Acral lentiginous melanoma
Acral lentiginous melanoma
In the early stages of the radial growth phase of acral lentiginous melanoma the changes may be quite subtle, consisting of irregular epidermal hyperplasia and scattered, basally located, atypical melanocytes.166–170 The established lesion shows acanthosis with marked elongation of the epidermal ridges and obvious melanocytic atypia (Figs 26.33 and 26.34). The lower reaches of the epidermis are infiltrated by large numbers of atypical melanocytes characterized by nuclear pleomorphism and hyperchromatism, and showing a cytoplasmic fixation retraction artifact. Nucleoli are conspicuous and mitotic figures may be identified. Although spindled forms are most often encountered, epithelioid and giant cells are sometimes evident. Scattered foci of junctional nests may also be detected, usually at the tips of the epidermal ridges (Fig. 26.35). A heavy bandlike chronic inflammatory cell infiltrate is frequently present. The invasive tumor is often a spindled cell in type and may elicit a desmoplastic reaction (Fig. 26.36). Deep extension along the sweat gland epithelium is common and neurotropism may be evident in a subset of cases. Cross-sectioning of involved sweat glands may lead to the erroneous interpretation of invasion. Occasionally, acral tumors may show a superficial spreading in situ component or represent de novo nodular melanoma with absent radial growth phase.
1319 Cell types
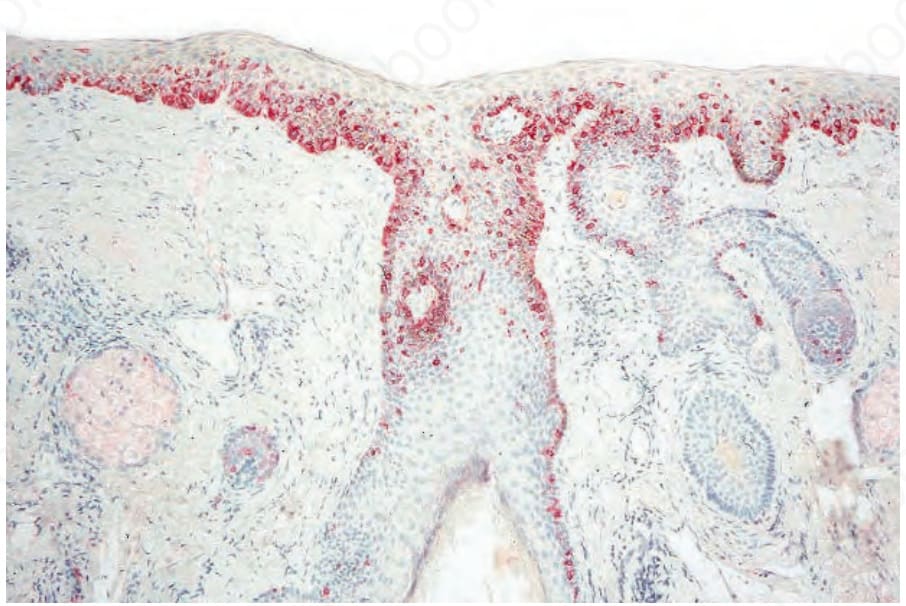
Fig. 26.26 Lentigo maligna: occasionally it is difficult to distinguish between actinic keratosis and lentigo maligna. In such cases, immunohistochemistry using a red chromogen (in this case alkaline phosphatase) can make the distinction easy.
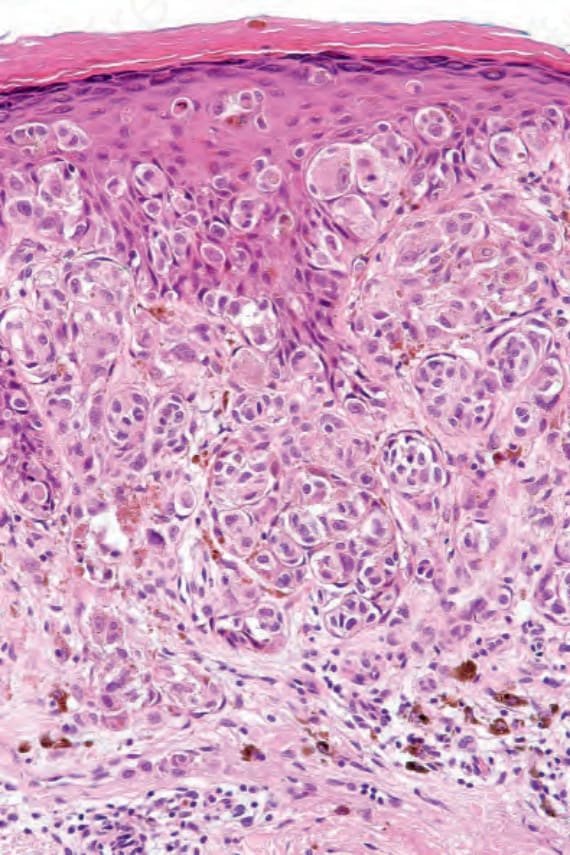
Fig. 26.29 Superficial spreading melanoma: invasive tumor is usually of the epithelioid type as shown in this field. Note the abundant cytoplasm, nuclear pleomorphism, and prominent nucleoli.
