Epithelioid blue nevus
Epithelioid blue nevus
Clinical features Epithelioid blue nevus is a rare variant of blue nevus that has been described most often in patients with Carney complex.1,2 Small numbers of similar tumors presenting in the absence of Carney complex have also been documented.3–7 Epithelioid blue nevus has also been described in the setting of a giant congenital melanocytic nevus.8 Carney complex is an autosomal dominant condition in which patients suffer from a variety of lesions including cutaneous lentigines and blue nevi, cutaneous, mammary and cardiac myxomas, Cushing syndrome due to primary pigmented nodular adrenal hyperplasia, acromegaly due to pituitary adenoma, and sexual precocity as a result of a large cell calcifying Sertoli cell tumor. Malignant melanotic schwannian tumors (previously known as psammomatous melanotic schwannoma) is also a characteristic feature.
Epithelioid blue nevi present as blue to black or purple often dome-shaped lesions, which are most often encountered on the extremities and trunk and typically measure up to 1.0 cm in diameter.2 Mucosal (oral and genital) involvement has been described.9,10 Sometimes, multiple lesions may be encountered. An example of a generalized congenital variant has also been reported in an infant presenting with over 1000 epithelioid blue nevi.11 Sporadic lesions are morphologically similar. They are biologically benign.
Histologic features
Epithelioid blue nevus is a poorly circumscribed, often dome-shaped, oval to spherical or wedge-shaped mass within the dermis and sometimes extending into the subcutaneous fat (Fig. 25.235).2 Occasionally, combined lesions may be encountered.4 It consists of an admixture of variably sized and heavily pigmented globular cells with small vesicular nuclei and distinct eosinophilic nucleoli and polygonal cells with only lightly pigmented cytoplasm, vesicular nuclei, and single large eosinophilic nucleoli (Fig. 25.236).2 The cells are distributed interstitially, singly, in short rows, and sometimes as fascicles between the dermal collagen bundles. The adnexae are typically involved. Sparsely distributed mitotic figures may sometimes be identified. There is a background lesser population of spindled and dendritic cells. Fibrosis is not a feature of this lesion.
Some authors regard epithelioid blue nevus (both sporadic and in the context of Carney complex) and pigment synthesizing (animal-type) melanoma as part of a clinical and pathological spectrum, and use the term pigmented epithelioid melanocytoma in this context.12,13 Lesions designated as pigmented epithelioid melanocytoma seem to have a low-grade malignant potential with frequent regional lymph node metastases (up to 60%), infrequent distant metastases, and a favorable long-term clinical course.12,13 The term pigmented epithelioid melanocytoma is, however, controversial, and other authors suggest using the term pigment synthesizing melanoma to refer to such lesions.14 Further long-term studies are necessary.
The globular cells express CD68 and CD163; the epithelioid forms express S100 protein and HMB-45 but not CD68.2
Sporadic epithelioid blue nevi are morphologically identical. Epithelioid combined nevus is associated with features of desmoplastic Spitz, deep penetrating, or banal nevus.15
Differential diagnosis Epithelioid blue nevus should be distinguished from pigment synthesizing (animal-type, equine) melanoma. Cytological atypia, mitotic activity, and epidermal involvement favor the latter diagnosis.
