Halo nevus
Halo nevus
Clinical features Halo nevus (Sutton nevus, leukoderma acquisitum centrifugum) presents clinically as a pigmented melanocytic nevus surrounded by a hypopigmented
border and is usually associated with regression.1,2 Rarely, development of a halo phenomenon in a melanocytic nevus can be predated, especially in children, by a preceding elevated or verrucous and crusted surface.3 Occasionally, a halo may be seen around a congenital melanocytic nevus, blue nevus, Spitz nevus, dysplastic nevus, or even melanoma.4–8
Typically, halo nevus presents as a small pigmented macule surrounded by a narrow border of hypopigmentation (Figs 25.98–25.100). The incidence is equal in men and women. It arises most frequently in the second decade, usually on the trunk, particularly the back. The developing of a melanocytic lesion with a halo in an old adult should be viewed with suspicion. Halo nevi are sometimes multiple and occasionally exhibit a familial tendency; there is an increased incidence of associated intralesional and extralesional vitiligo.5,9–12 Halo nevi are up to 10 times more frequent in patients with
1260 Melanocytic nevi
circulating antibodies to cytoplasmic antigen(s) in melanoma cells. These antibodies disappear after excision or spontaneous resolution of the central lesion.18 Patients with Turner syndrome have an increased prevalence of halo nevi compared with the general population (18% vs. 1%).19 An association of multiple halo nevi with carcinoid tumor of the ileum has been described.20 Mycosis fungoides superimposed on a melanocytic nevus can present clinically with a halo phenomenon.21
vitiligo than in the general population.13 In addition, children with halo nevi and vitiligo are more likely to develop generalized than segmental or focal vitiligo.13 Development of multiple halo nevi has also been reported following treatment with infliximab, imatinib, and interferon beta-1a.14–16 Furthermore, a short period of sunbathing has also been associated with the development of multiple halo nevi.17 Patients with halo nevi very often have
The natural history of halo nevi is usually associated with persistence for years, often even more than a decade, frequently without complete regression.22
Histologic features The lesion consists of a raised dermal nodule associated with an acanthotic and frequently hyperkeratotic epidermis (Fig. 25.101). The nevus is usually compound and infiltrated extensively by lymphocytes and histiocytes with occasional mast and plasma cells (Figs 25.102 and 25.103). The lymphocytes are predominantly of suppressor/cytotoxic T-cell phenotype, admixed with a minor population of CD4-positive T-helper cells, B lymphocytes, macrophages, and Langerhans cells.23–25 Epithelioid granulomata can occasionally be found within the inflammatory cell infiltrate.26 With progressive apoptosis, the nevus cells may become increasingly more difficult to identify, and their numbers are replaced by pigment-containing macrophages.
1261 Halo nevus
Degenerative cytological atypia may be seen. Mitotic activity is not a feature. However, inflammatory cells are often mitotic, and this is often a challenge. An accurate evaluation of the proliferation rate in the melanocytes population is aided by immunohistochemistry for Ki-67 counterstained with a melanocytes marker such as Melan-A using two different colors. Maturation is very difficult to evaluate during the evolution of the lesion, particularly in late stages due to the prominent inflammation. Residual nevus cells may be highlighted with immunohistochemistry using a melanocytic marker like S100 protein (Fig. 25.104). Since the latter often stains variable numbers of reactive dendritic cells, a marker such as MART-1/Melan-A may be used, remembering that the latter may sometimes label macrophages. It is at the late stages that the lesion may be histologically mistaken for melanoma. In the center of the lesion, blood vessels may sometimes be conspicuous. Rarely, halo nevi may develop in the absence of an inflammatory cell
infiltrate.27 Some lesions display identical histologic features to those seen in halo nevi, but a halo is not noticed clinically. Such lesions are described as showing a halo phenomenon.
The depigmented halo shows a complete absence of melanin pigment accompanied by a negative dopa reaction. Often, complete absence of melanocytes is also seen. The epidermis, however, contains increased numbers of Langerhans cells.
