Dysplastic nevus syndrome and dysplastic nevi
Dysplastic nevus syndrome and dysplastic nevi
Dysplastic nevus syndrome (familial atypical multiple mole melanoma [FAMMM] syndrome) and dysplastic nevi have been the source of considerable controversy since their original descriptions.1,2 Debate has been particularly focused on nomenclature, defining histologic criteria and their reproducibility.3–8 Numerous publications have documented varying degrees of interobserver reliability, ranging from poor when non-specialist pathologists review series of nevi to excellent when experts performed similar studies.9–19 Nevertheless, criteria by which such nevi can be recognized clinically and diagnosed histologically in the majority of cases are now well established in the literature.
It is important, however, to note that not all clinically atypical nevi are dysplastic. Thus flexural and acral nevi, for example, may be clinically and histologically atypical and of concern to both the dermatologist and the pathologist but, as defined below, they are not dysplastic. Recurrent nevi may also be disturbing to the clinician but should be readily recognized by the pathologist as of little consequence. Equally well, histologic features of dysplasia may be occasionally found in clinically ‘typical’ banal nevi and the reverse is also sometimes true, although to some extent this may be a reflection of clinical inexperience and lack of clinicopathological correlation.
The importance of the dysplastic nevus syndrome is that it identifies an at-risk population group for the subsequent development of melanoma.20–23 Although originally described as a familial condition, sporadic cases and isolated solitary lesions may also occur. The last two categories are by far the more common, with an estimated frequency of 1.8% to 17% of the population.24 The association of dysplastic nevi and familial melanoma was originally termed the ‘B-K mole syndrome’ from the initials of two of the families in the original series.1 It was also reported as FAMMM syndrome.2 Numerous synonyms have since been recommended, of which ‘dysplastic nevus syndrome’ has gained most support. The syndrome consists essentially of a tendency for the affected individual to develop large numbers of clinically atypical nevi, which histologically show dysplastic features and are associated with an increased incidence of melanoma. The histologic finding of dysplastic nevi adjacent to invasive tumor in as many as 36% of melanomas supports the hypothesis that these lesions may progress to melanoma, at least in patients with the familial variants.25 Similarly, a meta-analysis of sporadic dysplastic nevi has demonstrated a relative risk of 10.49 for melanoma developing in the presence of five dysplastic nevi.26 An even higher relative risk for melanoma development of 46.1 in patients with five or more atypical nevi was detected in a recent Dutch cohort of sporadic atypical nevi patients. However, about 7% of these sporadic atypical nevus patients were reclassified to the familial variant during the subsequent follow-up.27 Patients with dysplastic nevi have been subdivided into a variety of clinical categories (Table 25.1).25 Patients in category D2 have a 100% incidence of melanoma.28 Patients with dysplastic nevus syndrome have increased risk of developing other malignancies, particularly pancreatic cancer.29–32
Clinical features While apparently normal at birth, affected individuals develop large numbers of morphologically normal nevi in early childhood. These become more numerous and acquire atypical clinical features at or around puberty.33 New lesions continue to develop throughout life; numbers of lesions per patient range from a few to hundreds (Figs 25.174 and 25.175).33
Sites of predilection include the trunk, face, and arms, but covered sites, such as the buttocks, genitalia, breasts of females, and scalp, may also be affected. Local clustering of dysplastic nevi, i.e., agminated dysplastic nevus, has also been described.34 The nevi are usually large (6 mm or more in
- Hereditary melanoma
a. Individuals with DMN phenotype* and at least one blood relative
with melanoma (D1)
b. Individuals with DMN phenotype and at least two blood relatives
with melanoma (D2)
2. Familial DMN
Individual with blood relatives having DMN phenotype but not
melanoma
3. Personal history of melanoma
1281 Dysplastic nevus syndrome and dysplastic nevi
diameter) and irregularly shaped, frequently with an uneven or ill-defined border (Figs 25.176 and 25.177). Coloration is variable, often showing a mixture of pale and dark brown, and pink. Dysplastic nevi are sometimes surrounded by an erythematous macule (the shoulder phenomenon). The skin creases are frequently unaffected.
Clinically, these nevi tend to show marked variability both within and between patients. Although the lesions are generally macular, central nodules may develop, raising the possibility of malignancy. As patients with this syndrome, particularly those with a family history of melanoma, have an increased risk of developing melanoma, careful and frequent clinical follow-up examinations with photographic records are mandatory (Figs 25.178 and 25.179).35 Features suggestive of malignant transformation include the acquisition of contour asymmetry, excessive pigment variegation, and the development of black foci or the presence of a gray coloration suggestive of regression. The malignancies occur at a somewhat younger age than usual (mid-thirties), are sometimes multiple, and are usually located on the trunk. All relatives of patients with the dysplastic nevus syndrome should be carefully examined, because at least 50% will be found to have evidence of clinical involvement.
Individuals with both DMN phenotype and personal history of
melanoma
4. Sporadic DMN
Individuals with DMN phenotype but no personal or family history of
melanoma or a family history of DMN
*The minimum criteria for this phenotype have not been quantified. The classic presentation is one of increased numbers of both typical and clinically atypical nevi. Reproduced with permission from Elder, D.E. et al (1982) American Journal of Dermatopathology, 4, 455–460.
