Nodular melanoma
Nodular melanoma
Nodular melanoma (3–4%) has no radial growth phase and therefore may be distinguished clinically from nodules of invasive tumor that have arisen in lesions associated with a pre-existent radial growth phase.135 It has a poor prognosis (the majority being thick tumors by the time of excision), affects more males than females (2 : 1), and generally arises in the fifth or sixth decade.136 The trunk and limbs are most commonly involved. The tumor, which may be nodular or polypoid (polypoid melanoma), is often ulcerated and, when lacking pigment (amelanotic melanoma), is frequently mistaken
Melanoma arising at noncutaneous (primarily mucosal) sites
Melanoma may arise at a diverse range of sites other than the skin, including the orbit, the oral cavity and nasal cavities, the external genitalia, vagina, urethra, and anus.137–139 In general, mucosal tumors are associated with aggressive behavior and a poor prognosis.138,140–143 This relates particularly to delayed presentation. Rare sites for primary melanoma also include the meninges, esophagus, stomach, uterus, cervix, breast, biliary system, bronchus, and adrenal gland.
Histologic features
Central to our understanding of the histologic classification of cutaneous melanoma is the concept of radial (horizontal) growth phase and vertical (invasive) growth phase.33,108,114,144,145 By current definition, the radial
1314 Melanoma
growth phase may include (in addition to a wholly in situ, intraepidermal component) evidence of microinvasion into the papillary dermis (microinvasive radial growth phase), often accompanied by features of regression (Figs 26.11 and 26.12). The microinvasive stage of melanoma is believed to lack significant metastatic potential and as a consequence is associated with an excellent prognosis.146–149 Indeed, in a large series of patients discussed by Clark and coworkers, no tumors in the radial growth phase were associated with metastatic spread.109
phase (Fig. 26.14).33,145,151 Mitotic figures are common.33 Features of regression may be seen but are usually absent at the base of the tumor. The tumor cells in the vertical growth phase are pleomorphic and apoptosis is often present. Vertical growth phase implies an alteration in biological potential with a capacity for lymphovascular invasion and metastatic spread.33,145,146
Histologically, the microinvasive radial growth phase tumor is characterized by single cells or small aggregates of melanoma cells, histologically similar to their intraepidermal counterparts and invariably forming tumor nests smaller than those present within the overlying epidermis.33 A lymphohistiocytic infiltrate is usually present. Mitotic figures are absent by definition. The last feature is of particular importance; multiple levels should therefore be carefully examined before making a diagnosis of microinvasive radial growth phase melanoma (Fig. 26.13).150
Vertical growth phase melanoma is composed of cohesive nests, nodules, or plaques larger than those present within the epidermis and consisting of tumor cells that are cytologically different from those in the radial growth
A subset of melanocytic tumors can be challenging to definitively assess as either benign or malignant and are described under various names to indicate their uncertain malignant potential. Such cases often have some, but not all or fully developed features of the malignant phenotype histologically. Experts often disagree on the designation of malignancy in this group of exceedingly challenging lesions.152–155 Multi-probe fluorescence in situ hybridization (FISH) and genomic hybridization can assist diagnostically, but in some cases the biological potential of these equivocal lesions remains uncertain.156 Proposals have suggested that in such cases, grouping the lesions into classes linked to the type or extent of excision needed increases agreement and aids in communication of the clinical care needed despite the uncertainty in the diagnosis.157
1315 Histologic features
B
A

Fig. 26.9 Nodular melanoma: this heavily pigmented, dome-shaped nodule has no adjacent macular component. From the collection of the late N.P. Smith MD, the Institute of Dermatology, London, UK.
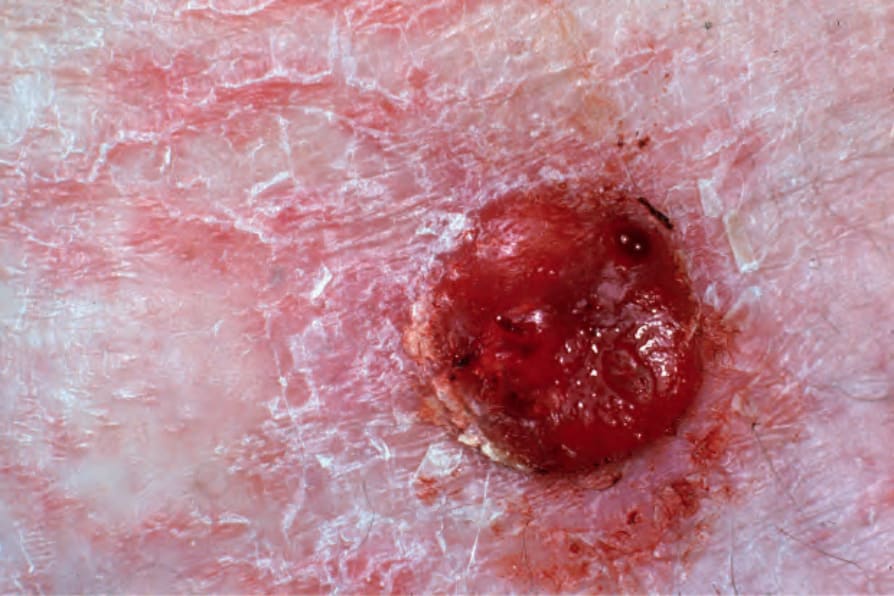
Fig. 26.10 Nodular melanoma: amelanotic tumors as shown here are often a source of clinical (and histological) diagnostic difficulty. From the collection of the late N.P. Smith MD, the Institute of Dermatology, London, UK.
