Proliferation nodule within a congenital nevus
Proliferation nodule within a congenital nevus
Clinical features The proliferation nodule is a rarely encountered, benign lesion that develops within a congenital melanocytic nevus, usually but not invariably of the giant type, which both clinically and histologically may result in suspicion for melanoma. The frequency of proliferation nodules in giant congenital melanocytic nevi has been reported to be from 2.9% to 19%.1–3 Lesions generally present at birth as a smooth-surfaced brown to black papule or nodule, most often measuring less than 1.0 cm in diameter although larger variants may also be encountered.4–12 On occasion, they become ulcerated.12 Although typical lesions are solitary, occasionally satellites or multifocal lesions are encountered. In some examples, ulceration or hemorrhage heightens the clinical concern for melanoma. The natural history of proliferation nodules is one of spontaneous gradual regression. Alternatively, they remain stable over prolonged period of time, or exhibit enlargement and hyperpigmentation.6
Histologic features Several morphological patterns of proliferation can be present in proliferation nodules, the most common being expansile nodule with epithelioid (or sometimes more spitzoid) melanocytes (see below).13 Additional morphological patterns in proliferation nodules include blue nevus-like pattern with increased pigmentation of melanocytes, nevoid melanoma-like pattern, small round blue cell tumorlike pattern, and complex pattern characterized by two or more melanocytic populations.13
melanocytosis).17–23 Neurocutaneos melanosis has been found in 3% to 15% of patients with giant melanocytic nevi.24–26 The risk for neurocutaneous melanosis is associated with the size of large cutaneous melanocytic nevi and the frequency of satellite nevi.26 Although neurocutaneous melanosis may be asymptomatic, there is a significant risk of hydrocephalus or intracranial primary melanoma.17,27,28 Symptomatic neurocutaneous melanosis has been associated with poor prognosis – there is over 50% mortality within the first 3 years of the diagnosis.29 Giant nevi on extremities can be associated with hypotrophy of the affected limb.1 Association with infantile hemangioma, vitiligo, hepatic melanin deposition, hypophosphatemic rickets, and lissencephaly with absent corpus callosum has also been reported.30–34 SCALP syndrome is characterized by synchronous occurrence of nevus sebaceous, central nervous system malformations, aplasia cutis congenita, limbal dermoid, and pigmented nevus (e.g., giant congenital melanocytic nevus) together with neurocutaneous melanosis.35
In a classical example, a proliferation nodule is characterized by increased cellularity and larger melanocytes than in the background melanocytic component. Although distinctive and superficially appearing fairly well circumscribed, the nodule often blends imperceptibly at its margin with the adjacent melanocytes. However, a lack of blending with sharp circumscription is not uncommon (Fig. 25.214).12 The lesion is composed of large epithelioid or spindled cell melanocytes with abundant cytoplasm and mildly pleomorphic nuclei (Fig. 25.215). Nucleoli are small and not prominent. Intranuclear pseudoinclusions are frequently present. Mitoses are typically rare and by definition do not usually exceed 1/mm2 (Fig. 25.216). No atypical mitoses are seen. Maturation of melanocytes with depth may or may not be seen. Necrosis is not a feature. Occasionally, greater nuclear pleomorphism and macronucleoli can be observed in proliferation nodule, which is not associated with increased mitotic activity.12 A mild to moderate mononuclear inflammatory cell infiltrate composed of lymphocytes, confined to proliferation nodule can sometimes be present.12 Epidermal involvement is rare.12 However, no pagetoid spread is seen. Areas of mesenchymal differentiation, including myofibroblastic, chondroid, and osteoid, can occasionally be seen within a proliferative nodule.
