Deep penetrating nevus
Deep penetrating nevus
Deep penetrating nevus is a distinctive melanocytic nevus initially described by Seab et al. in 1989.1 A plexiform spindle cell nevus subsequently reported by Barnhill et al. has essentially the same histologic characteristics.2,3 Although the term ‘deep penetrating nevus’ implies extension into the deep dermis or subcutis, it is rather the combination of growth and cell morphology that define the entity. A superficial variant of the deep penetrating nevus, designated as melanocytic nevus with focal epithelioid component (clonal nevus), was reported in 1994.4 This variant shares similar age,
1276 Melanocytic nevi
anatomic distribution, and cytological features with deep penetrating nevus, but lacks deep extension of melanocytes.5
and unevenly pigmented, thus raising clinical suspicion of melanoma. The face, upper trunk, or proximal extremities are particularly affected (Fig. 25.161).1,2,5–9,11,12 A single case of a deep penetrating nevus has recently been reported on the sole of the foot.13 A unique case of linear distribution of multiple deep penetrating nevi in the preauricular skin has also been published.14 Deep penetrating nevus shows a slight female predominance (1.3 : 1).1,2,5–9
Deep penetrating nevus is difficult to categorize. While in some cases it appears to represent an entity sui generis, in other instances it represents a variant of combined nevus. The presence of dendritic cells in a significant number of cases suggests that many examples might be better classified within the blue nevus spectrum.
Clinical features Deep penetrating nevus is uncommon and of particular importance because it may be clinically and histologically mistaken for a melanoma. The age at presentation is quite broad (0–77 years), but less than 5% of deep penetrating nevi have been reported beyond the age of 50 years.1,2,5–10 Patients are most often in their second or third decade and present with a solitary, circumscribed, usually less than 1 cm diameter, dome-shaped, blue or black papule or nodule.1,2,5–9,11,12 Pigmentation can be variegated, from light brown to black, but most lesions are darkly pigmented. Especially if part of a combined melanocytic nevus, the lesion may appear asymmetrical
Histologic features A distinctive morphological feature of deep penetrating nevus at scanning magnification is its symmetrical, wedge-shaped, and sharply circumscribed configuration with the broad base uppermost, parallel to the surface epithelium (Fig. 25.162).1,9 The deep tapered component typically extends into the lower reticular dermis or even the subcutaneous fat.6,12 One or more such extensions along the skin adnexa or neurovascular bundles are frequently seen.
A junctional component is present in 60% to 85% of deep penetrating nevi, usually limited to a few small nests.1,2,5–8 Upward extension of melanocytes and pagetoid spread are not features of this lesion. In between one-third to two-thirds of cases, however, deep penetrating nevus presents as a combined lesion with banal or Spitz features as the superficial
1277 Deep penetrating nevus
component (Figs 25.163 and 25.164).15 The papillary dermis is frequently uninvolved, especially in lesions that have an exclusive deep penetrating nevus component. The dermal component is typically sharply delineated and follows neurovascular bundles and adnexal structures, often presenting a fascicular or plexiform outline (Fig. 25.165), hence its alternative designation, plexiform spindle cell nevus.2,6 The dermal melanocytic component consists of loose nests and vertically oriented fascicles of epithelioid- and
spindled-shaped melanocytes. Epithelioid melanocytes are more frequent in the more superficial parts of the lesion, and foci of clear cells are often present (Figs 25.166 and 25.167). Spindled cell melanocytes generally predominate toward the deeper reaches (Fig. 25.168). A confluence of nests may be seen, especially in the upper dermis and central areas of the lesion, but this is generally a focal phenomenon. Discohesion of melanocytes can be present at the periphery and base of the lesion. Perineural extension and infiltration of arrector pili muscle are common. No obvious maturation of melanocytes is seen. Mild nuclear pleomorphism is frequent, and nuclear hyperchromatism may be a feature. Moderate nuclear pleomorphism can also be evident, but is usually focal and random. This is not usually associated with an increase in mitotic activity. Variation in the size of the nuclei can be present within individual melanocytic nests or bundles. Nucleoli are small- to medium-sized and eosinophilic. However, mitoses are either very sparse or, more often, absent (Fig. 25.169). The number of mitosis ranges
1278 Melanocytic nevi
from 0 to 1.2/mm2.6,8 The presence of more than an occasional mitosis is a worrying feature, however, and should raise suspicion on either atypical deep penetrating nevus (see below) or melanoma with features of deep penetrating nevus. Atypical mitoses are not found in deep penetrating nevus. Intranuclear pseudoinclusions are frequently seen. The cytoplasm of melanocytes is pale pink to amphophilic. Occasional dendritic melanocytes are frequently present. A variable reactive chronic inflammatory cell infiltrate
accompanies the nevus. There is usually minimal stromal reaction. Melanophages are a constant finding in deep penetrating nevi. They can be sparse and focal or abundant and dispersed throughout the lesion. They usually surround individual nests and bundles of melanocytes and can be especially prominent at the periphery of the lesion.
