Cellular blue nevus
Cellular blue nevus
The cellular blue nevus is a rare dermal neoplasm that is particularly important because it may be confused both clinically and histologically with melanoma. The recognition of benign ‘metastasizing’ variants is critical to prevent unnecessary potentially mutilating surgical treatment.1,2
Clinical features
Cellular blue nevi are uncommon lesions and occur much more often in Caucasians than in dark-skinned races. They show a female predominance (2 : 1).1 Presentation is usually in the second, third, or fourth decade, but occasionally they are evident at birth.1 Although they may arise at a wide variety of sites (scalp, face, trunk, and extremities), over 50% develop over the sacrococcygeal region and buttocks (Fig. 25.239).1,3 The distal extremities are also sites of predilection.3 Typically, they are slowly growing, grayish blue, blue-black or black, dome-shaped papules or nodules 1–2 cm or more in diameter, which may rarely ulcerate or become painful. Giant cellular blue nevi measuring in excess of 10 cm in diameter have rarely been reported.4 Cellular blue nevus with satellitosis is characterized clinically by development of macules around a central papule or nodule, and may thus mimic a melanoma.5 These nevi have been described at a variety of other sites including the cervix, vagina, spermatic cord, and breast.1 Intraocular, conjunctival, and intraoral variants have also been documented.3,6,7
Histologic features
The cellular blue nevus is a large, often well-circumscribed nodular mass that fills the dermis and may occasionally involve the subcutaneous fat, giving the tumor a dumbbell morphology (Fig. 25.240).1,3 The epidermis is normal unless the features of a combined nevus (i.e., junctional activity) are present.
A number of histologic variants are recognized.3 Most tumors show a biphasic pattern consisting of an admixture of:
• plump spindled cells with pale cytoplasm and round or oval vesicular nuclei containing small inconspicuous nucleoli,
• elongated bipolar or dendritic melanocytes containing variable quantities of fine melanin pigment indistinguishable from those seen in the common blue nevus (Figs 25.241–25.243).1
Heavily pigmented melanophages are commonly present, and the intervening stroma is frequently sclerotic. Necrosis is not a feature and mitoses are usually absent or very sparse (less than one mitosis per mm2) (Fig. 25.244).3 Cyst formation with stromal myxoid change and vascular hyalinization – features reminiscent of ancient schwannoma – are sometimes present.8–11
Many tumors show an alveolar pattern characterized by nodules of plump or spindle-shaped nonpigmented or clear melanocytes surrounded by
1301 Dermal melanocytic lesions (dermal melanocytoses)
dense collagenous septa containing dendritic and spindled melanocytes and often prominent pigmented macrophages (Figs 25.245 and 25.246). Multinucleated giant cells may be evident (Fig. 25.247). Necrosis is not a feature of benign cellular blue nevi. Mixed/biphasic (patternless) and fascicular/ neuronevoid variants may also be encountered (Figs 25.248–25.250). Intralesional perineural extension is common. Combined nevi, including an overlying junctional melanocytic nevus, are occasionally seen. Balloon cell, amelanotic, and desmoplastic variants have been documented (Figs 25.251–25.254).12–17 Occasionally, the margin of the cellular blue nevus infiltrates adjacent nerve trunks.1,18
Exceptionally, small deposits of nevus cells are found in the subcapsular sinuses and within the parenchyma of the drainage lymph nodes.16,19 They are histologically identical to the spindled cells of the parent lesion, show no pleomorphism or mitotic activity, and do not appear to represent true metastases because they do not alter the prognosis of this benign lesion in any way.
Differential diagnosis Cellular blue nevus must be distinguished from malignant blue nevus. Features in favor of the latter diagnosis include tumor necrosis, pleomorphism, and mitotic rate in excess of 1/mm2.2,13
1302 Melanocytic nevi
1303 Superficial atypical melanocytic proliferations of unknown significance

Fig. 25.239 Cellular blue nevus: large dome-shaped lesion with central blue nodule. By courtesy of J.C. Pascual, MD, Alicante, Spain.