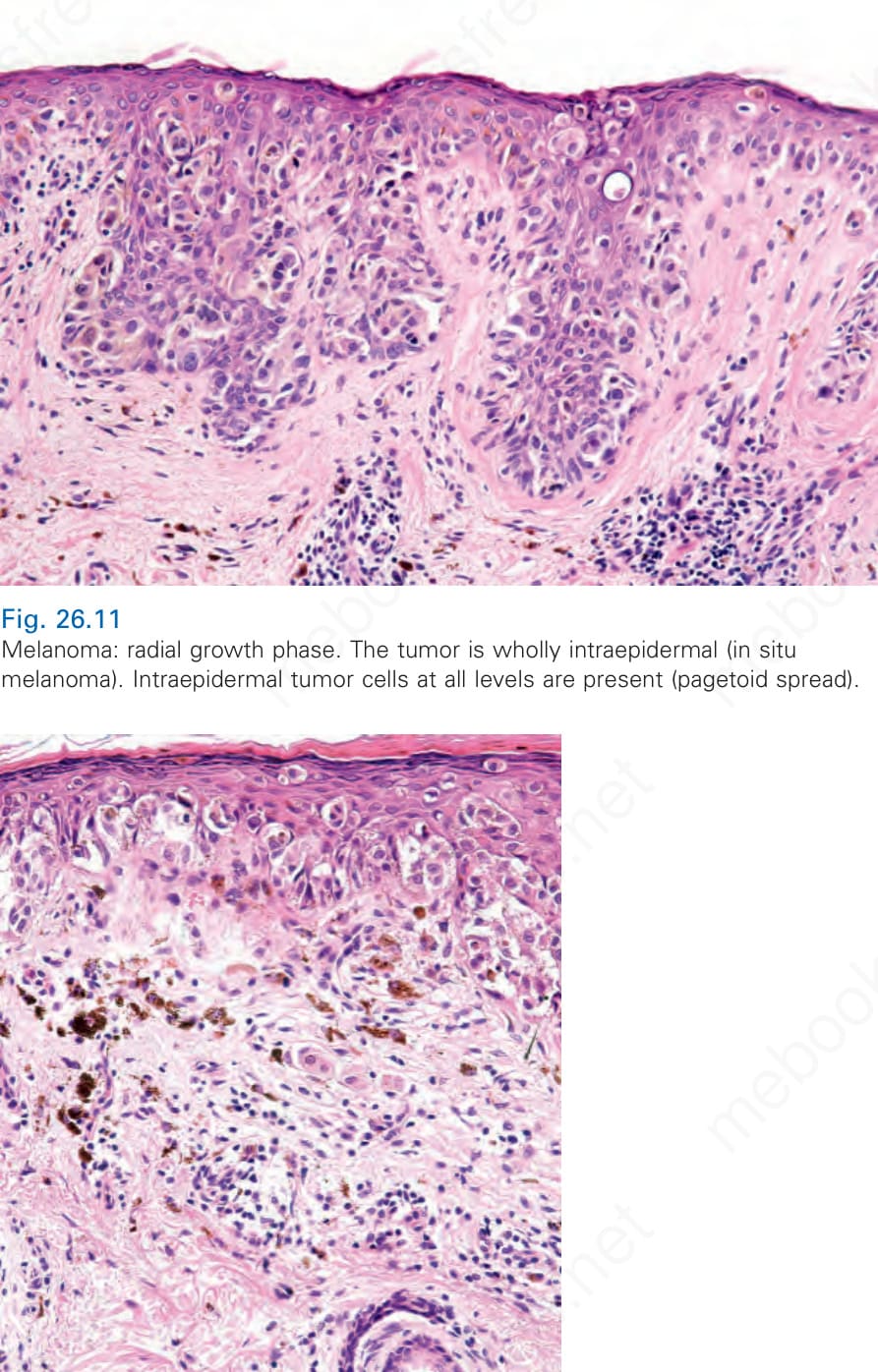
Fig. 26.11 Melanoma: radial growth phase. The tumor is wholly intraepidermal (in situ melanoma). Intraepidermal tumor cells at all levels are present (pagetoid spread).