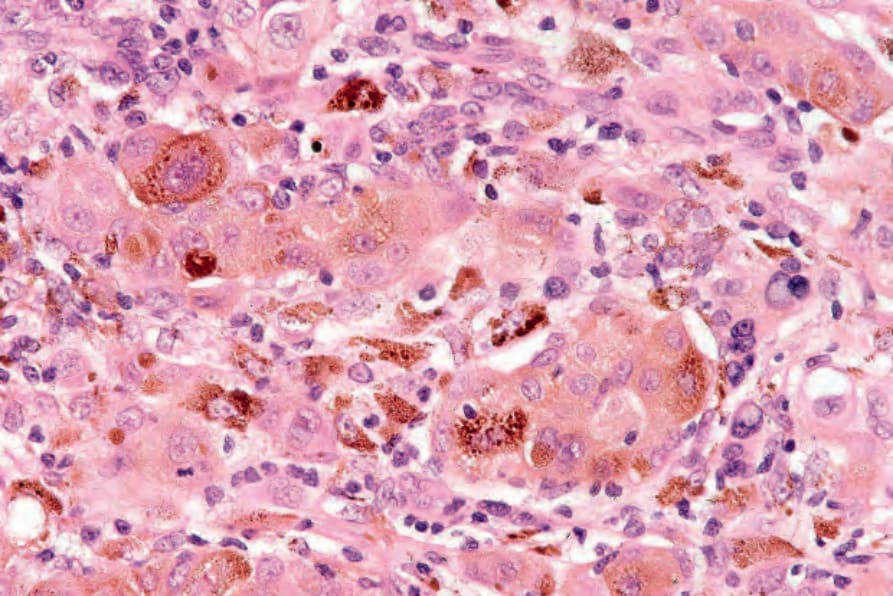
Fig. 26.30 Superficial spreading melanoma: in this example there is heavy melanin pigmentation.
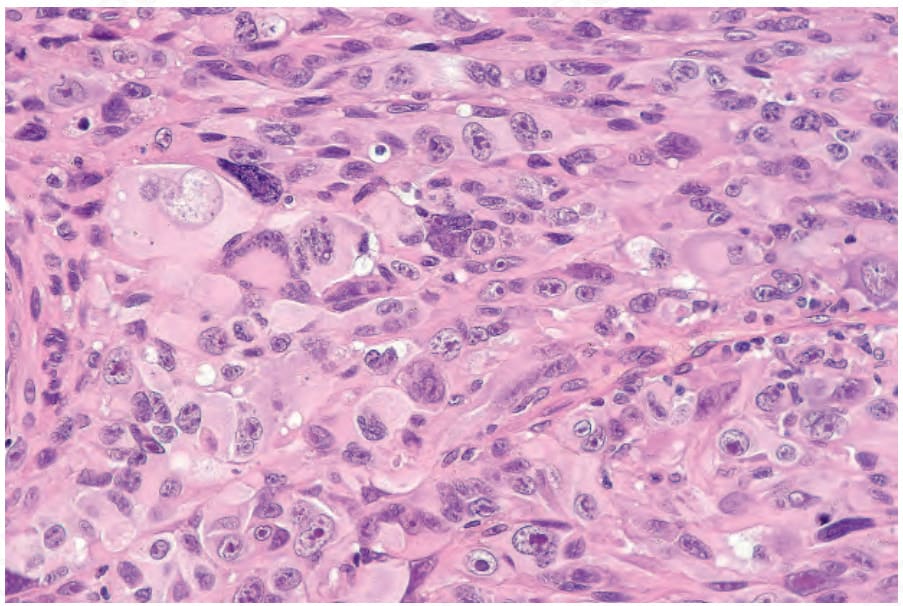
Fig. 26.31 Superficial spreading melanoma: diagnosis of amelanotic tumors, particularly when very pleomorphic as in this example, often depends upon immunohistochemistry if a junctional component is not evident.