The melanocytes are consistently S100 and HMB-45 positive.12 Proliferating cell nuclear antigen (PCNA) is typically expressed by less than 5% of cells.12 While HRAS mutations have been detected in 2 of 32 deep penetrating nevi, none of them demonstrated GNAQ or GNA11 mutations (commonly observed in blue nevi), suggesting possible relationship with spitzoid melanocytic proliferations.16
It has recently been demonstrated that the lesions are caused by combined activation of MAP-kinase pathway and beta catenin signaling and expression of B-catenin is retained throughout the tumor.17
1279 Deep penetrating nevus
Deep penetrating nevus is a benign melanocytic proliferation. Local recurrences are most uncommon and are usually associated with incomplete or marginal excision.5,8,12
Differential diagnosis The main differential diagnosis includes melanoma, which may rarely present with a deep penetrating growth pattern. Points of distinction include absence of atypical junctional melanocytic component, non-random cytological atypia of dermal melanocytes, more severe pleomorphism, nucleolar prominence, excessive mitoses (including abnormal forms), and impaired maturation (Figs 25.170–25.173).
A concept of atypical (or high grade) deep penetrating nevus has been proposed for proliferations fulfilling one or more of the following histologic features: lesional diameter greater than 5 mm, asymmetry, poor circumscription, involvement of subcutis, increased cellularity, nodular or
sheetlike growth, moderate to severe cytological atypia, and mitotic activity greater than 2/mm2.18 Limited available data on atypical deep penetrating nevi suggest possible development of lymph-node deposits in a subset of the lesions, yet the outcome may not be unfavorable, drawing the parallels with the so-called atypical Spitz tumors.18–20 Furthermore, atypical deep
1280 Melanocytic nevi
penetrating nevi generally lack copy number aberrations typical of melanoma by either FISH or CGH.19,20
Benign melanocytic lesions that should be distinguished from deep penetrating nevus include common and cellular blue nevi.21 While common blue nevi consist of pigmented spindled-shaped and dendritic melanocytes within a sclerotic stroma, cellular blue nevi are composed of nests and fascicles of poorly pigmented melanocytes with ovoid nuclei, inconspicuous nucleoli, and clear cytoplasm.
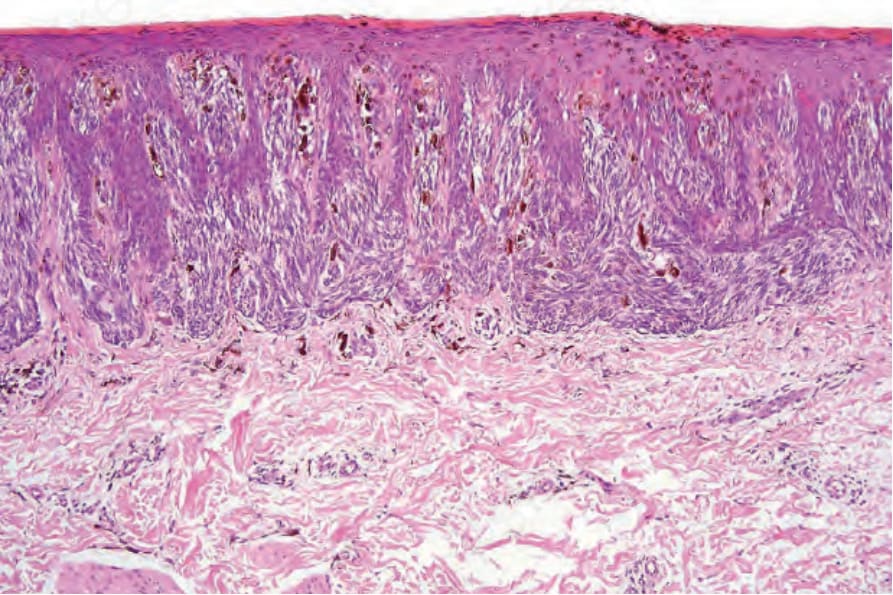
Fig. 25.155 Pigmented spindle cell tumor of Reed: the dermal papillae are distended by junctional nests of spindle cells. The presence of occasional nevus cells in the upper epidermis, particularly in the center of the lesion, is not uncommon and when taken in the context of the overall appearances of the lesion should not be a source of alarm.
