Congenital nevus
Congenital nevus
Clinical features Congenital nevi are common, being found in 0.6% to 1.6% of the population.1 They often have histologic features sufficiently characteristic to be distinguished readily from their acquired counterparts.2,3 Because of the risk of developing melanoma, this is more than a mere academic exercise. It is difficult to give a precise figure, but the incidence of malignant change in large congenital nevi has been documented as ranging from 3.8% to 18%.4,5 A retrospective analysis from the Netherlands demonstrated higher risk of melanoma development in females than males (14.1 vs. 6.4).6 Medium and small congenital nevi may also be a potential source of concern, but the risk of melanoma in these is exceedingly low.4,5,7–11
associated with leptomeningeal melanocytosis, hydrocephalus, spina bifida, or meningomyelocele.14 Annular dermatitis (eczema) can occasionally be superimposed upon congenital nevi.15
The lesions are present at birth and are often multiple. In general, they show predilection for trunk and legs, followed by head and neck, feet, and hands.12 By convention, they are classified into three subtypes: small (measuring up to 1.5 cm in diameter), medium (from 1.5 to 20 cm in diameter), and large (measuring over 20 cm in diameter). The last often cover a limb or large area of the trunk and are typically classified separately as giant or bathing-trunk congenital melanocytic nevi (see below). The majority of melanocytic nevi greater than 1.5 cm in diameter are most likely congenital.13 Initially, congenital nevi are flat and often pale brown, reminiscent of café-au-lait macules. Occasionally, they become more heavily pigmented, thicker, and hairy.14 They may also develop a warty surface with discrete small nodular projections (Fig. 25.197). Congenital nevi are widely distributed, and those occurring over the vertebral column are sometimes
Histologic features Congenital nevi have variable appearances. Some (particularly small lesions) are indistinguishable from conventional acquired variants.16–18 Others, especially large examples, show a constellation of changes, which in the majority of cases enables an accurate assessment (Figs 25.198–25.201).19,20 The reliable diagnosis of a congenital nevus, aside from the obvious clinical information, depends on the sum of the histologic changes rather than on any one feature in particular.
The epidermis, as with acquired nevi, often participates in the process. Frequently, there is hyperkeratosis, acanthosis, and papillomatosis, although occasionally the epidermis is atrophic. Sometimes the epithelium has a lentiginous pattern. Distinction may be made between those nevi examined in neonates and young children (see below) and those examined at a later stage.
A variety of histologic features are seen in congenital nevi.21–23 Most important is the depth of the lesion. Usually, the nevus consists of a diffuse
1288 Melanocytic nevi
infiltrate of melanocytes spreading from the papillary dermis into the deep reticular dermis and frequently involving the fibrous septa of the subcutaneous fat (Figs 25.202–25.204). Unlike acquired melanocytic nevi, there is little tendency to form discrete nests, except at the junctional zone and within the superficial papillary dermis. Not uncommonly, a grenz zone separates the nevus cells from the overlying epidermis.
Also, although an acquired nevus tends to have a well-developed fibrous stroma, congenital nevi depend on indigenous connective tissue as their supporting framework. Pigmentation is variable, being most conspicuous at the superficial aspect of the lesion. Nevus cells characteristically ensheath the epidermal appendages and very often actively involve them. Nevus cells may therefore be found within arrector pili muscles, hair follicles, sebaceous glands, and the walls of eccrine sweat ducts (Figs 25.205 and 25.206). A common finding is involvement of the perineural space and infiltration of the walls of lymphatic and blood vessels. In the context of a congenital nevus, the latter features should not necessarily be regarded as sinister. An occasional normal mitotic figure may be identified in the papillary dermal component of the tumor (Fig. 25.207).24 Acquired nevi may occasionally involve an appendage structure, but the finding of nevus cells within multiple epidermal appendages is more suggestive of congenital nevi.25
1289 Congenital nevi in neonates and young children
With increasing depth, the nevus cells adopt a single-cell array and Indian-file pattern, which are particularly evident in the reticular dermis and subcutaneous fat.
The development of neuroid features is characteristic of both congenital and acquired nevi. In congenital lesions, however, the process is often patchy and remains cellular, in contrast to the relative hypocellularity of the neuroid foci within acquired nevi.
Of the many differences between these two types of nevi, the single most important diagnostic marker of congenital nevi is permeation of single nevus cells between the collagen fibers of the deep reticular dermis and septa of the subcutaneous fat.