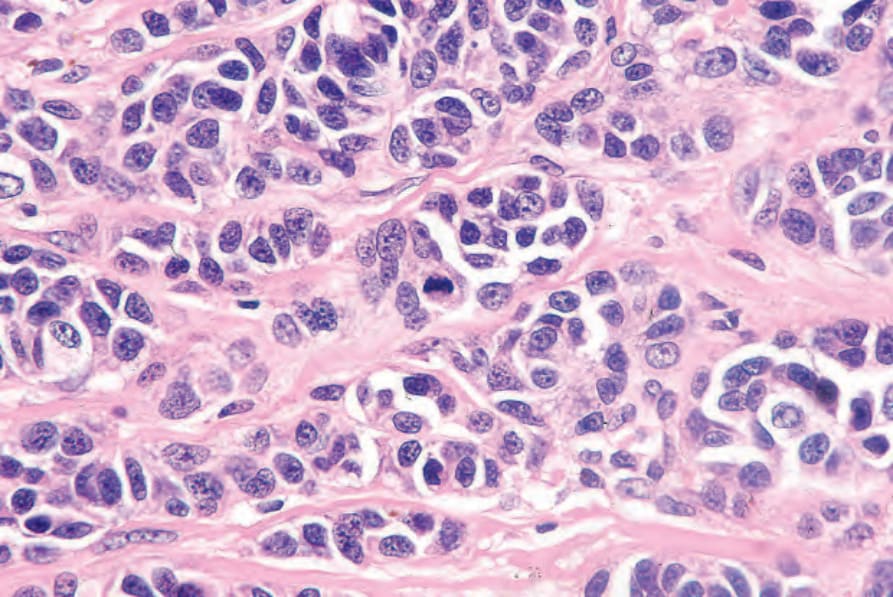
Fig. 26.32 Superficial spreading melanoma: this example shows a mitotic figure in the center of the field.
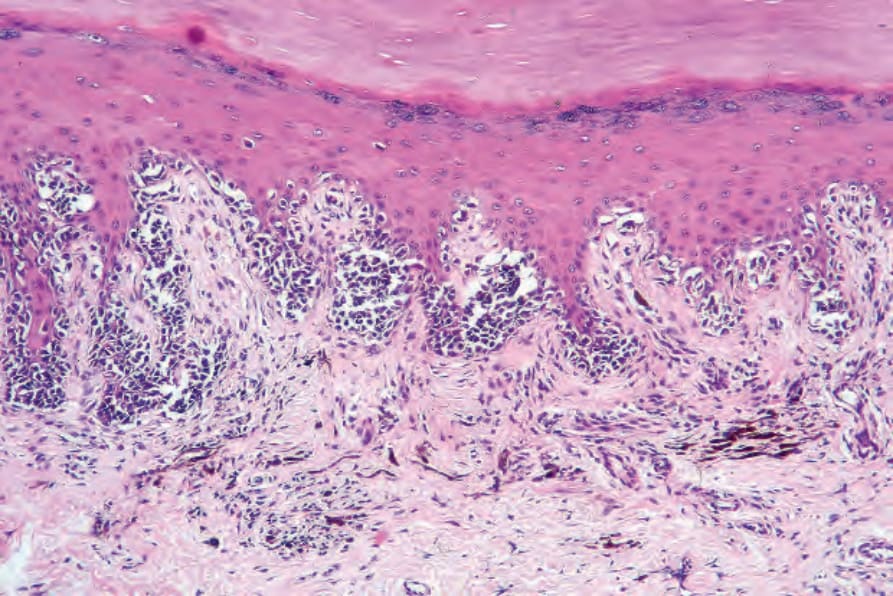
Fig. 26.33 Acral lentiginous melanoma: in this in situ lesion, there is irregular acanthosis, hypergranulosis, and hyperkeratosis. Tumor cells are hyperchromatic and distributed in a lentiginous and nested pattern. The dermis is scarred and there are conspicuous melanophages and chronic inflammatory cells.
