Dysplastic nevus syndrome and dysplastic nevi — Part 2
1284 Melanocytic nevi
Parameter Mild Moderate Severe
1–2 × keratinocyte nucleus
2 × or greater keratinocyte nucleus
Nuclear size Approximate size of keratinocyte nucleus
Nuclear pleomorphism
Mild Moderate Severe
Chromatin Hyperchromatic Hyperchromatic or vesicular
Vesicular
Nucleolus Absent or small Absent or small Prominent and enlarged
Cytoplasm Usually little but sometimes abundant with dusty pigmentation
Usually little but sometimes abundant with dusty pigmentation
Often abundant
Modified from Weinstock, M.A. et al (1997) Archives of Dermatology, 133, 953–958.
cytological atypia should raise concern for in situ melanoma. Mitotic figures, though uncommon, are occasionally a feature. Although one or two cells may be seen in the suprabasal epidermis, any significant degree of pagetoid spread should be taken as evidence of evolving in situ melanoma. The dermal component, if present, often appears cytologically banal although in some nevi it shows superficial cytological atypia comparable to the junctional component. Sebocyte-like melanocytes, characterized by multivacuolated cytoplasm and scalloped nuclei, can exceptionally be observed in the dermal component of a dysplastic nevus.61
Cytological atypia may be classified into three grades: mild, moderate, and severe (Table 25.2; Figs 25.187–25.190).18,19 A simplification into high and low grades also has merit.62 Two studies have clearly demonstrated that the probability of melanoma development correlates with increasing grade of dysplasia, being the highest for severe dysplasia.63,64 Grading, in addition, has the benefit of drawing the clinicians’ attention to those lesions which cause pathologists most concern. It should not, however, be forgotten that on occasion one may encounter melanoma arising in a background of a dysplastic nevus with apparently only mild cytological atypia (Figs 25.191–25.193).
A recent study demonstrated site-specific and gender-related differences in histopathology of dysplastic nevi.65 Dysplastic nevi on lower extremities were smaller and more likely displayed focal pagetoid spread than dysplastic nevi on the back. While dysplastic nevi on lower extremities in females were
predominantly junctional, showed more prominent pagetoid spread, and were associated with deposition of melanin in the dermis, dysplastic nevi in males were predominantly compound nevi with little or no pagetoid spread.
A controversial entity, described as a ‘de novo intraepidermal epithelioid melanocytic dysplasia’, has been reported to be a marker of the dysplastic
1285 Dysplastic nevus syndrome and dysplastic nevi
nevus syndrome and to correlate with a familial or personal history of melanoma.66 Histologically, it is characterized by poorly circumscribed lentiginous and pagetoid proliferation of moderately to severely atypical epithelioid melanocytes within the epidermis, and may represent a precursor lesion to melanoma in situ. Distinction from melanoma in situ is difficult, and there appears to be an overlap between the two entities.
The stromal changes include an eosinophilic or more characteristic lamellar fibroblastic response; patchily distributed lymphocytes and melanophages are often evident (Figs 25.194–25.196). A subacute spongiotic dermatitis, e.g., Meyerson phenomenon, may be an accompanying phenomenon of a dysplastic nevus.67 A peculiar feature, reported in four dysplastic nevi from the same patient, was a prominent neutrophilic infiltrate within both the epidermal and dermal melanocytic components.68 The vasculature sometimes appears accentuated.
All dysplastic nevi must be carefully scrutinized to exclude the coexistence of melanoma, which is most often of the superficial spreading subtype.
It should be noted, however, that some nevi from patients with the dysplastic nevus syndrome may appear architecturally and cytologically banal.
Differential diagnosis Although any one of the above features (excluding cytological atypia) may be seen in a banal nevus, it is the combination of these features and the
1286 Melanocytic nevi
invariable presence of cytological atypia that is essential for the diagnosis of a dysplastic nevus.
Lentiginous dysplastic nevus must be distinguished from lentiginous junctional nevus and lentigo maligna. In short, the former may show minor architectural anomalies and fibroplasia but by definition, cytological atypia is absent. The clinical setting of lentigo maligna (in situ melanoma) is quite different, and the lesion is associated with epidermal atrophy rather than epidermal hyperplasia with elongation of rete ridges; solar elastosis is characteristically present. Furthermore, lentigo maligna displays non-random cytological atypia distributed throughout the lesion.69 Distinction between dysplastic nevus and lentigo maligna can be particularly challenging in small or partial biopsies.
