Nevi on the scalp
Nevi on the scalp
Clinical features Nevi on the scalp occur most frequently on the occipital region, followed by left parietal region, right parietal region, and frontal region (Fig. 25.65).1
1251 Melanocytic nevi at special sites
Their number is related to the number of total body nevi and are most common in the fourth decade of life (mean age, 35 years).1 Nevi on the scalp show male predominance.
About 10% of nevi on the scalp show disturbing histologic features.2 Such nevi are usually seen in adolescents and young adults.2,3 They have histologic features similar to those found on lesions in the mammary line, genital area, and flexural sites.
Histologic features Two main morphological patterns of atypical melanocytic nevi can usually be appreciated at this site: a large nested pattern and a pattern mimicking a dysplastic nevus.2,3 In general, atypical nevi on the scalp are characterized by asymmetry and poor lateral circumscription (Figs 25.66–25.70).2 The nested pattern of proliferation consists of large nests of melanocytes located at the tips and sides of rete ridges and randomly scattered along the dermal– epidermal junction. In addition, melanocytic nests show variation in shape, with frequent bizarre forms and discohesion of tumor cells within them. Involvement of skin adnexa can be seen and may be prominent.3 Focal lentiginous proliferation along the dermal–epidermal junction is frequently present. Melanocytic atypia is usually mild (although occasionally severe
1252 Melanocytic nevi
cytological atypia is present) and random, and consists of hyperchromatic nuclei and indistinct nucleoli. Upward migration of isolated melanocytes can sometimes be seen in the central part of the lesion. The dysplastic nevus-like pattern is characterized by bridging of the rete ridges, extension of the junctional component past the dermal component, and papillary dermal fibroplasia.3 The dermal melanocytic component is usually unremarkable, although occasionally superficial mitotic activity can be seen.
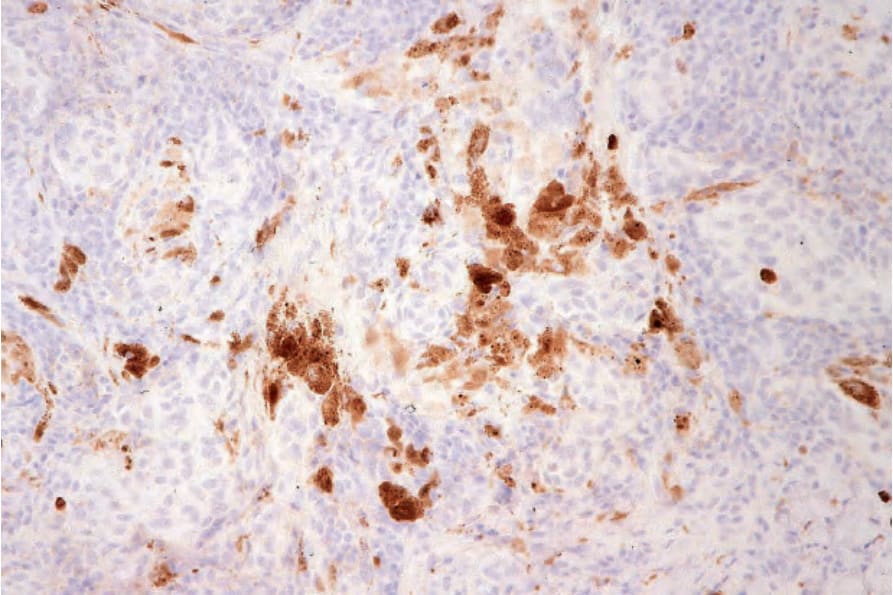
Fig. 25.64 Clonal nevus: the nevus cells do not express MIB-1. By courtesy of W. Grayson, MD, National Health Laboratory Service, Johannesburg, South Africa.

Fig. 25.65 Scalp nevus: lesions at this site may on occasions show cytological features that can raise concern for a diagnosis of melanoma by the unwary. Note the central pallor with a rim of hyperpigmentation.