1282 Melanocytic nevi
Dysplastic nevus frequently reveals diverse morphological features on dermoscopy. Nevertheless, a classical example will feature a reticular pattern with thin lines, occasionally coupled with peripheral dots and clods.42 While patterns are arranged symmetrically, color variegation can be prominent.42 Most commonly, dysplastic nevus is characterized by central hyperpigmentation and uniform brown periphery.42
Pathogenesis and histologic features Familial cutaneous melanoma (dysplastic nevus syndrome) is inherited as an autosomal dominant with incomplete penetrance. It is associated with mutations of the CDKN2A gene on 9p21–22 in approximately 40% of families. CDKN2A encodes the tumor suppresser gene products p14ARF and p16INK4a.43–52 A novel atypical nevus susceptibility gene has recently been identified on 7q21.3, containing a candidate gene, CDK6.53 Loss of heterozygosity of p16INK4a and p53 genes has been demonstrated in sporadic dysplastic nevi.54,55 A dysplastic nevus syndrome associated with an inactivating germline BAP1 mutation has been reported in a proband and his son.56 Namely, in this novel kindred, the father developed multiple dysplastic nevi, BAP-deficient tumors, and conventional superficial spreading melanomas.56
Dysplastic nevi, whether familial or sporadic, show identical histologic features.57–59 The changes can be divided into architectural, cytological, and host responses. Dysplastic nevi by definition should display melanocytic proliferative changes, the latter showing cytological atypia (dysplasia) not amounting to melanoma in situ. Some authors, however, recognize dysplastic nevi on the basis of architectural changes in the absence of cytological atypia; however, they are in the minority. Such a practice is unfortunate and should be discouraged as it blurs the distinction between banal and dysplastic nevi to such an extent that it renders the concept somewhat meaningless!
A recent study demonstrated a low clinical recurrence rate of 3.6% for incompletely excised dysplastic nevi with mild to moderate dysplasia.35 A 5-mm tumor-free margin is, however, recommended for dysplastic nevi with severe atypia.36 Nevertheless, a recent study with a long-term follow-up (median, 11.9 years) of incompletely excised dysplastic nevi with severe atypia failed to detect any melanoma development at the site of previous procedure, suggesting that re-excision of previously completely excised dysplastic nevi with severe atypia may not be necessary.37
Development of clinically atypical melanocytic nevi, frequently in eruptive pattern, has been reported following chemotherapy, treatment with vemurafenib and nilotinib, administration of melanotropic peptides for tanning, but also in patients with myotonic dystrophy type I.38–41
Dysplastic nevi may be junctional or compound. In compound lesions, the epidermal component frequently extends beyond the lateral border of the dermal nevus cells. This is sometimes referred to as the ‘shoulder’ phenomenon (Figs 25.180 and 25.181).
The dysplastic nevus is characterized by lentiginous hyperplasia. The epidermis – which is usually of normal thickness, although it may sometimes be slightly acanthotic – typically shows marked elongation of the rete ridges. Effacement of the rete ridges and attenuation of the epidermis overlying melanocytic proliferation, e.g., consumption of the epidermis, are features generally not seen in dysplastic nevus and suggest melanoma.60 The nevus cells are distributed both singly along the basal layer of the epidermis (lentiginous hyperplasia) and also as nests (Figs 25.182–25.184). The latter are irregular in both shape and distribution and are not confined to the tips of the epidermal ridges, as is characteristic of the banal nevus. They therefore may be present along the sides of the rete ridges or at the tips of the dermal papillae. Bridging between adjacent nests is commonly seen
1283 Dysplastic nevus syndrome and dysplastic nevi
(Fig. 25.185). Occasionally, spindle cell nests may appear expansile, compressing the dermal papillae and resulting in a superficial resemblance to spindle cell nevus of Reed.
Cytological atypia is characterized by increased nuclear size, nuclear membrane irregularity, prominent nucleoli, nuclear and cytoplasmic pleomorphism, and variable hyperchromatism. Dusty pigmentation giving rise to an olive green coloration is characteristically present (Fig. 25.186). The atypical melanocytes may be present singly or in small clusters and characteristically appear to sit within a lacuna due to a marked fixation retraction artifact. Typically, in any one nevus there is an admixture of normal and atypical nevus cells, i.e., the cytological atypia is random. Confluent
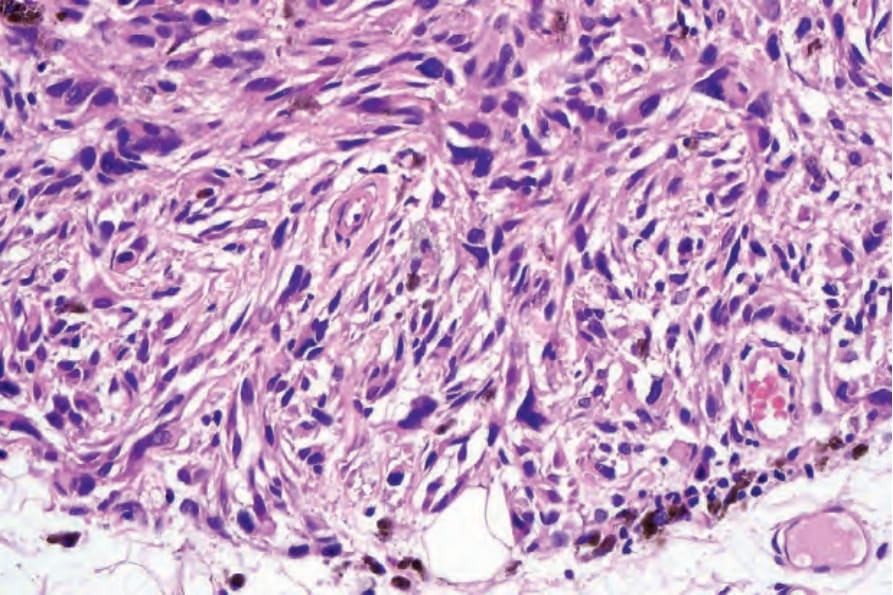
Fig. 25.172 Melanoma with deep penetrating growth pattern: there is no evidence of maturation.