1262 Melanocytic nevi
The resolved nevus is characterized by epidermal hypopigmentation accompanied by scattered dermal melanophages. Mild scarring may sometimes be evident.
Differential diagnosis The halo nevus must be distinguished from melanoma. Typically, mitotic activity and nuclear and cytoplasmic pleomorphism (except the degenerative changes mentioned before) are not features, except in those that represent regressing melanoma or dysplastic nevi. Evaluation of mitotic activity in the melanocytes of halo nevi is often difficult because inflammatory cells are mitotically active. Double staining with Ki-67 and a melanocytic marker such as Melan-A is useful in identifying the proliferating population of cells. Also, the cellular infiltrate accompanying melanoma is usually more monomorphic and often hugs the base of the tumor rather than actively infiltrating it, except in those undergoing regression.

Fig. 25.100 Halo nevus: this is an ‘end-stage’ lesion in which the central nevus has largely disappeared. By courtesy of the Institute of Dermatology, London, UK.
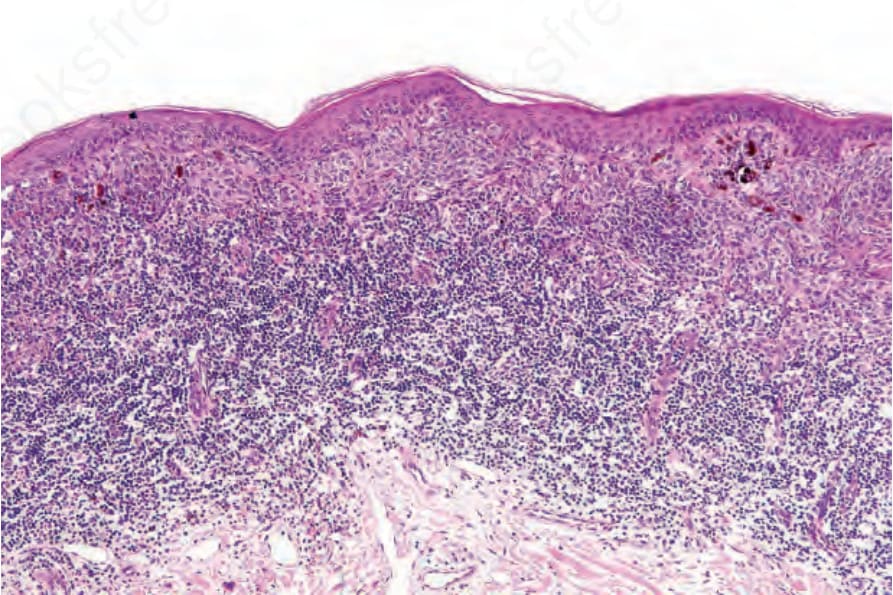
Fig. 25.101 Halo nevus: there are residual junctional nests deep to which is a dense, bandlike lymphohistiocytic infiltrate.
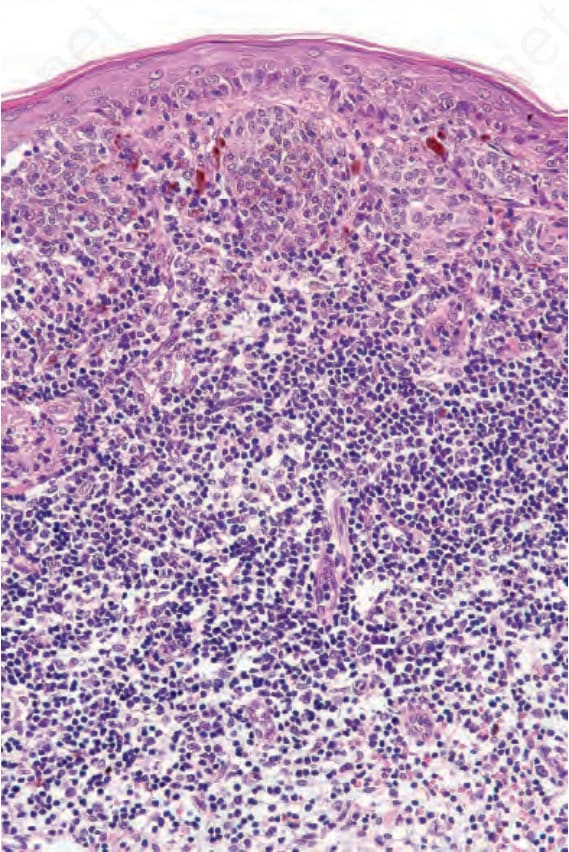
Fig. 25.102 Halo nevus: higher-power view of Fig. 25.101.