Epithelioid and fusiform blue nevus of chronically sun-damaged skin
1299 Dermal melanocytic lesions (dermal melanocytoses)
Histologic features Superficially, pilar neurocristic hamartoma may show collections of banal intradermal nevus cells and common blue nevus-like features. In the reticular dermis, however, pigmented spindled cells surround the inferior segments of hair follicles and adjacent eccrine sweat glands (pilar neurocristic hamartoma) (Figs 25.237 and 25.238).1 The hair follicles may be reduced in number or appear dystrophic.2,16 The interfollicular dermis contains scattered heavily pigmented spindled cells and dendritic cells reminiscent of a Mongolian blue spot arising in a background of neurofibroma-like nonpigmented spindled cells containing sharply circumscribed Schwann cell nodules, sometimes associated with Meissner tactoid body-like structures.2,6,18 Floret-like giant cells have been described.2 There is no cytological atypia, and mitoses are absent. The overlying epidermis may be hyperpigmented and show
Clinical features This recently described entity represents a subtype of blue nevus with predilection for sun-damaged skin of the head and neck and extremities.1 Epithelioid and fusiform blue nevus shows female predominance (about 1.7 : 1), and most frequently presents in the seventh decade of life (from 40 to 84 years; average, 63 years) as a solitary variegated macule or papule measuring up to 1 cm in diameter. Epithelioid and fusiform blue nevus is not related to Carney complex.
The lesion is entirely benign, and recurrences following complete excision have not been reported. However, due to occurrence on sun-damaged skin coupled with mild cellular pleomorphism, nuclear atypia, and rare mitotic activity in a subset of these lesions, epithelioid and fusiform blue nevus can be mistaken for melanoma.
Histologic features The melanocytic proliferation is typically centered in the superficial dermis and consists of plexiform growth of epithelioid and fusiform melanocytes with abundant melanin-filled cytoplasm. A second melanocytic component, a conventional blue nevus can also be identified. Solar elastotic bundles are characteristically seen admixed within epithelioid/fusiform melanocytic proliferation. No significant atypia of melanocytes is seen, and mitotic activity is usually absent. Maturation of the epithelioid component is typically preserved. However, focal moderate to high grade nuclear atypia associated with nuclear enlargement, hyperchromasia, prominent nucleoli, and occasional mitotic activity (less than 1 mitosis/mm2) can be observed in a subset of these proliferations.
Differential diagnosis A plexiform growth pattern, lack of confluent high-grade atypia, low mitotic activity, and absence of atypical mitoses should aid in distinction from melanoma.
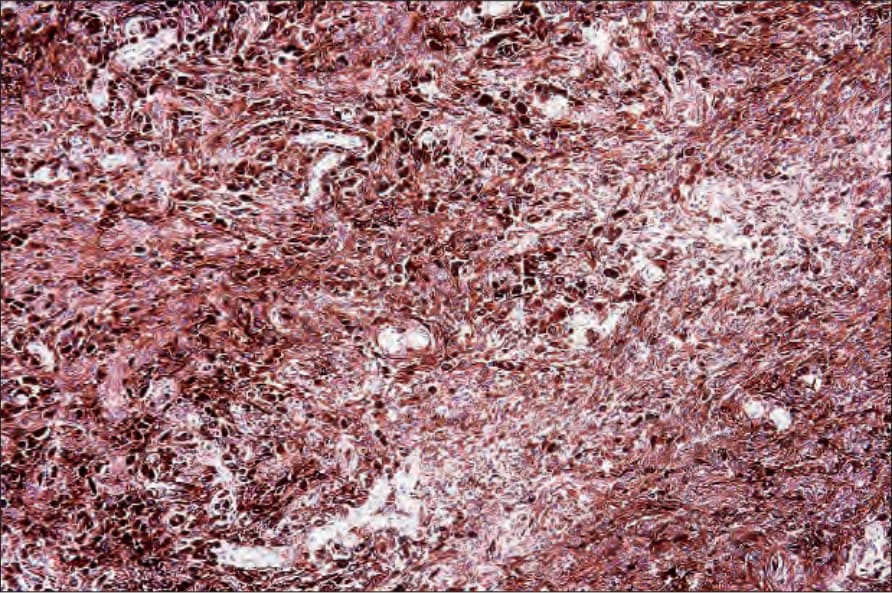
Fig. 25.235 Epithelioid blue nevus: heavily pigmented epithelioid cells are dispersed among dendritic cells and melanophages. By courtesy of C.D.M. Fletcher, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, USA.