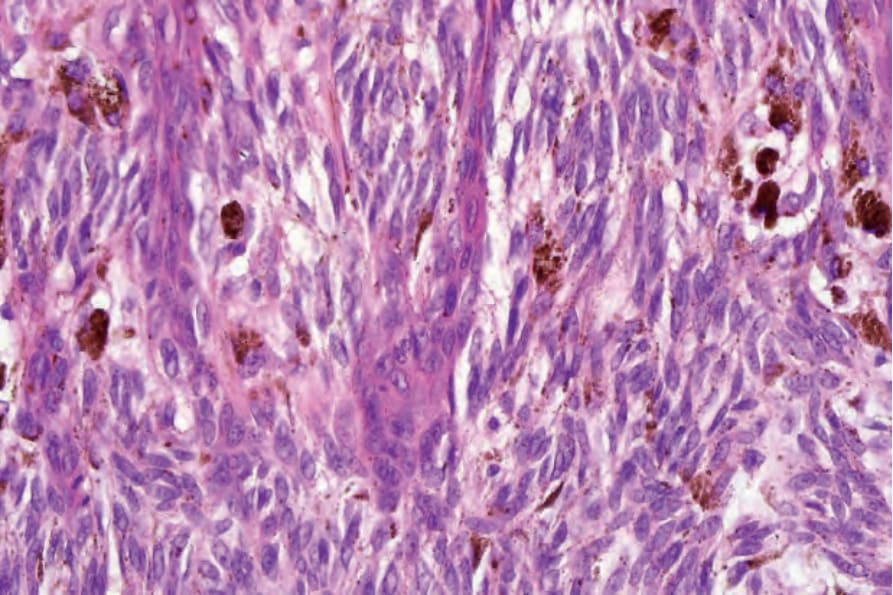
Fig. 25.156 Pigmented spindle cell tumor of Reed: the nevus cells have tapered vesicular nuclei with small nucleoli. Note the lack of pleomorphism. Heavily pigmented melanophages are also evident.
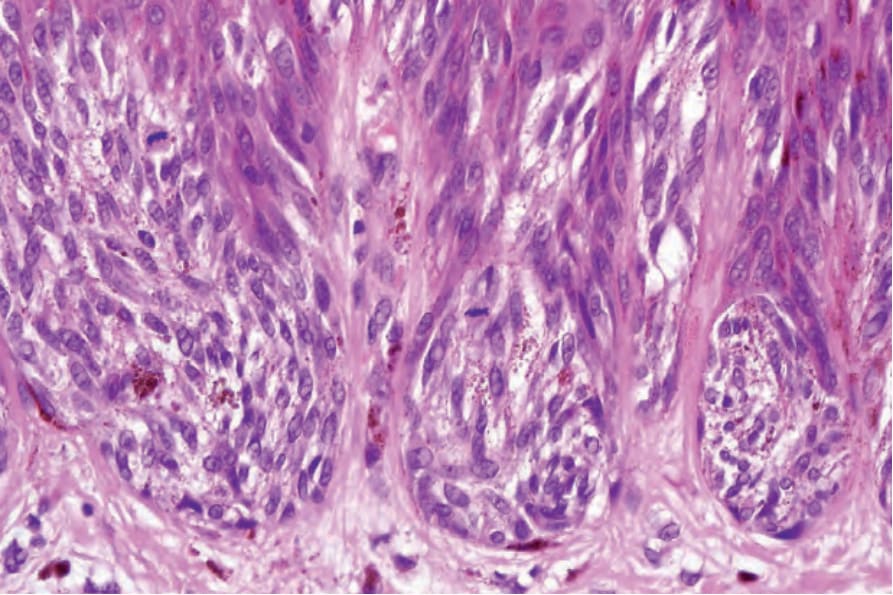
Fig. 25.157 Pigmented spindle cell tumor of Reed: junctional mitotic figures, as seen in this field, are not uncommon and should not necessarily be a source of concern unless numerous or atypical.