Dysplastic nevus must be distinguished from radial growth-phase (in situ) superficial spreading melanoma. The difference, however, is subjective and
usually one of degree. Severely dysplastic nevi show a continuum with early melanoma. Although most cases are readily classified, it must be acknowledged that they form a histologic (if not biological) spectrum. Reliable morphological criteria for their distinction do not exist. Since a diagnosis of either in situ melanoma or severely dysplastic nevus generally leads to the same therapy, such distinction is of little practical importance.
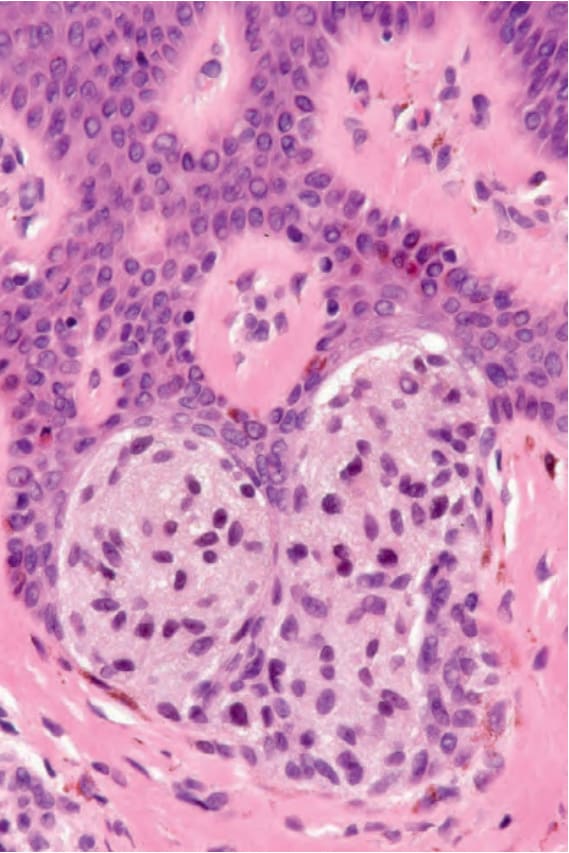
Fig. 25.187 Dysplastic nevus, mild cytological atypia: nuclei are of a similar size to the keratinocyte nuclei. They are hyperchromatic and have an irregular border. Note the fine pigmentation.
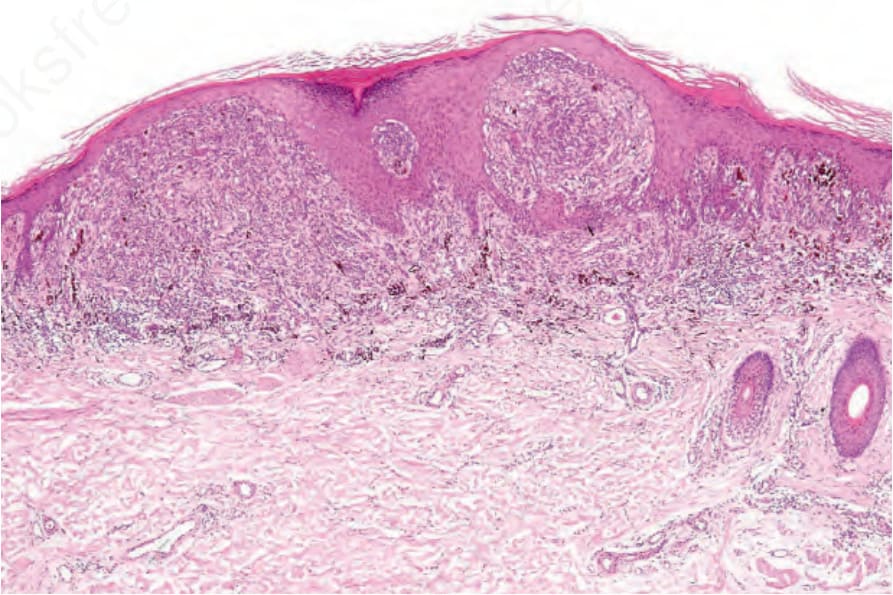
Fig. 25.191 Melanoma arising in a dysplastic nevus: invasive tumor with nevoid features.