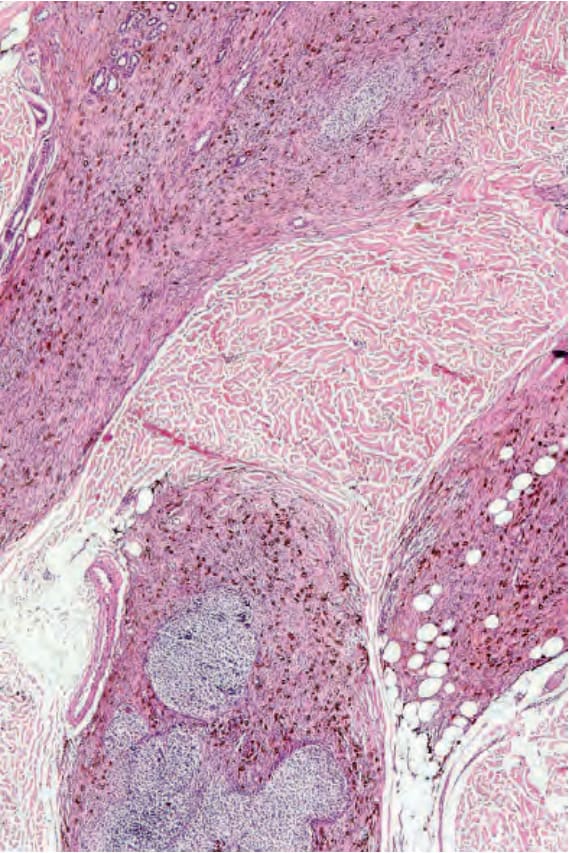
Fig. 25.240 Cellular blue nevus: this is the prototype. There is a typical dumbbell appearance.
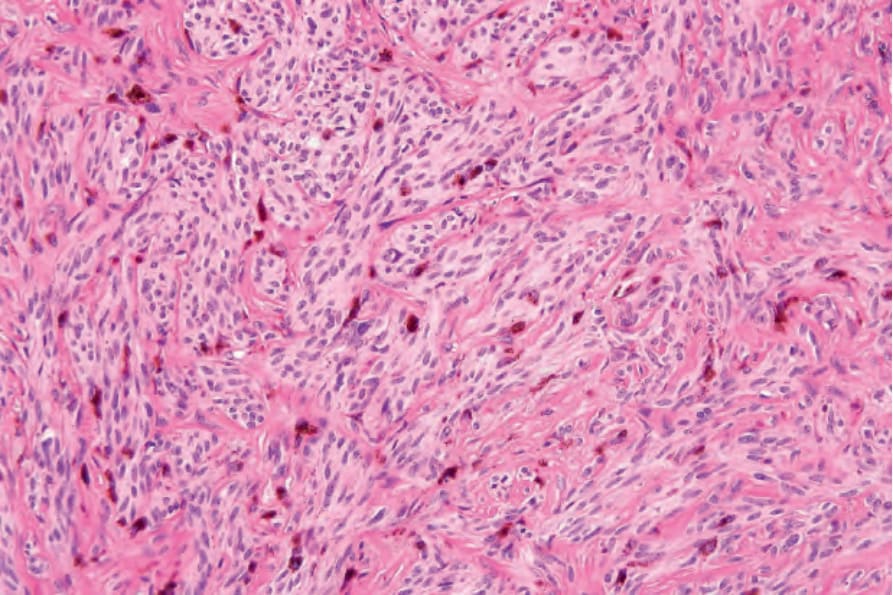
Fig. 25.241 Cellular blue nevus: the tumor is composed of a dual cell population consisting of large numbers of spindled and epithelioid cells admixed with heavily pigmented cells often arranged in an alveolar pattern, as in this example.