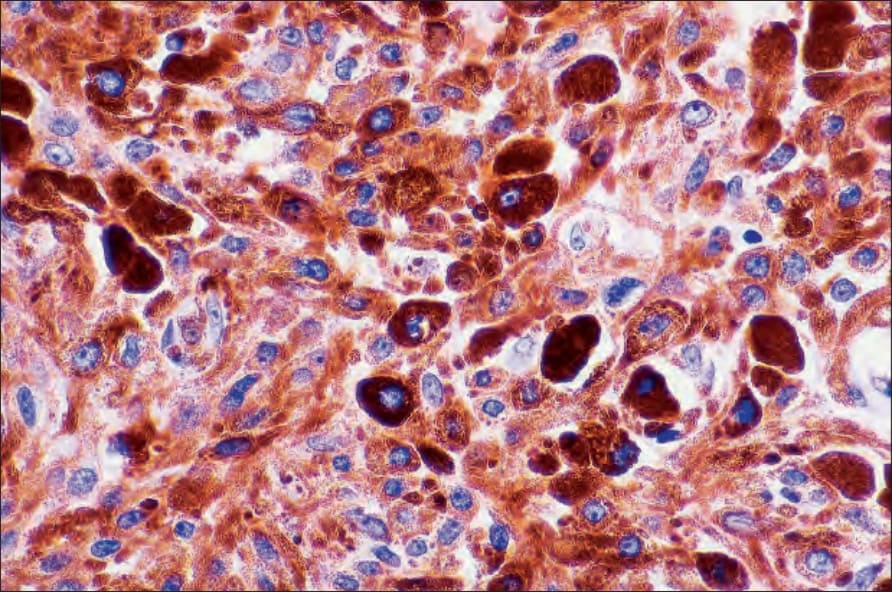
Fig. 25.236 Epithelioid blue nevus: the epithelioid cells are heavily pigmented and have vesicular nuclei with prominent nucleoli. By courtesy of C.D.M. Fletcher, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, USA.
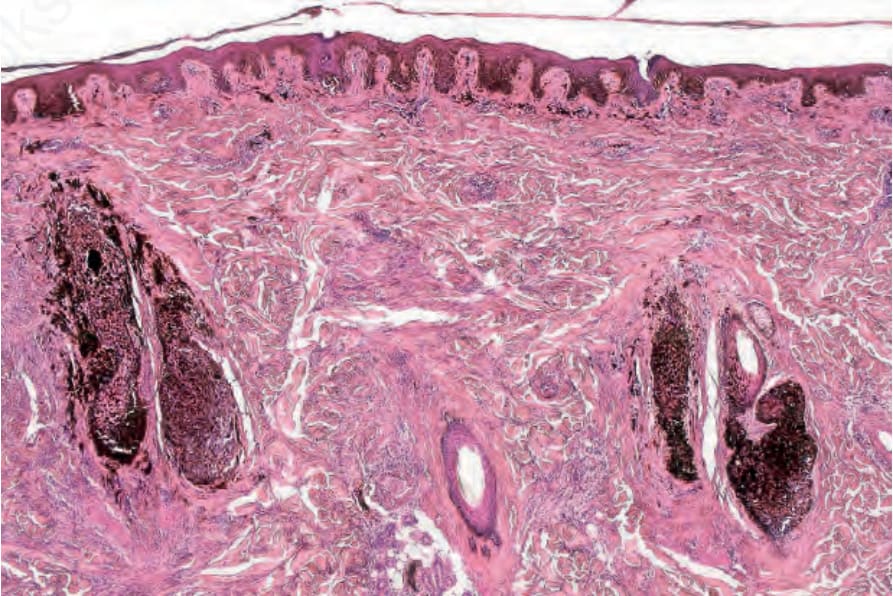
Fig. 25.237 Pilar neurocristic hamartoma: this example shows a strikingly folliculocentric lesion. The sweat glands were also involved.