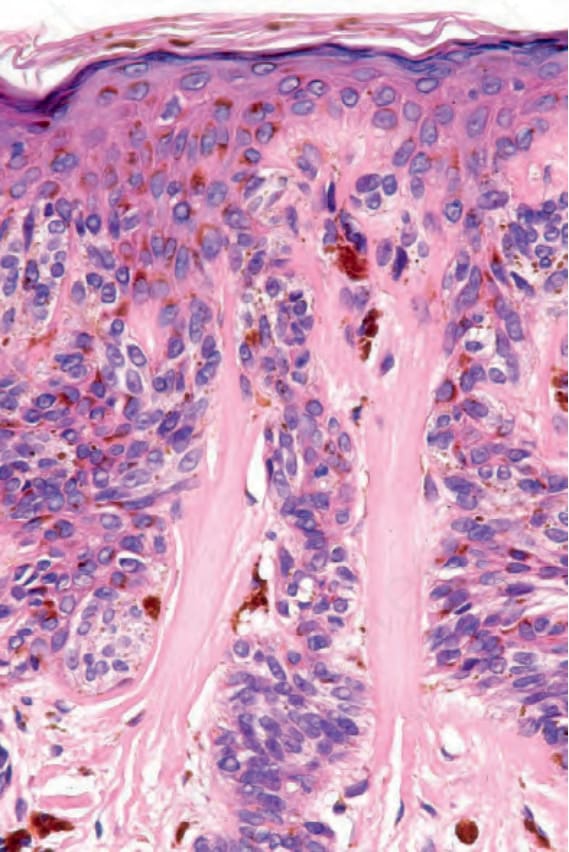
Fig. 25.194 Dysplastic nevus: there is striking eosinophilic fibroplasia.
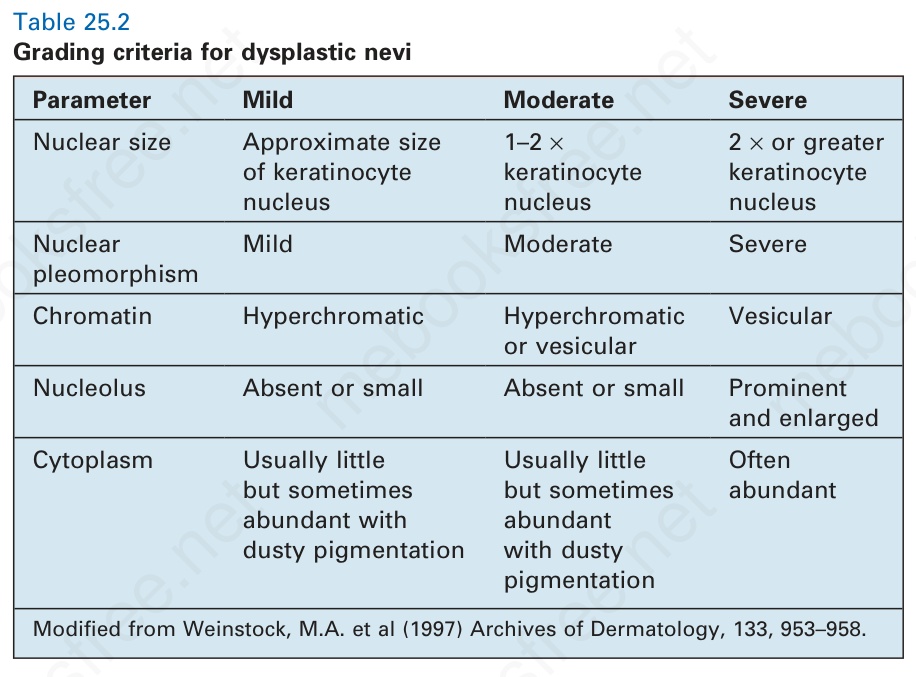
Table 25.2 Grading criteria for dysplastic nevi