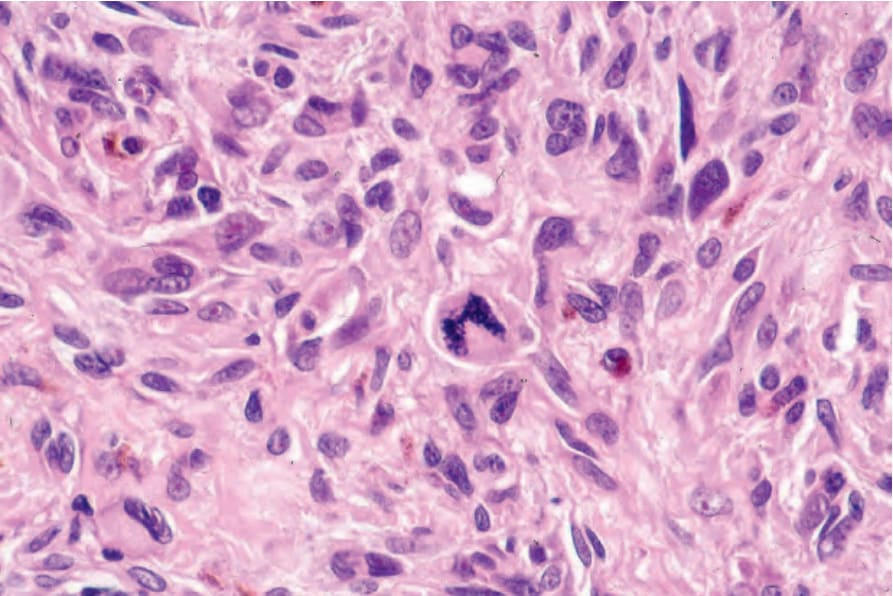
Fig. 25.173 Melanoma with deep penetrating growth pattern: mitoses including abnormal forms were present at all levels of the lesion.

Fig. 25.174 Dysplastic nevus syndrome: numerous atypical nevi are commonly present. Note the large size and irregular borders. By courtesy of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 25.175 Dysplastic nevus syndrome: the back was similarly involved. By courtesy of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
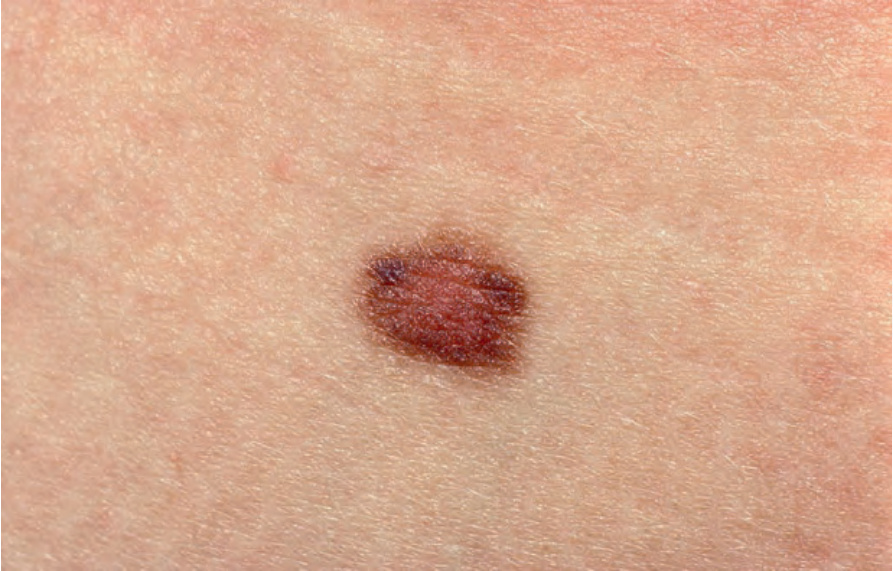
Fig. 25.176 Dysplastic nevus: nevi are often greater than 6 mm in diameter. Borders are typically irregular. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 25.177 Dysplastic nevus: there is variable pigmentation in this irregular lesion. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
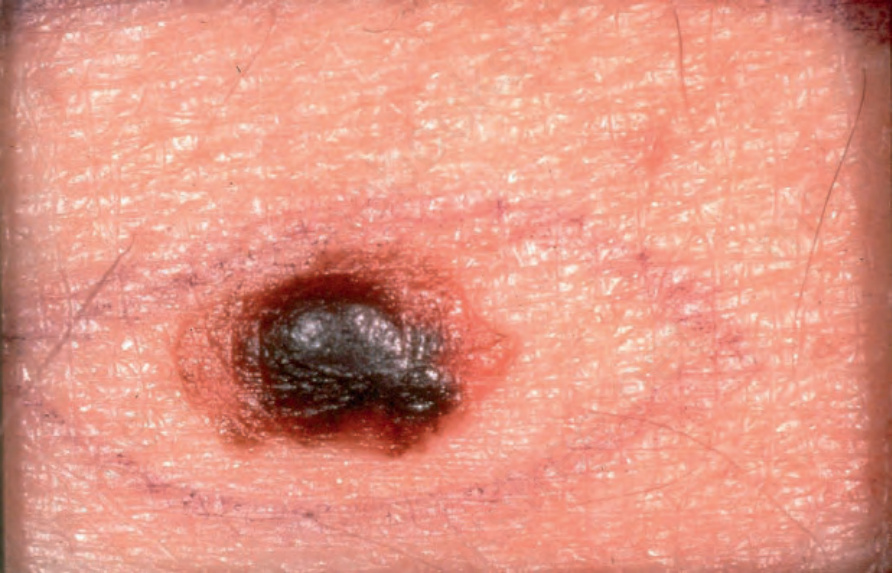
Fig. 25.178 Melanoma arising in a dysplastic nevus: note the heavily pigmented nodule. The border is highly irregular. By courtesy of J. Newton Bishop, MD, St James’s University Hospital, Leeds, UK.