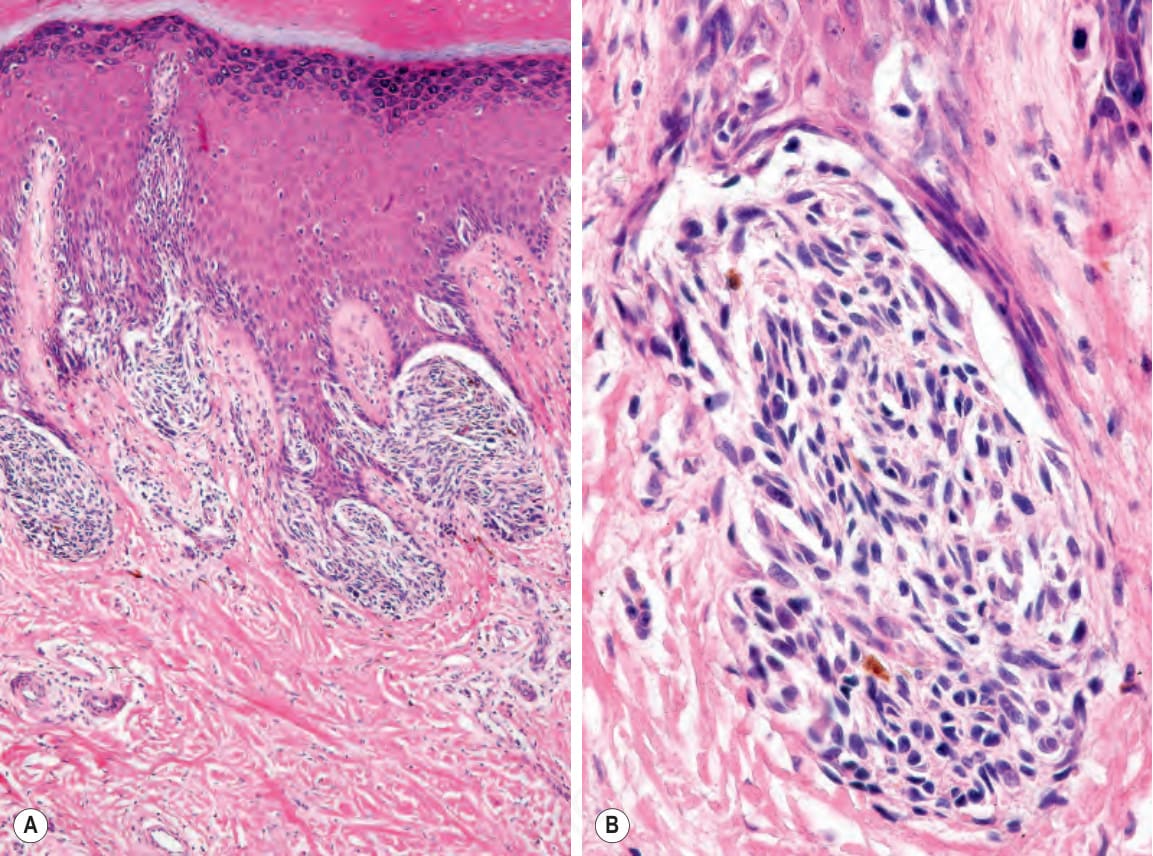
Fig. 26.35 (A, B) Acral lentiginous melanoma: large junctional nests are present at the tips of the rete.
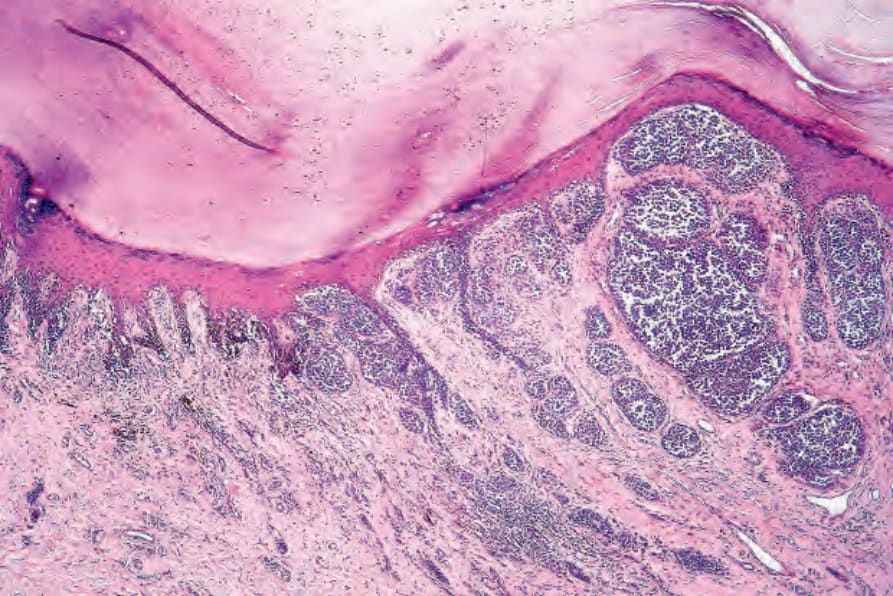
Fig. 26.36 Acral lentiginous melanoma: in this example, the invasive component is mixed epithelioid, spindled cell, and desmoplastic.