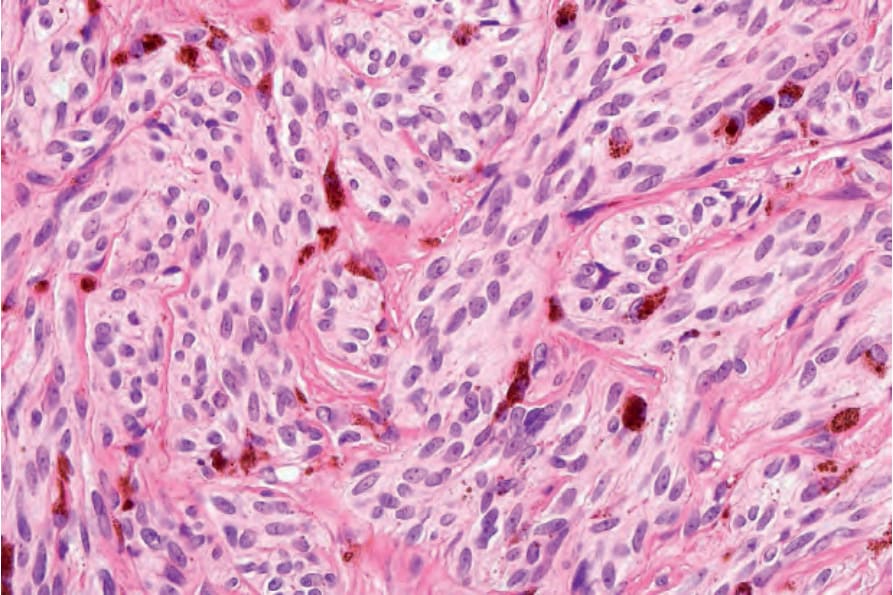
Fig. 25.242 Cellular blue nevus: high-power view. Nests of nevus cells are surrounded by fibrous septa.
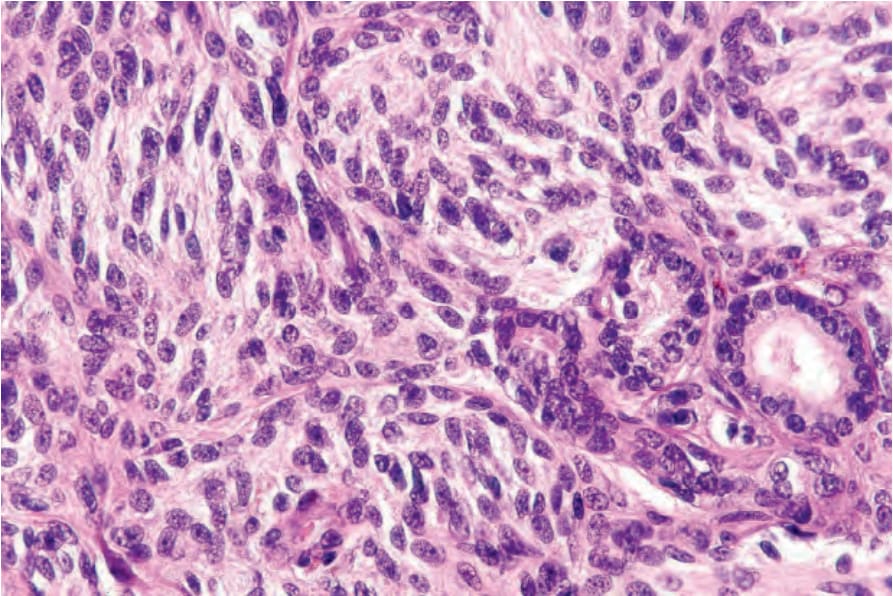
Fig. 25.243 Cellular blue nevus: there are elongated spindled cells with large oval vesicular nuclei containing prominent eosinophilic nucleoli.