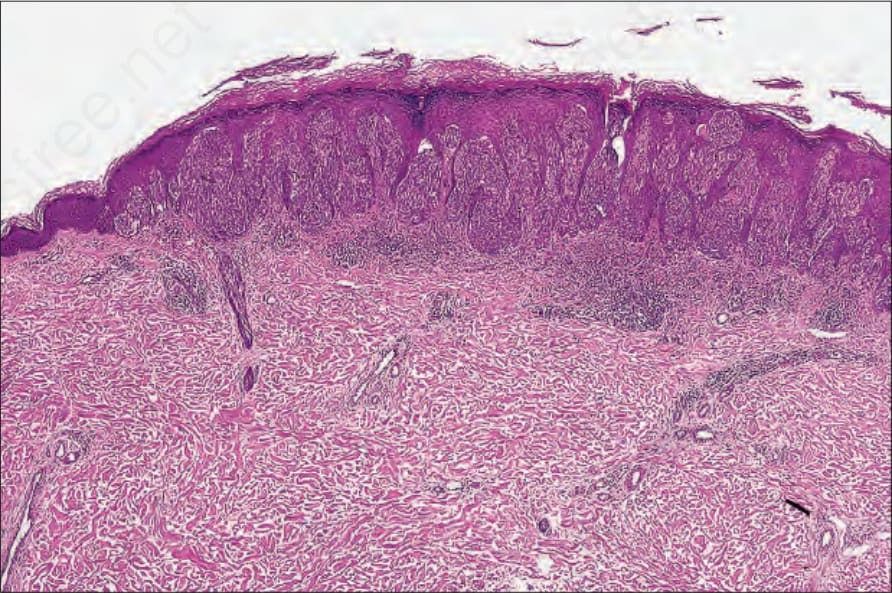
Fig. 25.158 Spindle cell tumor of Reed: low-power view of an amelanotic example. There is obvious overlap with Spitz nevus.
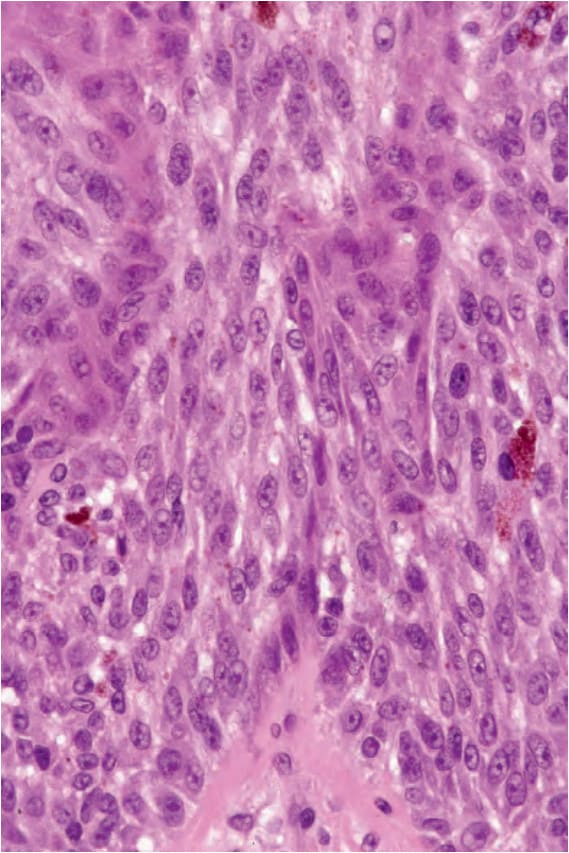
Fig. 25.159 Spindle cell tumor of Reed: careful search usually reveals small foci of melanin pigment. The nuclei are very uniform.
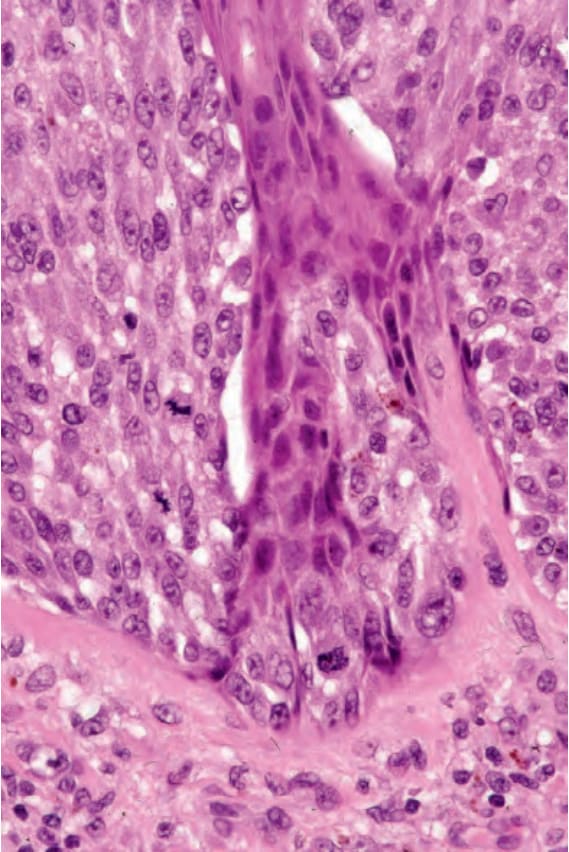
Fig. 25.160 Spindle cell tumor of Reed: note the mitotic figures.