Histologic features The histologic features are similar to those of the more typical congenital pigmented nevus, but the development of neuroid features is often more marked. ‘Bathing-trunk’ nevi may also show neurofibroma-like changes and foci of blue nevus formation (reminiscent of or perhaps identical to
Proliferation nodules with high mitotic activity have increasingly been recognized.9,11,14 Brisk mitotic activity (up to 30/mm2) is usually coupled with primitive cytology of the lesional cells, frequently with features of small blue round cell tumors displaying high nucleo-cytoplasmic ratio.14 These morphological features are not associated with a sinister biological behavior. Nevertheless, atypical mitoses, necroses, and expansile border are typically absent.9,11,14
Proliferation nodules can on occasion also demonstrate infiltrative yet nondestructive growth, preserving hair follicles and eccrine ducts.12
1292 Melanocytic nevi
Differential diagnosis Although exceedingly rare, dermal proliferation nodules must be distinguished from neonatal melanoma. Features, which should arouse suspicion for the latter, include marked pleomorphism, excessive mitotic activity, abnormal mitoses, and necrosis. A sharply delineated nodule, which does not merge with the adjacent nevus, is also a worrying feature (however, see above).
Distinction between proliferation nodule and neonatal melanoma can, however, be highly challenging, if not impossible on morphological grounds alone, in particular in lesions with brisk mitotic activity. A recent study detected the usefulness of H3K27me3 (an epigenetic gene silencer) immunohistochemistry in distinguishing between proliferative nodules and nodular melanomas developing in the background of congenital melanocytic nevi in childhood.15 Namely, while all 20 cases of proliferative nodules and background congenital melanocytic nevi retained homogeneous expression of H3K27me3, 80% of melanomas (4 out of 5) revealed a significant loss of nuclear H3K27me3 staining ranging from 50% to as much as over 80% of tumor cells.15 Furthermore, molecular diagnostic techniques including fluorescence in situ hybridization and CGH have increasingly been used to aid in this distinction. While proliferation nodules either display no detectable cytogenetic aberrations or show whole chromosomal copy number changes (gains or losses), melanoma on the other hand generally harbors more complex chromosomal aberrations including partial copy number gains and losses.15–17

Fig. 25.213 Giant congenital melanocytic nevus: in addition to being of cosmetic importance, lesions such as this have a significant risk of malignant change. By courtesy of the Institute of Dermatology, London, UK.
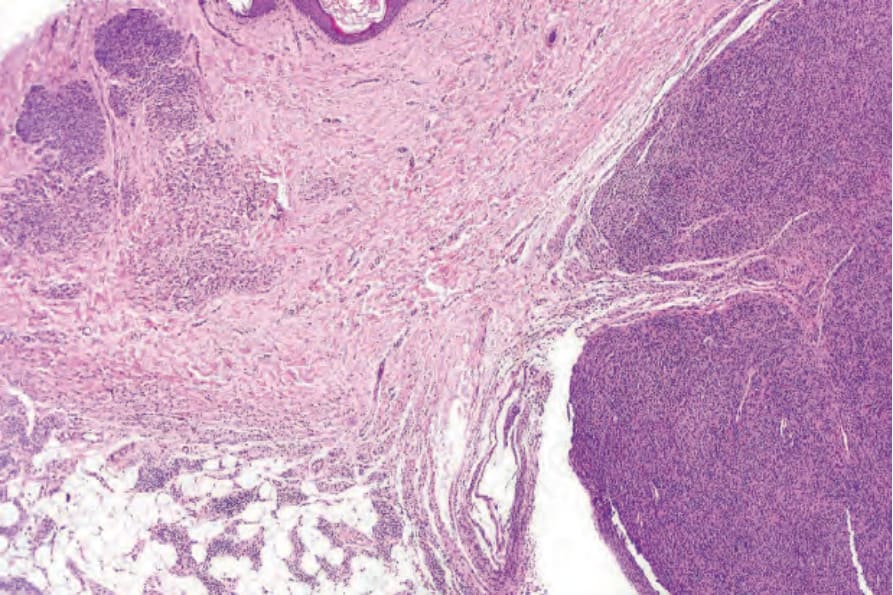
Fig. 25.214 Proliferation nodule: the congenital nevus present on the left contrasts with the hypercellular proliferation nodule of the right.