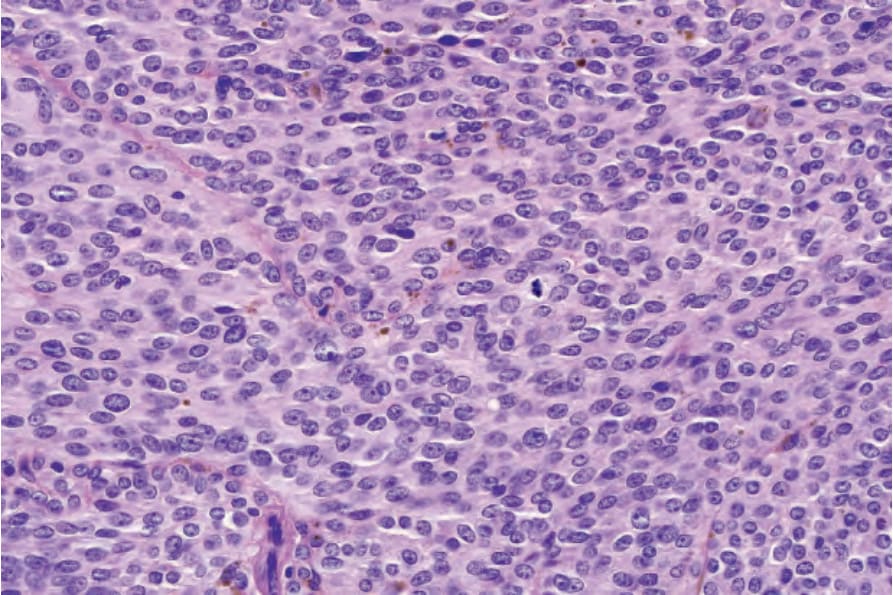
Fig. 25.244 Cellular blue nevus: mitotic figures, as seen in the center of the field, are uncommon. Atypical forms are never present.
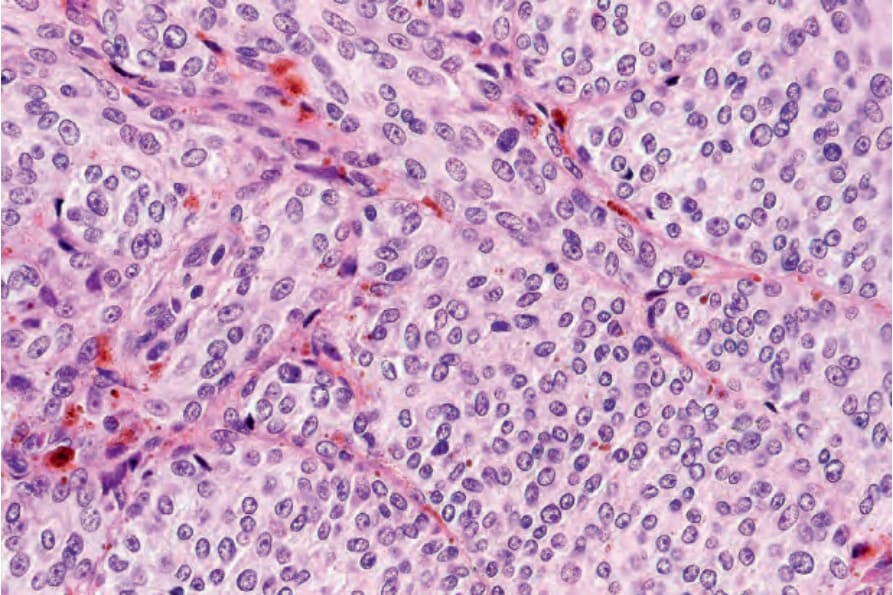
Fig. 25.245 Cellular blue nevus: an alveolar form, as shown in this field, is characteristic.