Fig. 25.161 Deep penetrating nevus: the nevus is intensely pigmented and sharply circumscribed. By courtesy of the Institute of Dermatology, London, UK.
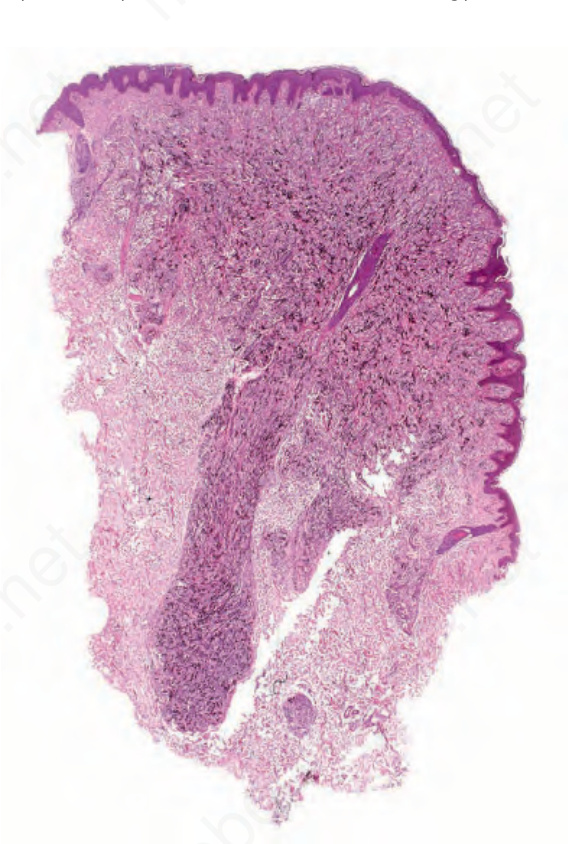
Fig. 25.162 Deep penetrating nevus: the nevus is wedge shaped with the broad base uppermost and a deeply penetrating lower border.
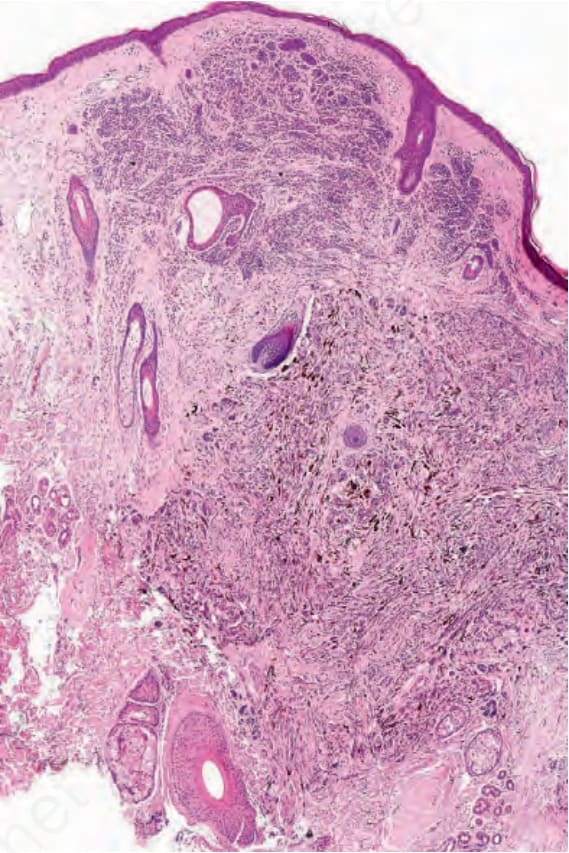
Fig. 25.163 Deep penetrating nevus: this example is a combined variant with a banal dermal component overlying the deep penetrating nevus.