Fig. 25.179 Dysplastic nevus syndrome: there are numerous large, irregular nevi. The scar marks the site of a previously excised melanoma. By courtesy of R. Mackie, MD, University of Glasgow, UK.
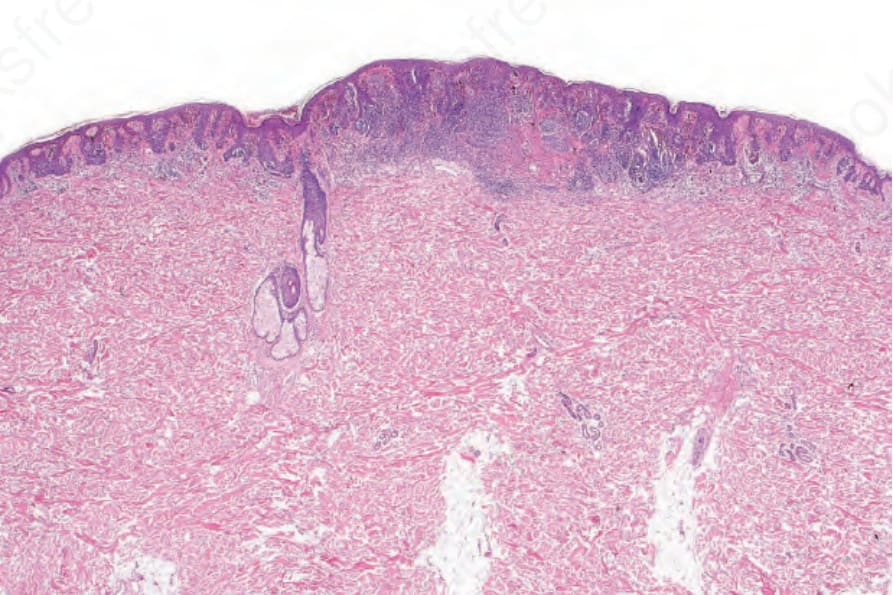
Fig. 25.180 Dysplastic nevus: compound lesion with a well-developed shoulder on either side.
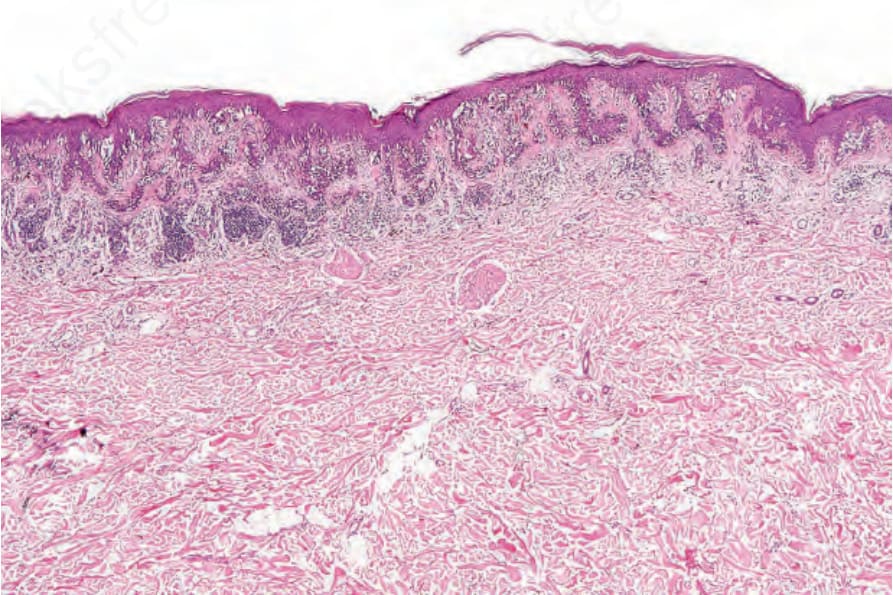
Fig. 25.181 Dysplastic nevus: medium-power view showing the typical architectural features of a dysplastic nevus. The rete ridges are elongated, junctional nests are randomly distributed, and the shoulder is clearly seen.
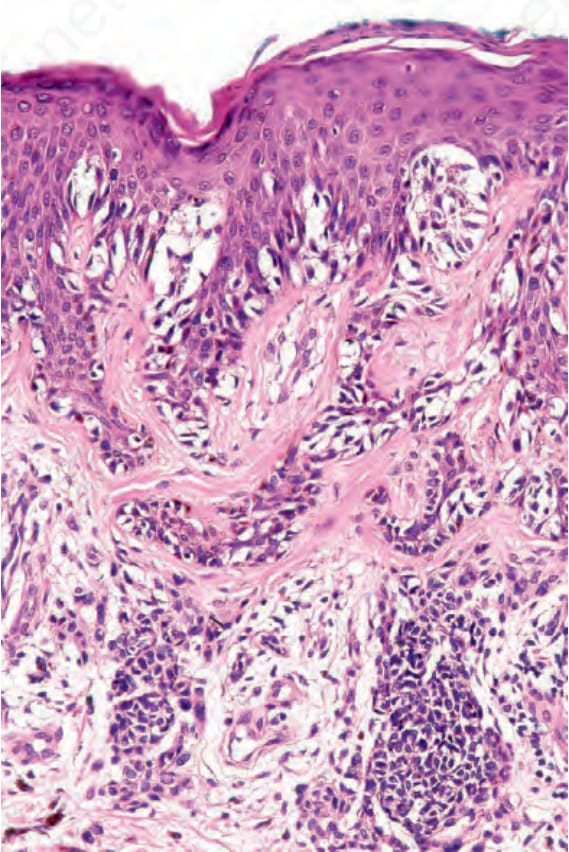
Fig. 25.182 Dysplastic nevus: high-power view of the nevus shown in Fig. 25.181. Note the lentiginous growth pattern and the abnormal location of the junctional nests along the sides of the rete and over the tips of the dermal papillae.