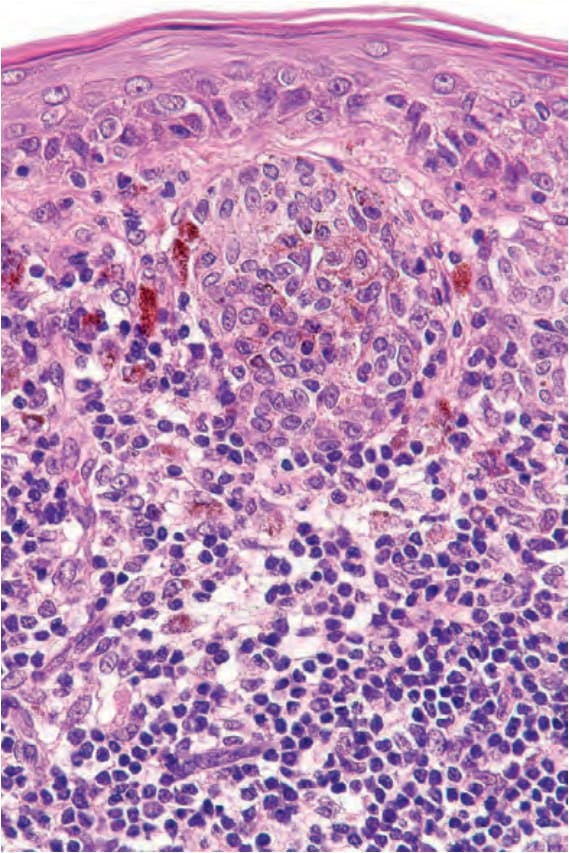
Fig. 25.103 Halo nevus: close-up view. Note the pigment incontinence.
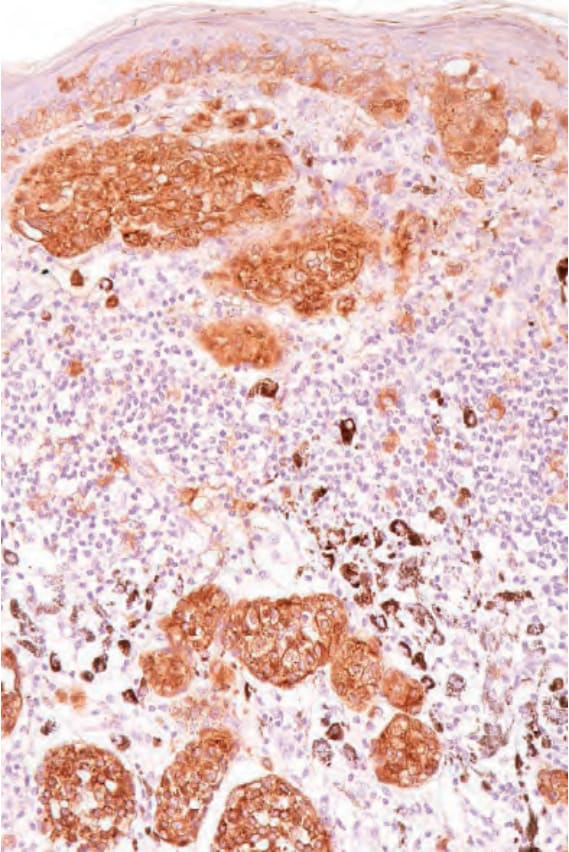
Fig. 25.104 Halo nevus: S100 protein immunohistochemistry highlights the residual nests in the dermis.