Fig. 25.197 Congenital melanocytic nevus: solitary large lesion showing hyperpigmentation and a verrucous surface. By courtesy of the Institute of Dermatology, London, UK.
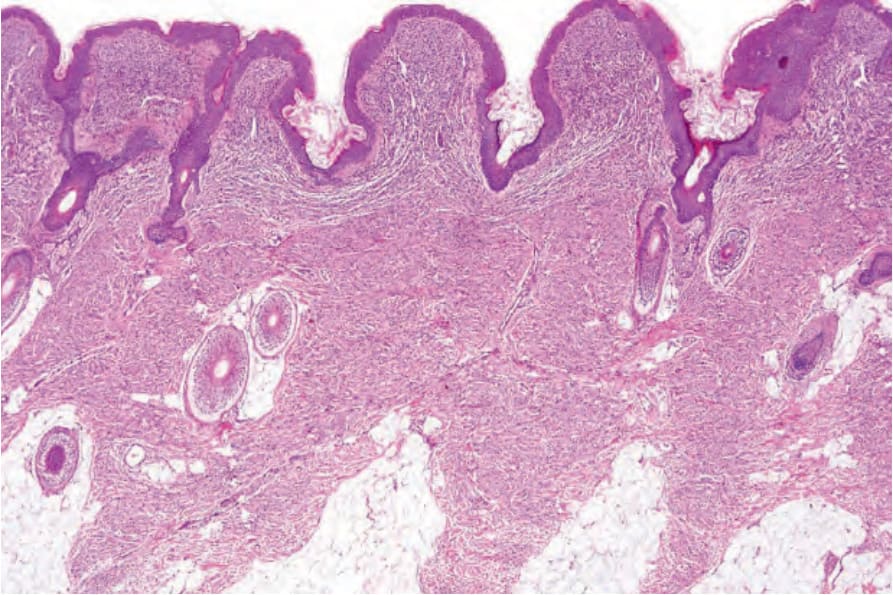
Fig. 25.198 Congenital melanocytic nevus: melanocytic proliferation extends from the superficial dermis to the septa of the subcutaneous fat. Such extensive cutaneous involvement is not a feature of an acquired melanocytic nevus.
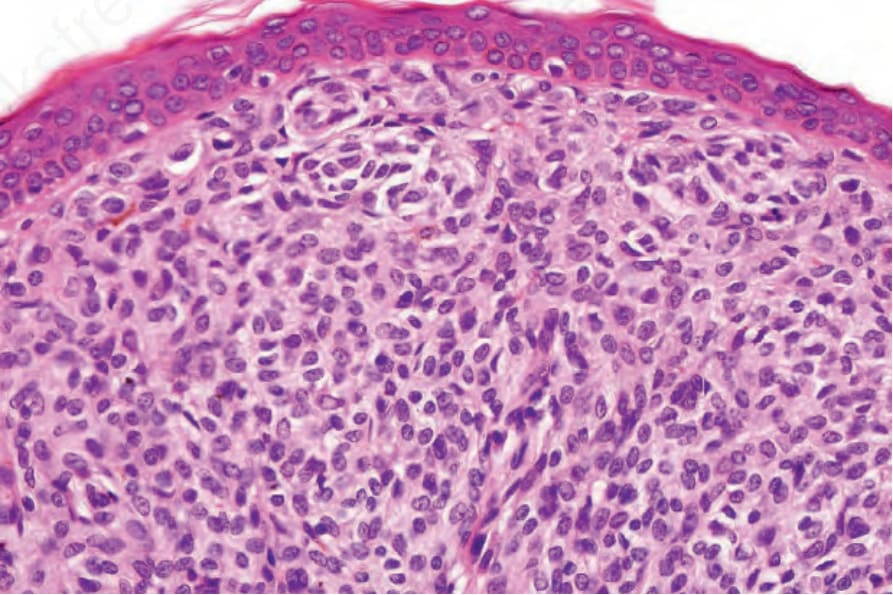
Fig. 25.199 Congenital melanocytic nevus: high-power view showing a uniform population of type A nevus cells.