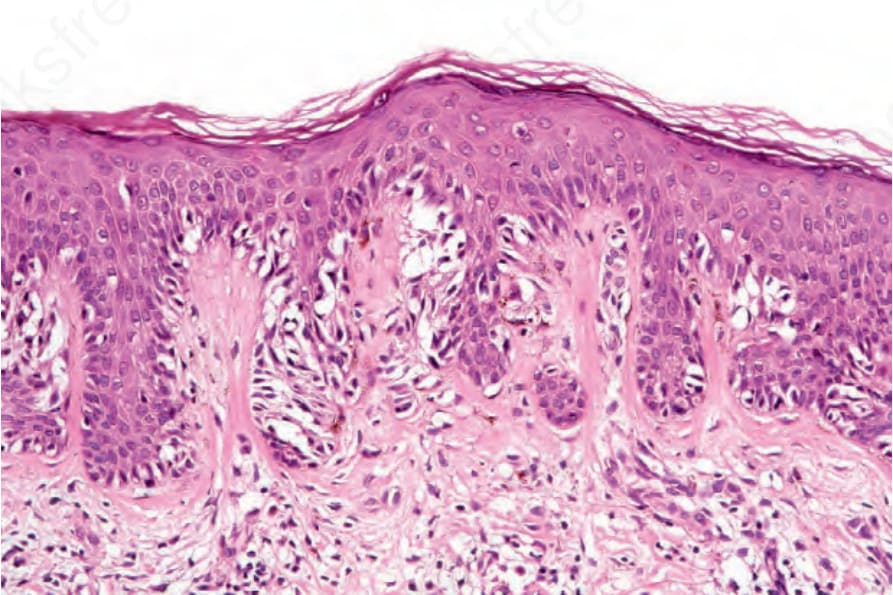
Fig. 25.183 Dysplastic nevus: the nuclei are hyperchromatic, spindled, and surrounded by a retraction artifact.
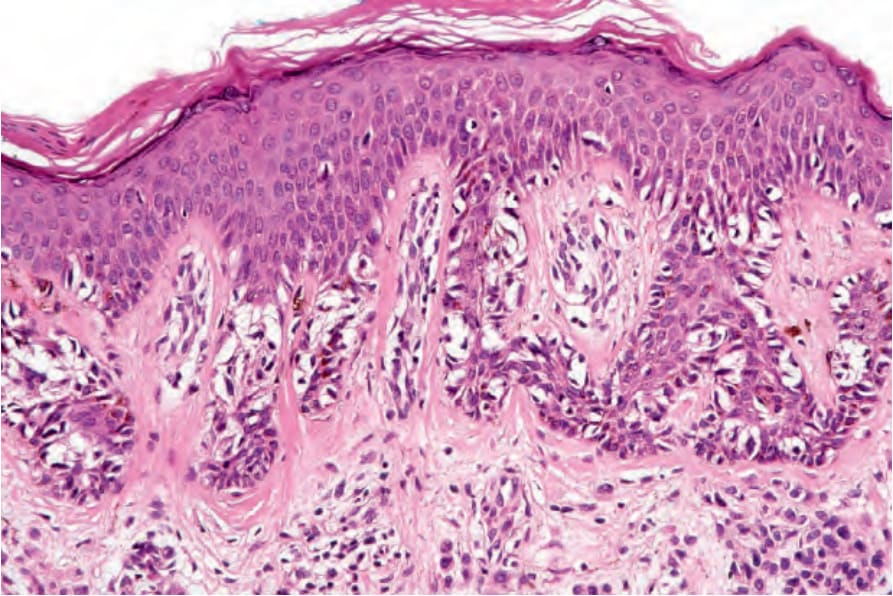
Fig. 25.184 Dysplastic nevus: in addition to nests, single cells are dispersed along the sides of the rete ridges.
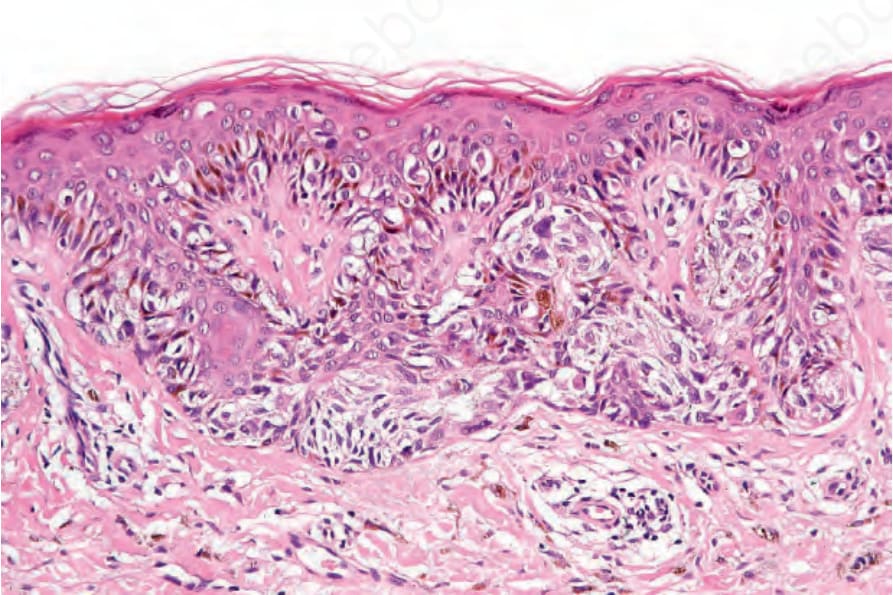
Fig. 25.185 Dysplastic nevus: bridging of melanocytic nests between adjacent rete is a common finding.