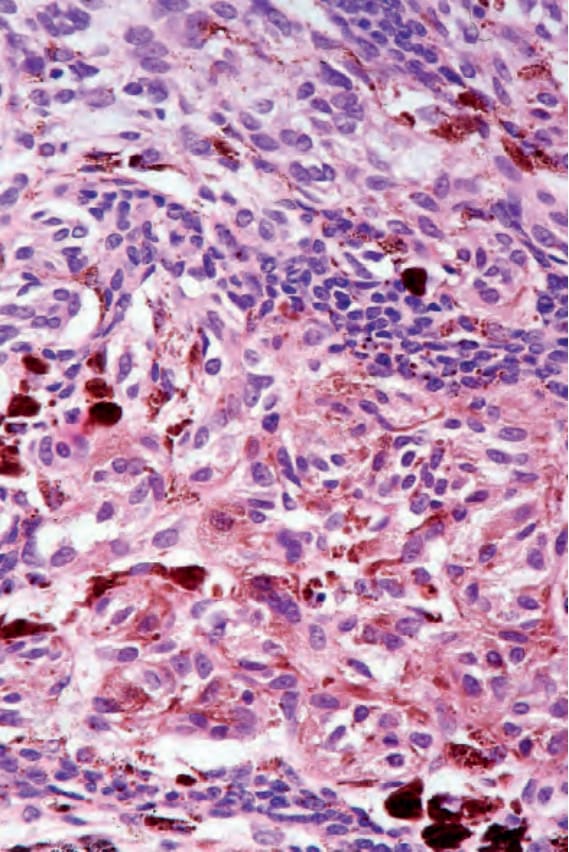
Fig. 25.164 Deep penetrating nevus: high-power view of Fig. 25.163.
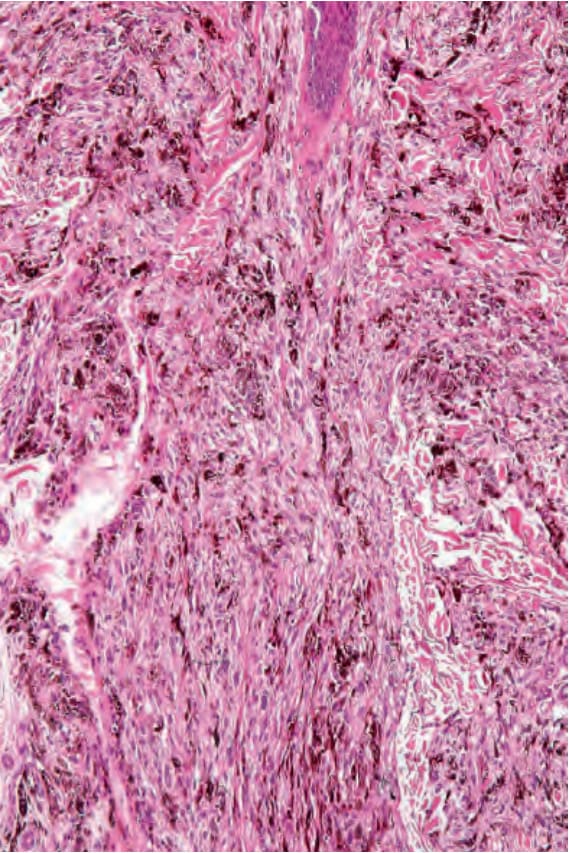
Fig. 25.165 Deep penetrating nevus: the deep extension typically follows the hair follicles and neurovascular bundles.
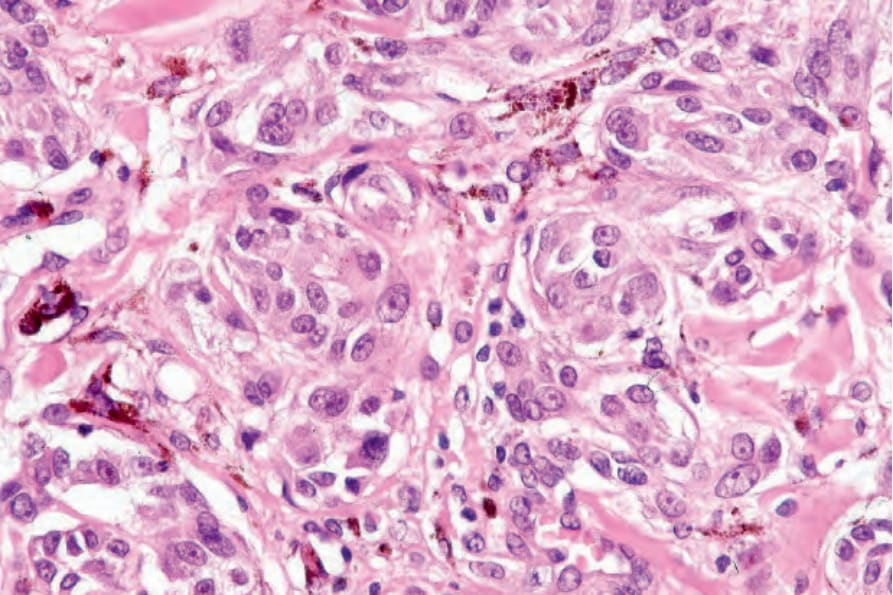
Fig. 25.166 Deep penetrating nevus: superficially, the nevus consists of epithelioid melanocytes with pale-staining or finely pigmented cytoplasm and vesicular nuclei, often with small eosinophilic nucleoli.