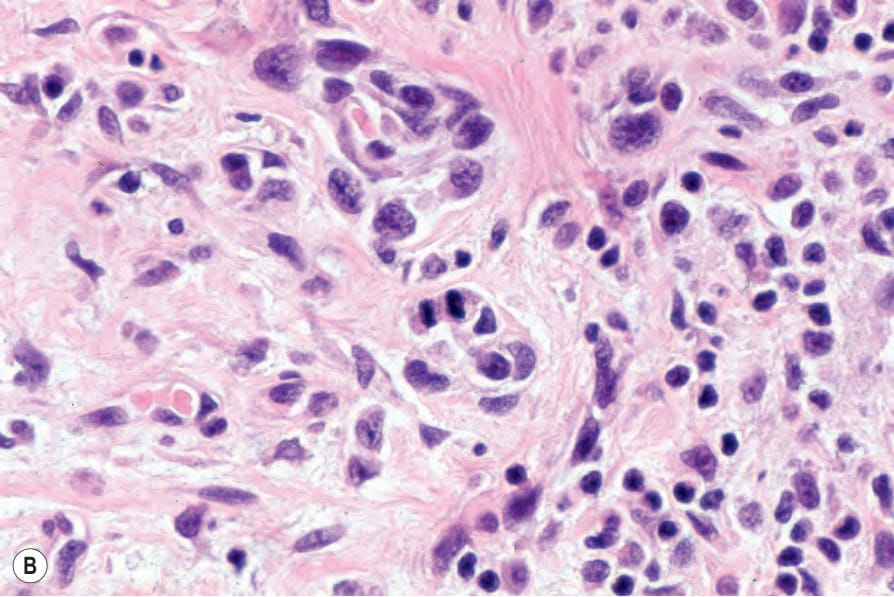
Fig. 26.12 Melanoma: microinvasive radial growth phase. In addition to in situ tumor, small numbers of single tumor cells are present in the papillary dermis.
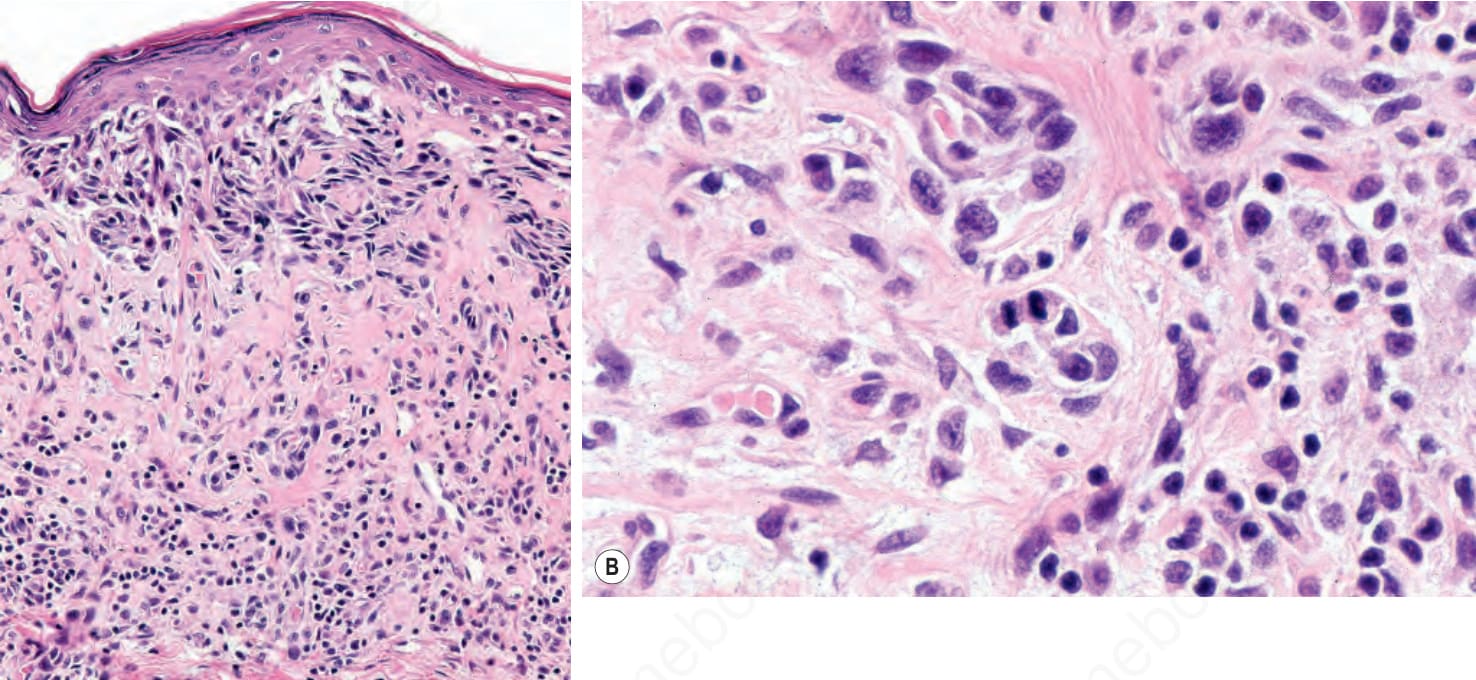
Fig. 26.13 (A, B) Melanoma: lentigo maligna melanoma. This tumor was incorrectly diagnosed as a microinvasive radial growth phase lesion on the grounds that only single cells were present in the dermis and there were no nests. Dermal mitoses were, however, present (B). The patient developed cerebral metastases.