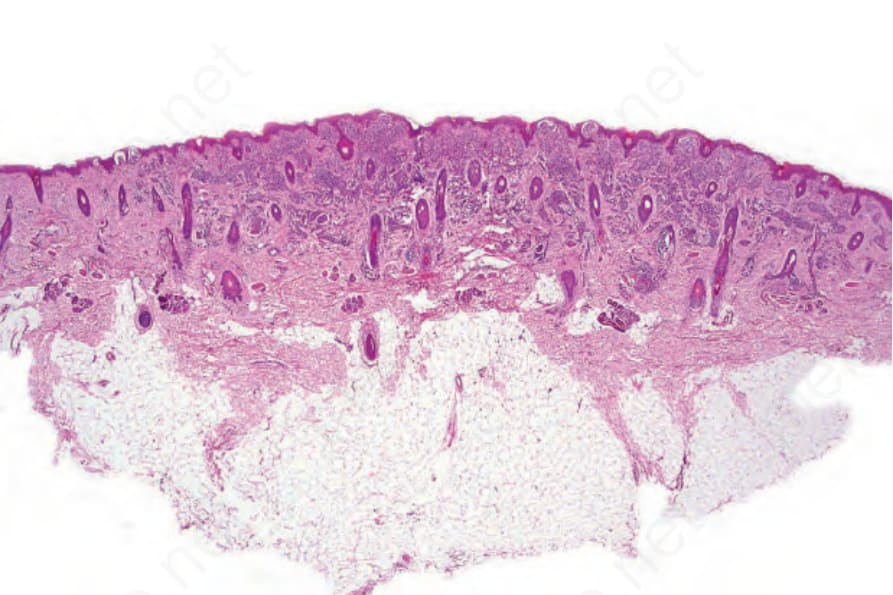
Fig. 25.200 Congenital melanocytic nevus: scanning view of a scalp lesion.
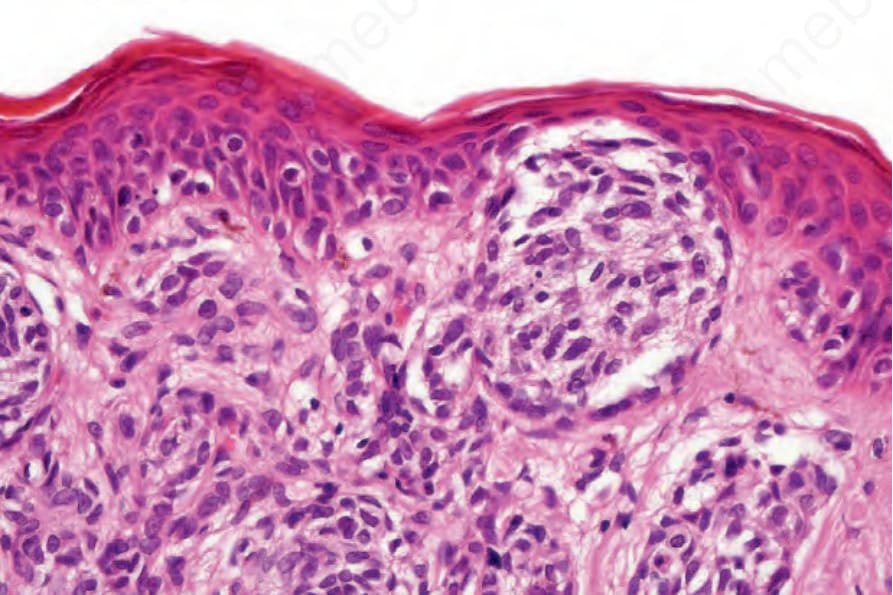
Fig. 25.201 Congenital melanocytic nevus: focal junctional activity is present.