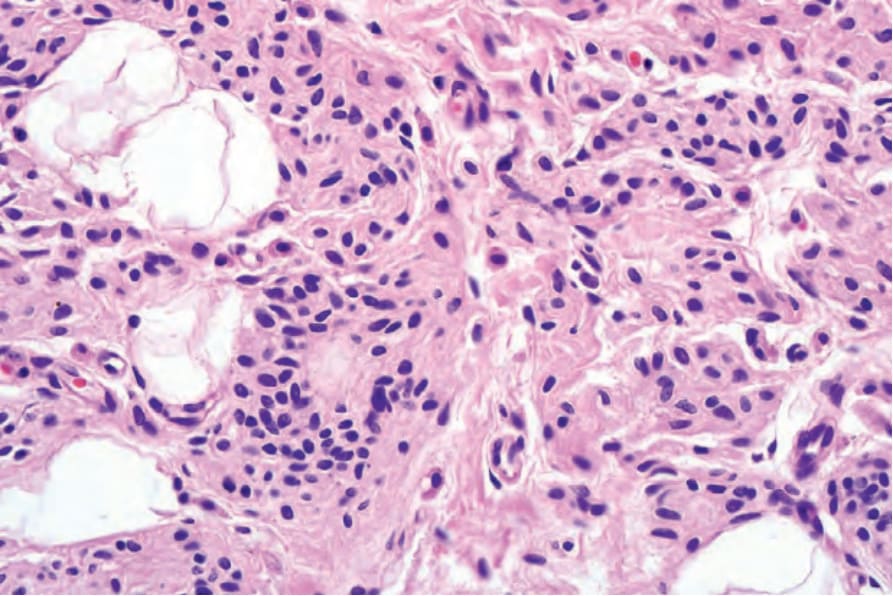
Fig. 25.215 Proliferation nodule: high-power view of the congenital nevus.
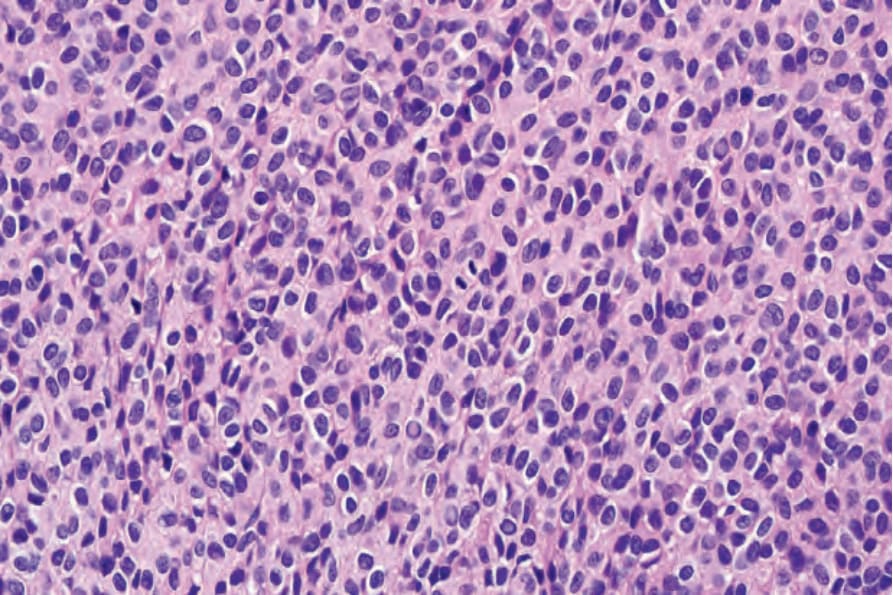
Fig. 25.216 Proliferation nodule: the nodule is composed of a uniform population of nevus cells. Note the central mitotic figure.