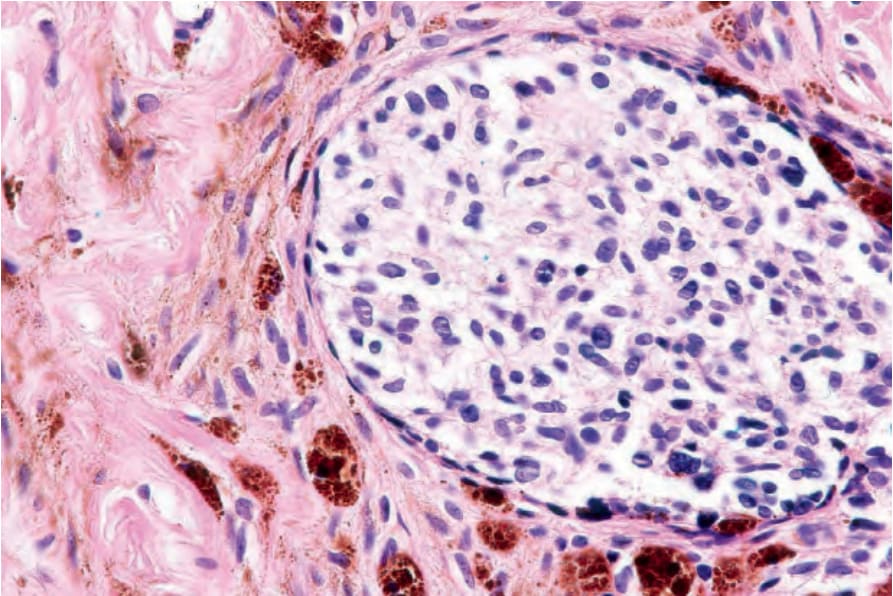
Fig. 25.246 Cellular blue nevus: note the clear cell population with surrounding spindle cells and melanophages.
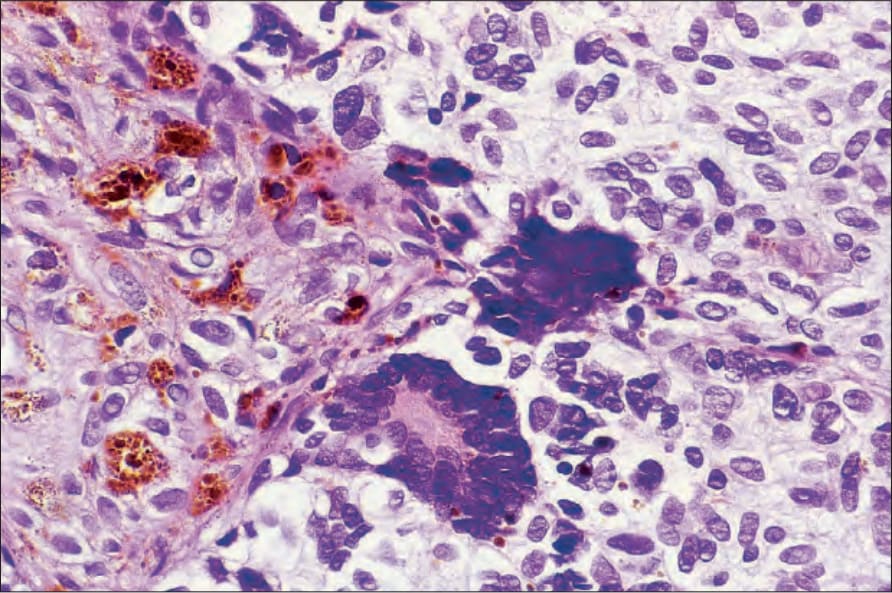
Fig. 25.247 Cellular blue nevus: multinucleated giant cells are sometimes present.
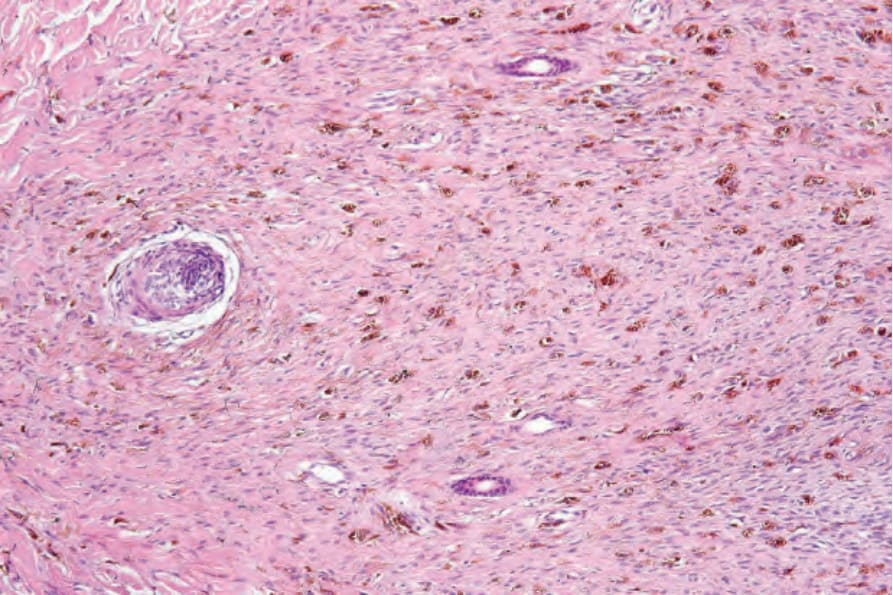
Fig. 25.248 Cellular blue nevus: low-power view of neuronevoid variant.