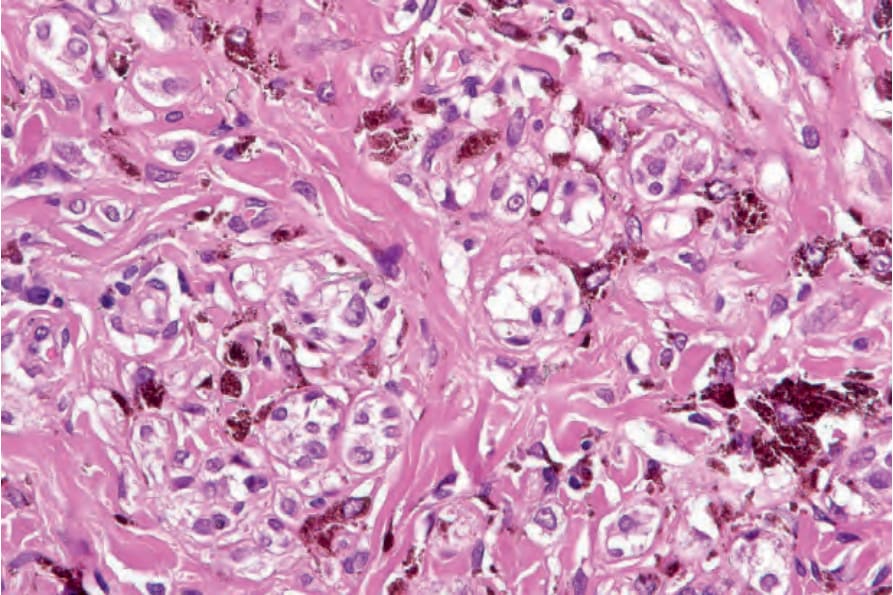
Fig. 25.167 Deep penetrating nevus: clear cells are commonly present.
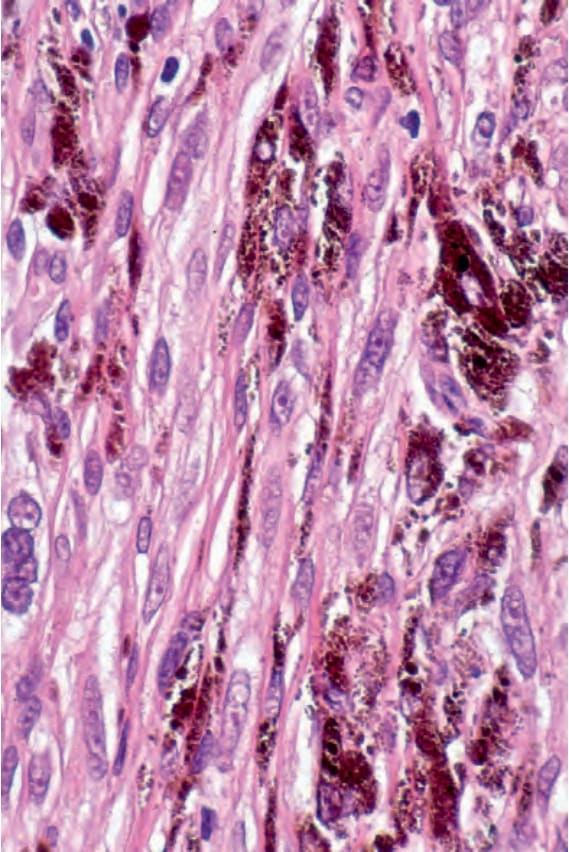
Fig. 25.168 Deep penetrating nevus: in the deeper reaches, spindled cell forms predominate and heavily pigmented melanophages are often conspicuous.