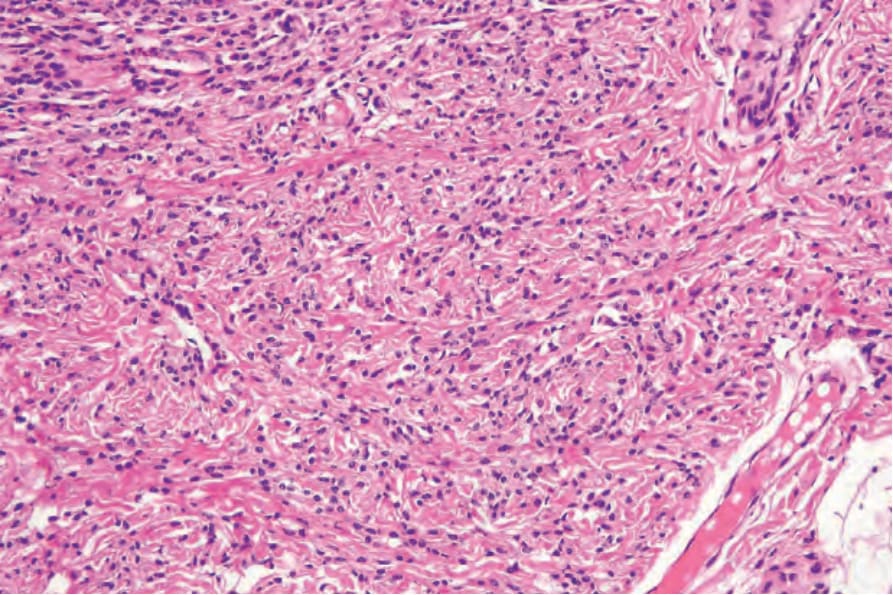
Fig. 25.202 Congenital melanocytic nevus: the nevus cells in the dermal component dissect between the collagen fibers.
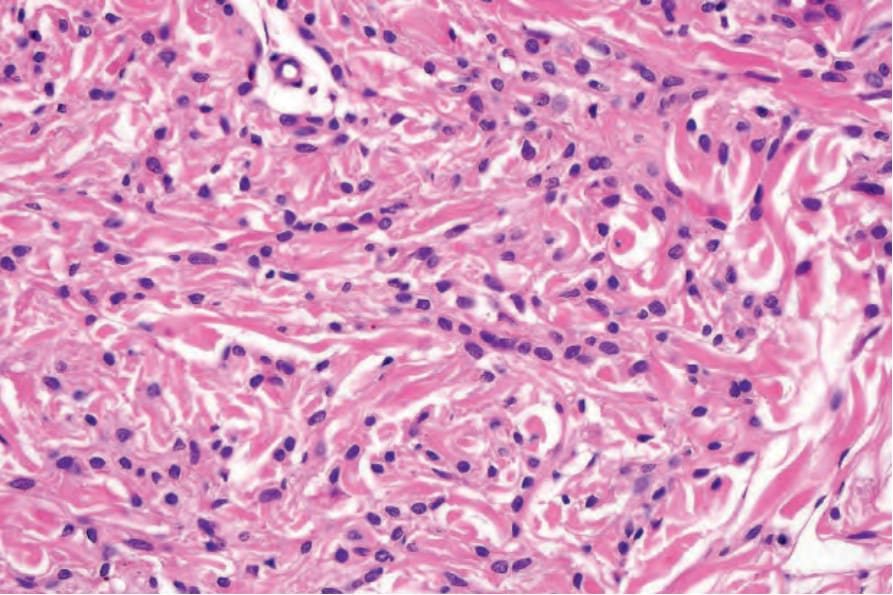
Fig. 25.203 Congenital melanocytic nevus: in this field, there is a characteristic Indian-file pattern.
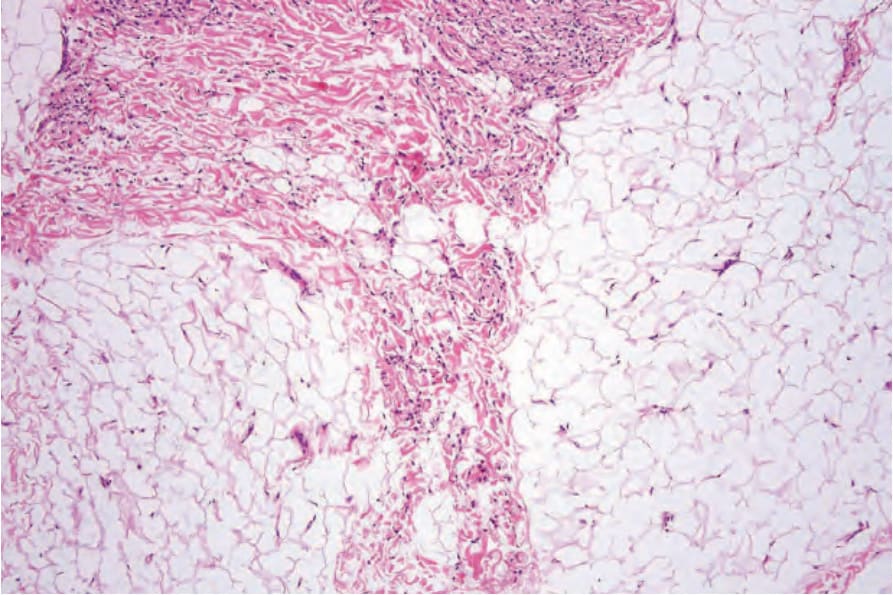
Fig. 25.204 Congenital melanocytic nevus: there is involvement of a septum of the subcutaneous fat, a typical feature.