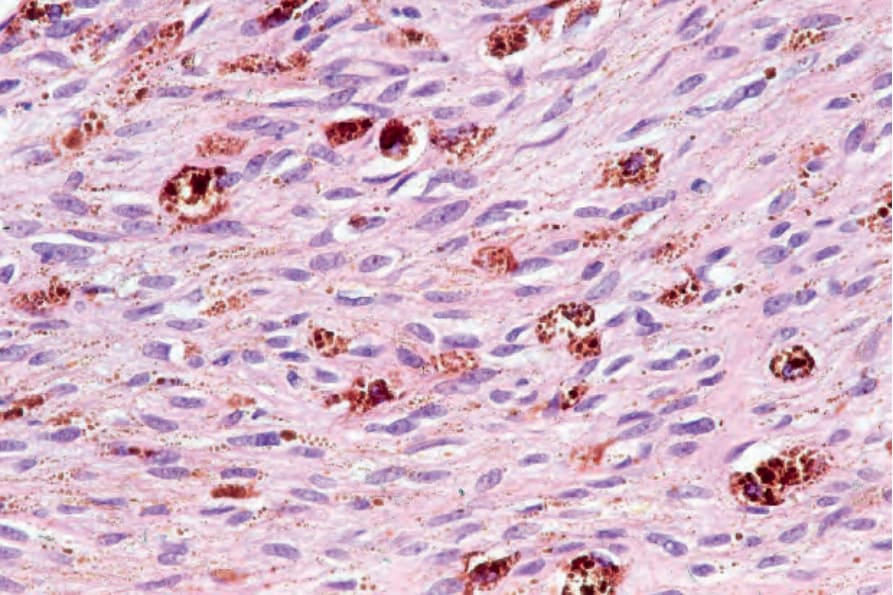
Fig. 25.249 Cellular blue nevus: the nevus cells have small twisted nuclei and pale indistinct cytoplasm in the neuronevoid variant.
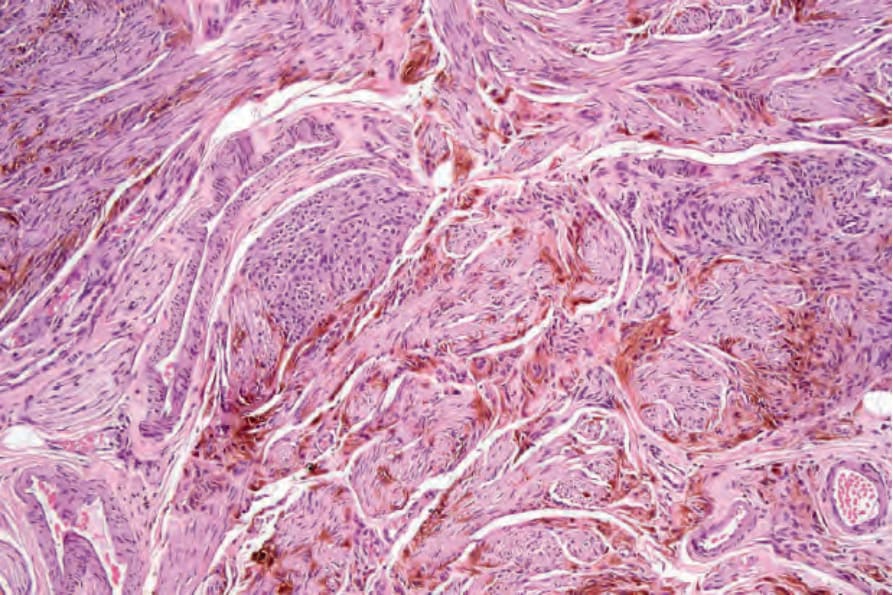
Fig. 25.250 Cellular blue nevus: this example shows a fascicular growth pattern.