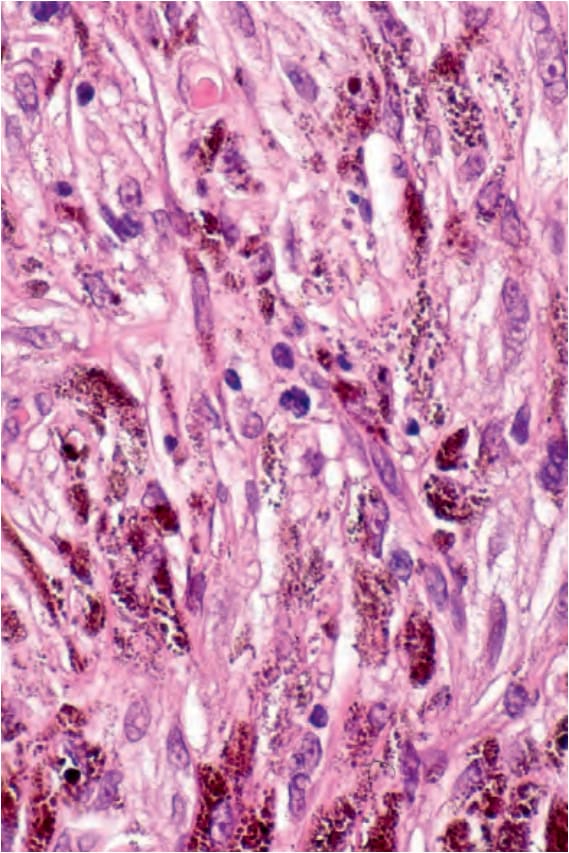
Fig. 25.169 Deep penetrating nevus: very occasional mitoses may be found but they are never numerous or abnormal.
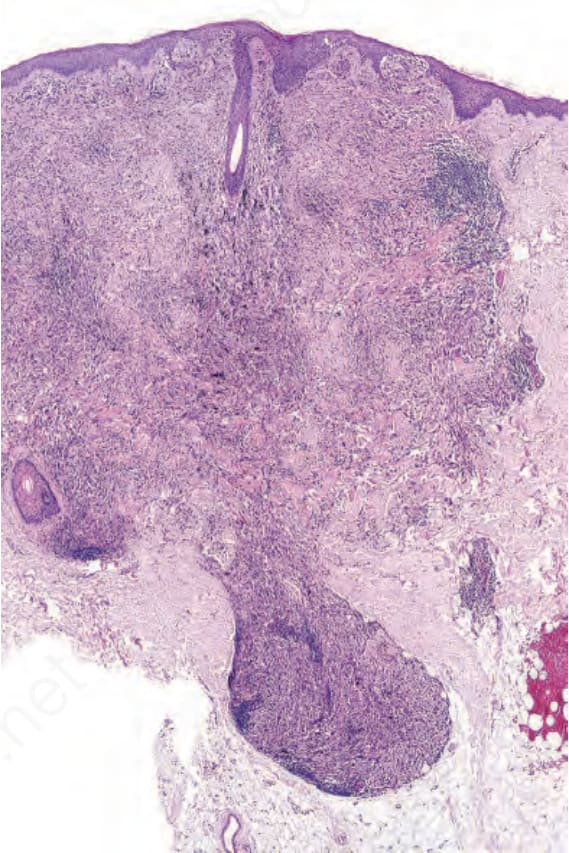
Fig. 25.170 Melanoma with deep penetrating growth pattern: at low-power magnification, this lesion shows a deep penetrating growth pattern.
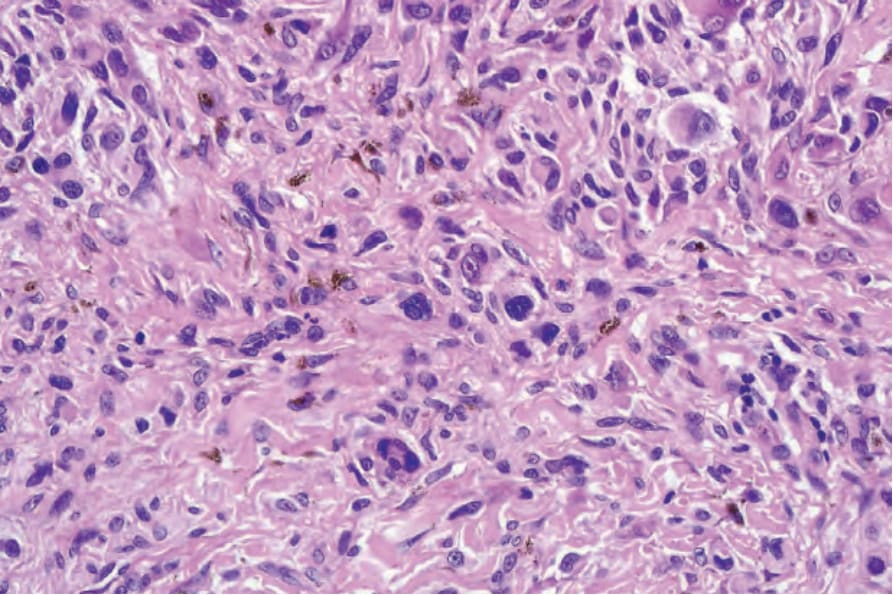
Fig. 25.171 Melanoma with deep penetrating growth pattern: at high-power magnification, however, there is marked nuclear pleomorphism and hyperchromatism.