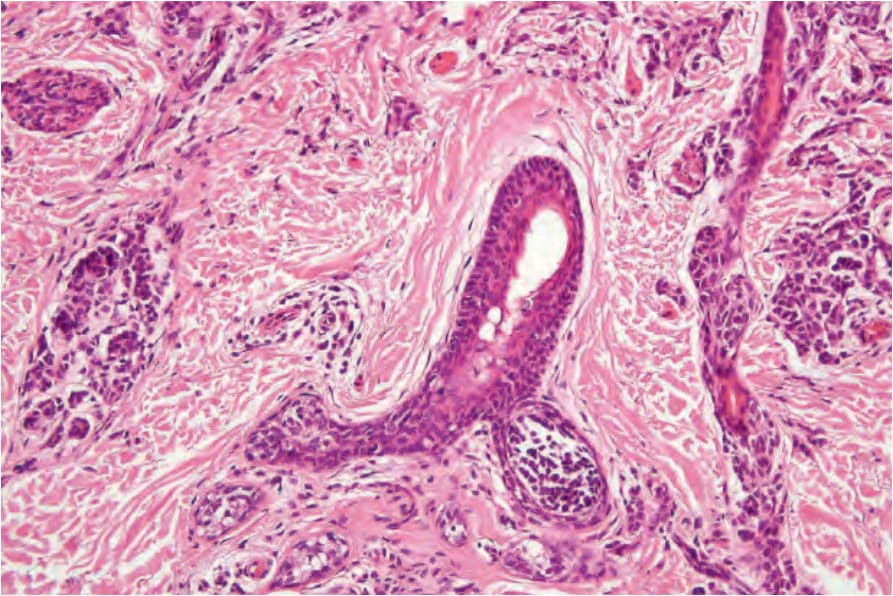
Fig. 25.205 Congenital melanocytic nevus: appendageal involvement is frequently present.
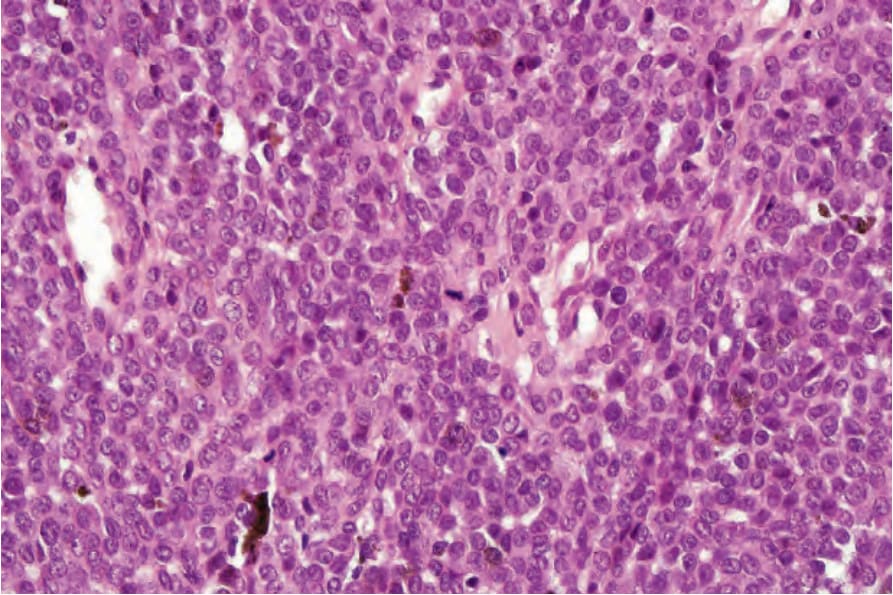
Fig. 25.207 Congenital melanocytic nevus: normal mitotic figures may be found in the superficial component, particularly in young patients. In the absence of abnormal forms and of nuclear or cytoplasmic pleomorphism, they do not imply malignancy.