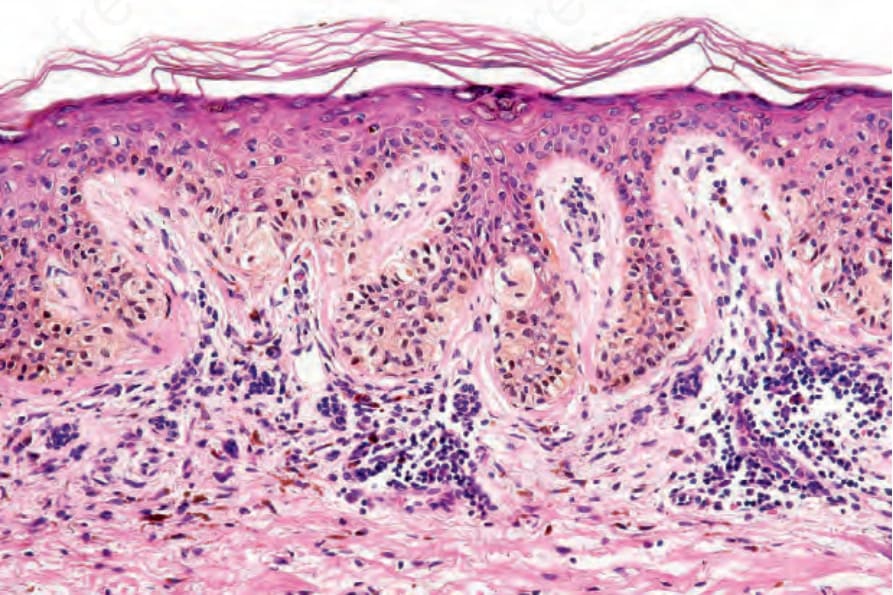
Fig. 25.186 Dysplastic nevus: dusty pigmentation often gives rise to an olive green coloration of the nevus cells.
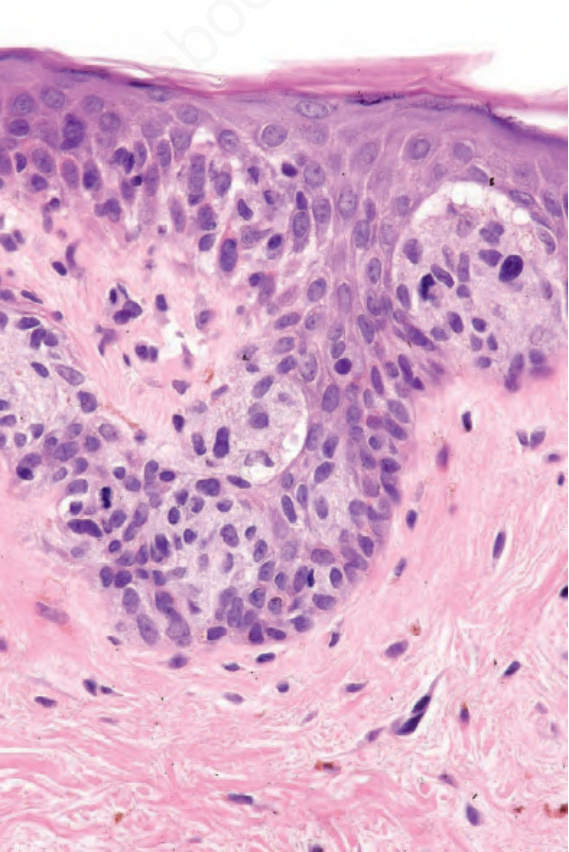
Fig. 25.188 Dysplastic nevus, moderate cytological atypia: the nuclei are variable in size. Some are larger than those of the adjacent keratinocytes. Note the mitosis.
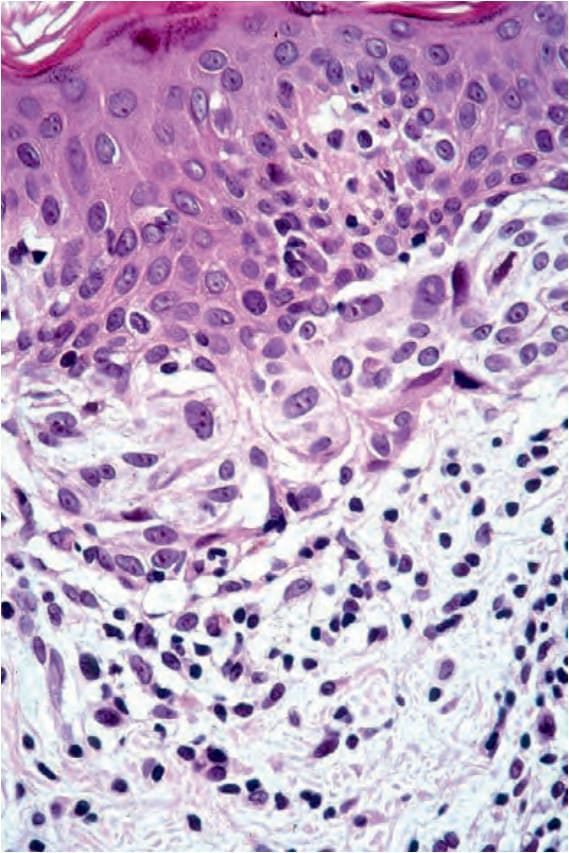
Fig. 25.189 Dysplastic nevus, severe cytological atypia: some of the nuclei are up to twice the size of keratinocyte nuclei. Nucleoli are prominent.