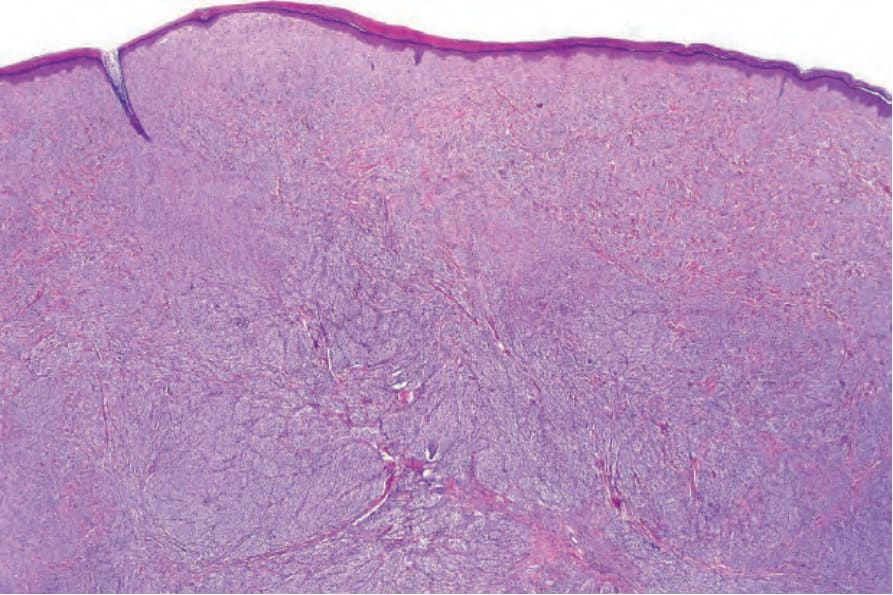
Fig. 25.251 Cellular blue nevus: low-power view of amelanotic variant.
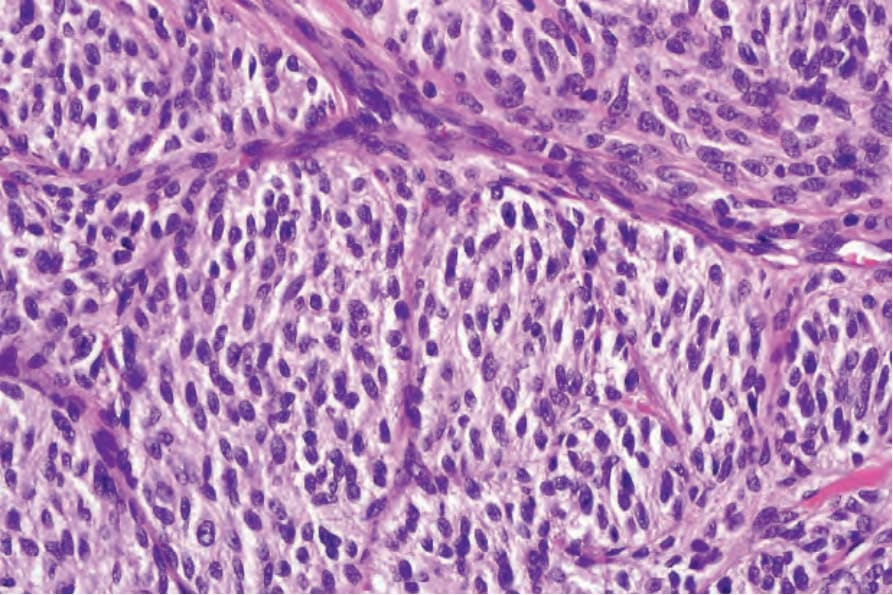
Fig. 25.252 Cellular blue nevus: this variant is composed of spindle cells with pale cytoplasm.