correlate with outcome.72–79 Care must be taken when increasing the sensitivity of mitotic rate detection since the majority of the data is derived using the less sensitive, but currently gold standard microscopic detection on H&E stains, as inappropriate inflation of prognosis can occur.
Bcl-2 is strongly expressed in normal melanocytes and in a variety of nevi including banal, congenital, Spitz, blue, and dysplastic variants.80–83 Although there is some variability of results in the literature, diminished expression has been said to correlate with melanoma, particularly metastatic lesions. Similarly, in problematical spitzoid lesions, strong expression may favor a diagnosis of benignancy.84 Bcl-2 downregulation has been correlated with melanoma progression.85–87 High bcl-2 was associated with improved disease-specific outcome when assessed in either primary or metastatic lesions using automated assessment of immunofluorescent immunohistochemistry.88 From our own experience, however, bcl-2 is as often positive in melanoma as it is in banal nevi and it is therefore of little value in difficult cases.
Cyclin D1 may be of help in differentiating between a banal nevus and a nevoid melanoma or a nevic component within a melanoma. Its expression throughout the full thickness of a melanoma has been reported in up to 60% of cases, whereas staining may be absent or limited to only occasional cells in the superficial aspect of a nevus.89,90 Increased cyclin D1 reactivity may correlate with amplification of its encoding genetic locus.91–93 High levels of cyclin D3 in superficial melanoma have been found to correlate with early relapse and decreased survival.94 This finding regarding cyclin D3 needs further confirmation.90 Interestingly, cyclin D1 may interact more with CDK4 while cyclin D3 interacts more readily with CDK6, suggesting different functions for these two cyclin D isoforms.95