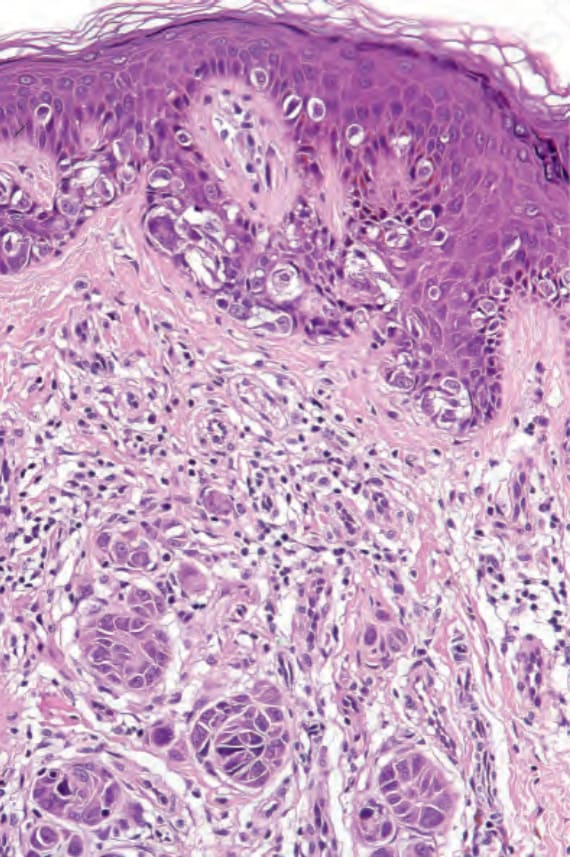
Fig. 26.14 Melanoma: vertical growth phase. In addition to in situ (radial growth phase) tumor, there are multiple nests in the dermis. These are larger than the epidermal ones.
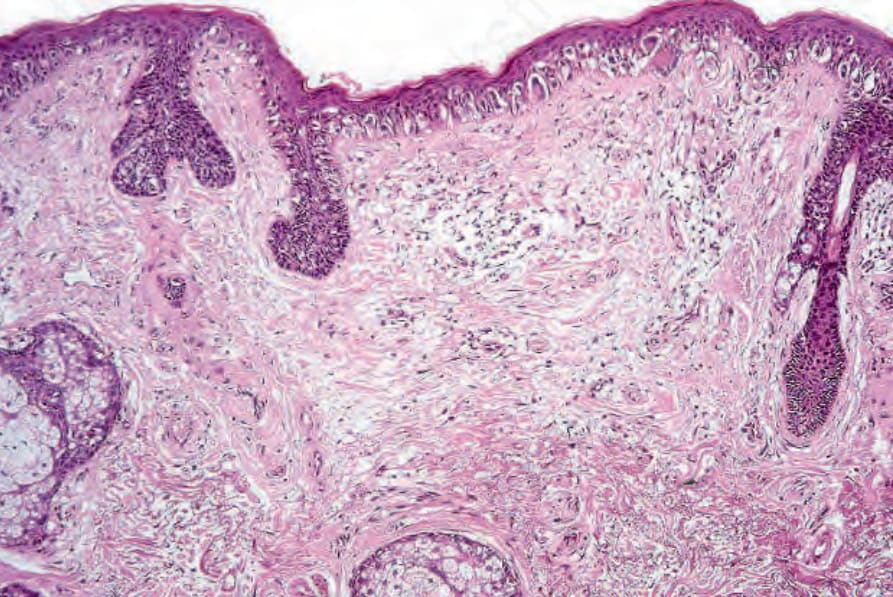
Fig. 26.15 Lentigo maligna: the epidermis is atrophic and flattened. Atypical melanocytes are basally located and the superficial dermis shows marked solar elastosis.