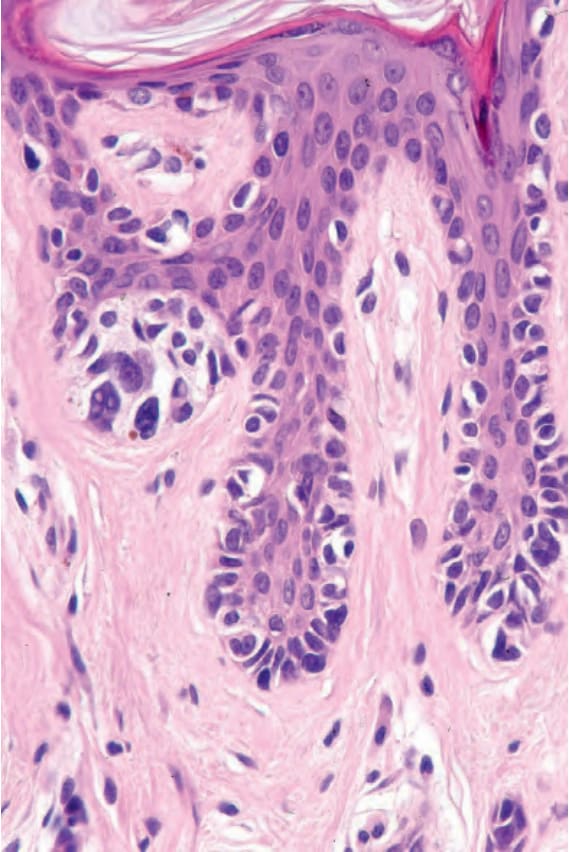
Fig. 25.190 Dysplastic nevus, severe cytological atypia: note the nuclear hyperchromatism.
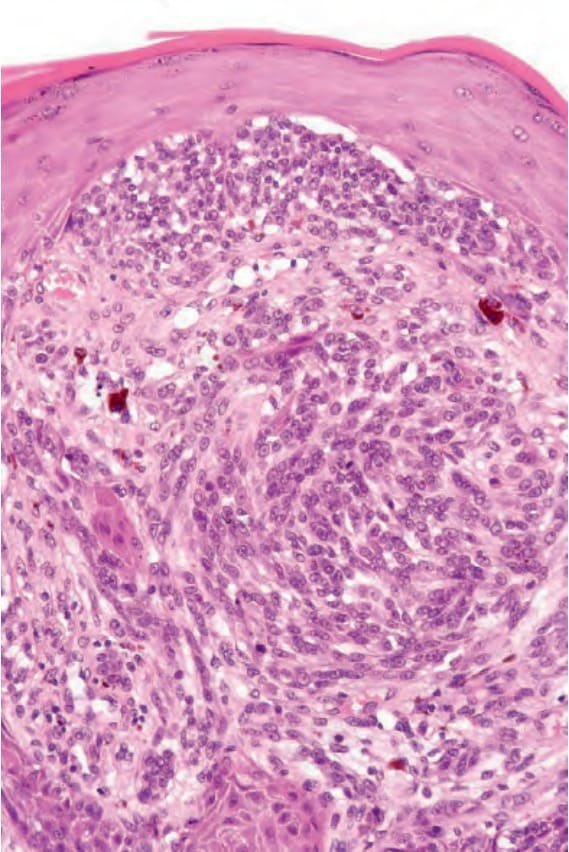
Fig. 25.192 Melanoma arising in a dysplastic nevus: close-up view of the center of the lesion.
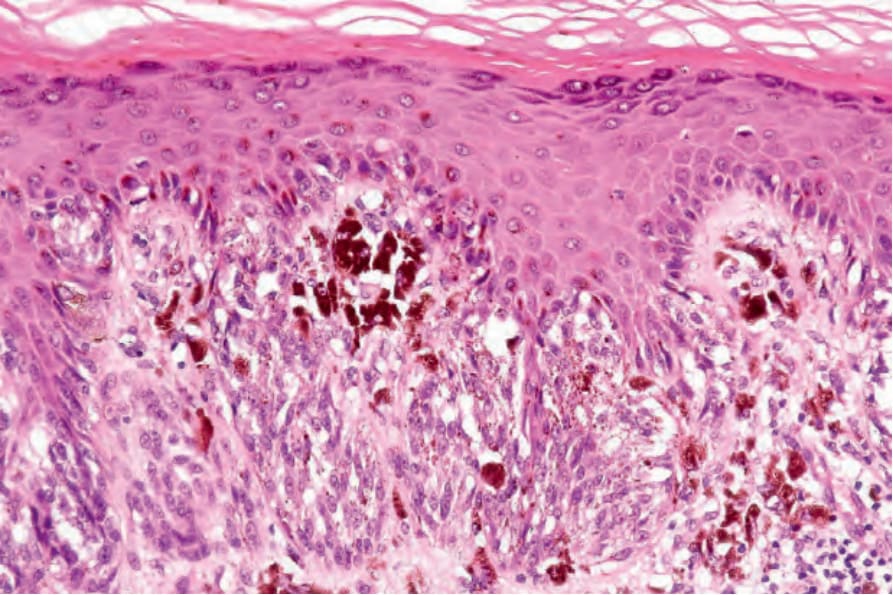
Fig. 25.193 Melanoma arising in a dysplastic nevus: the adjacent epidermis shows a junctional dysplastic lesion. Cytological atypia is mild. The patient has a long history of a dysplastic nevus that subsequently developed a nodule.