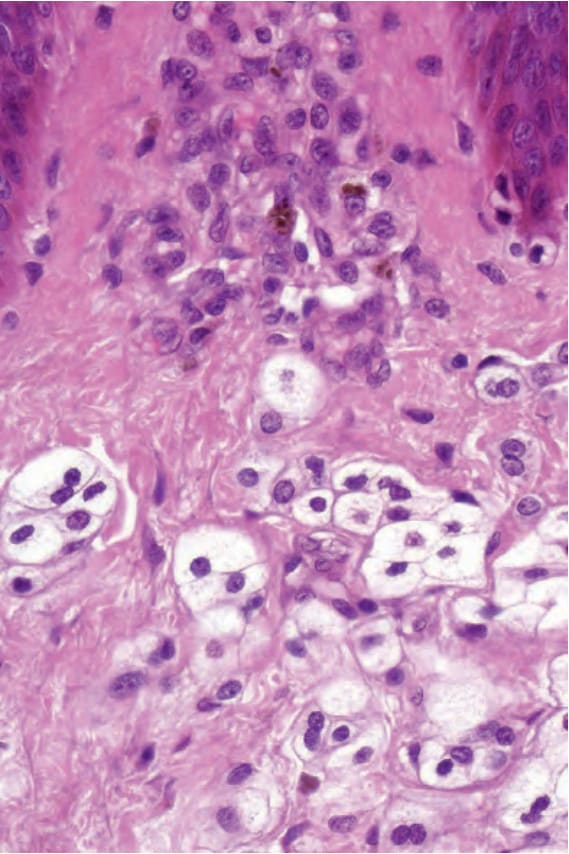
Fig. 25.97 Balloon cell nevus: diagnosis is facilitated by the identification of more typical nevus cells.
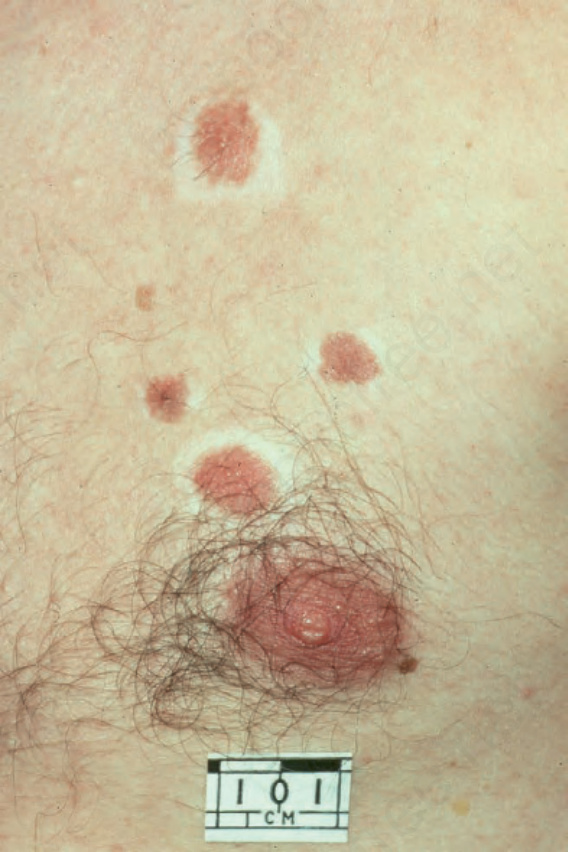
Fig. 25.98 Halo nevus: these nevi are surrounded by typical haloes. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 25.99 Halo nevus: close-up view showing a heavily pigmented central nodule with a pale-staining halo. By courtesy of the Institute of Dermatology, London, UK.