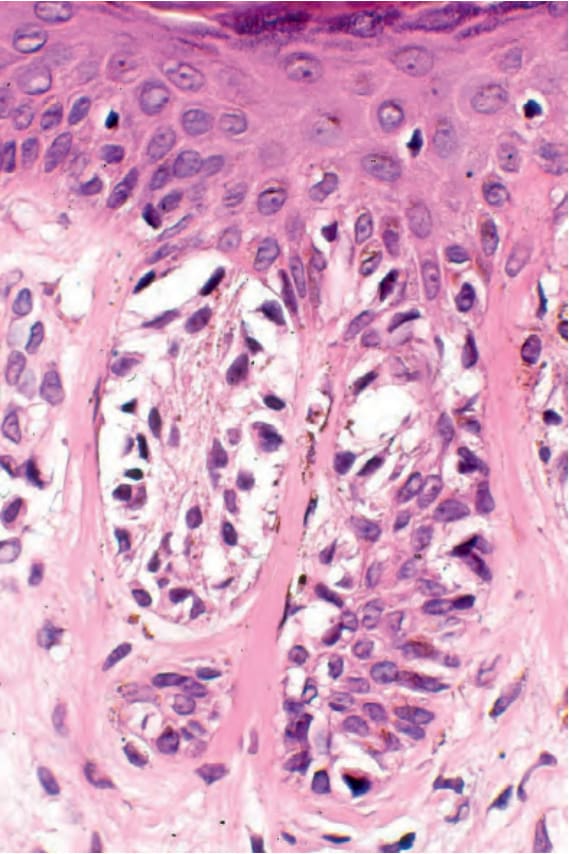
Fig. 25.195 Dysplastic nevus: note the lamellar fibroplasia.
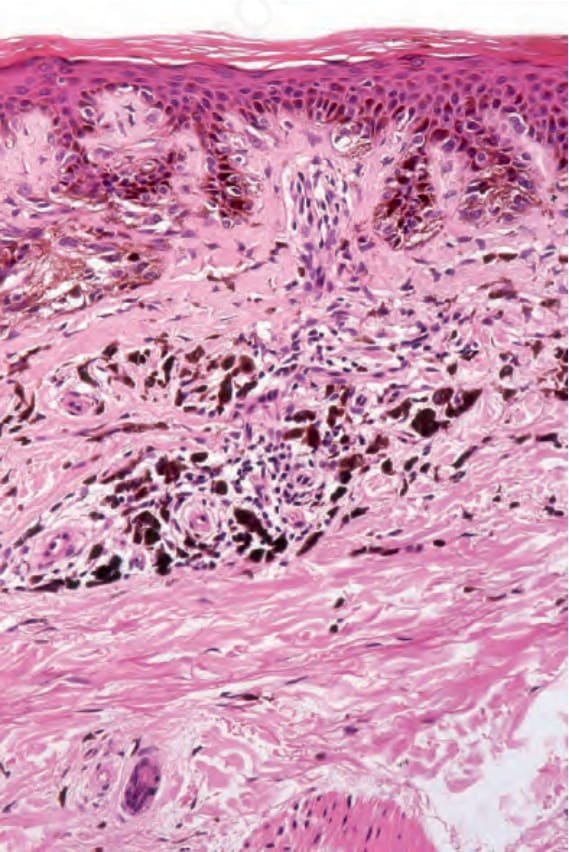
Fig. 25.196 Dysplastic nevus: in this example, pigment-laden macrophages are conspicuous.
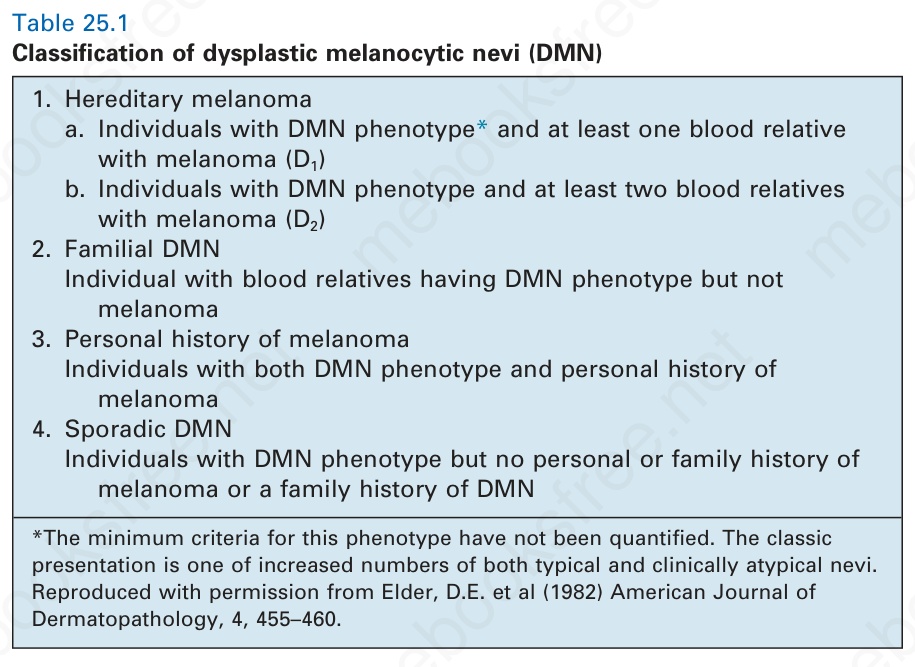
Table 25.1 Classification of dysplastic melanocytic nevi (DMN)