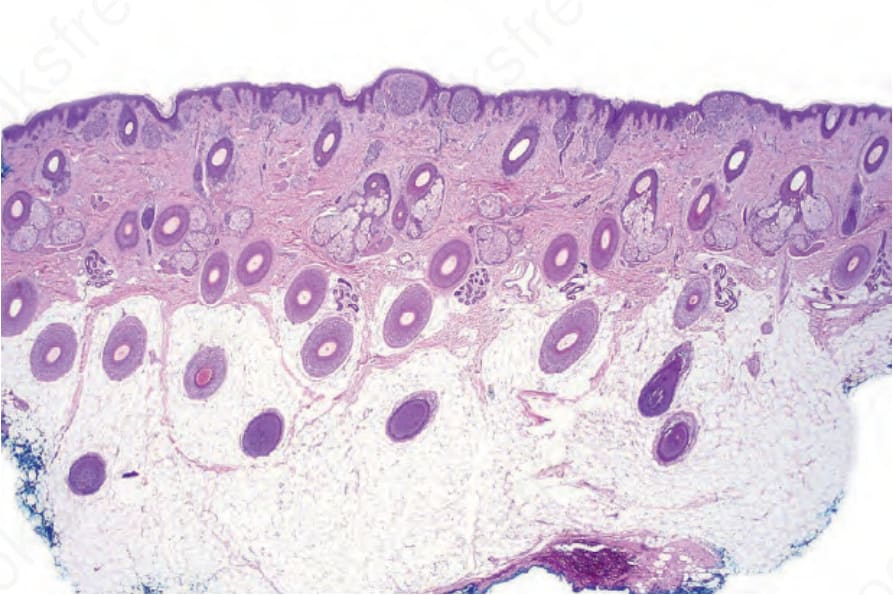
Fig. 25.66 Scalp nevus: even at low-power magnification, large expansile junctional nests can be appreciated.
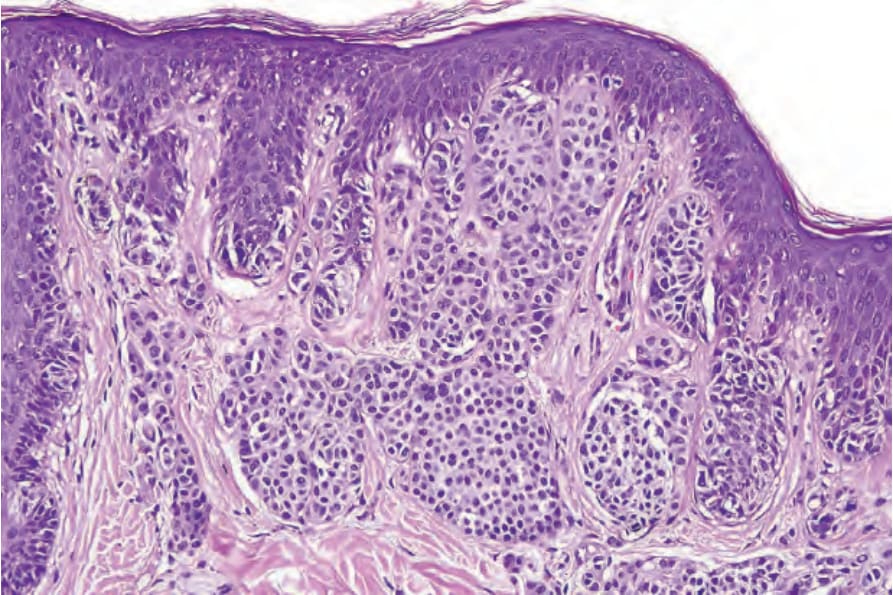
Fig. 25.67 Scalp nevus: the dermal nests are larger than the junctional ones, a feature which always results in concern.
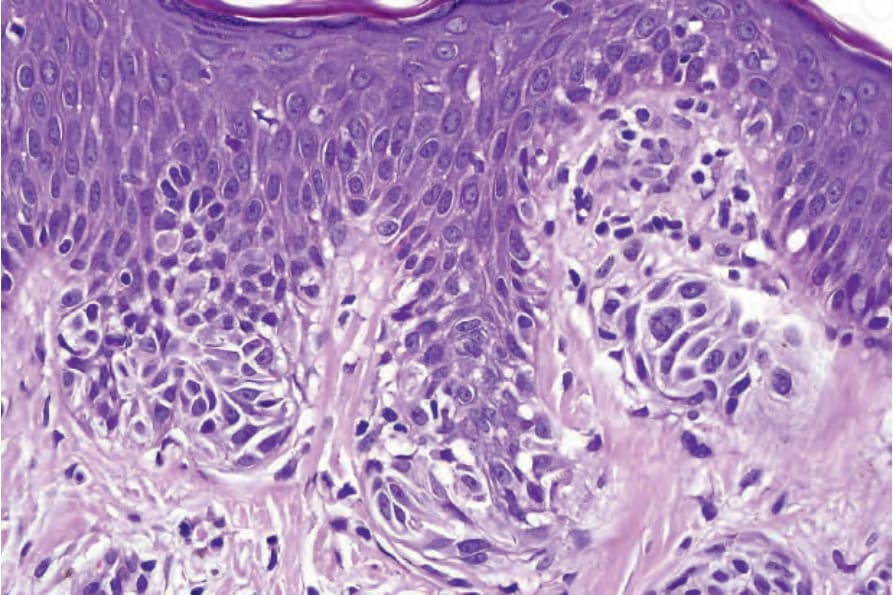
Fig. 25.68 Scalp nevus: in this field, the junctional nevus cells show moderate to severe cytological atypia.
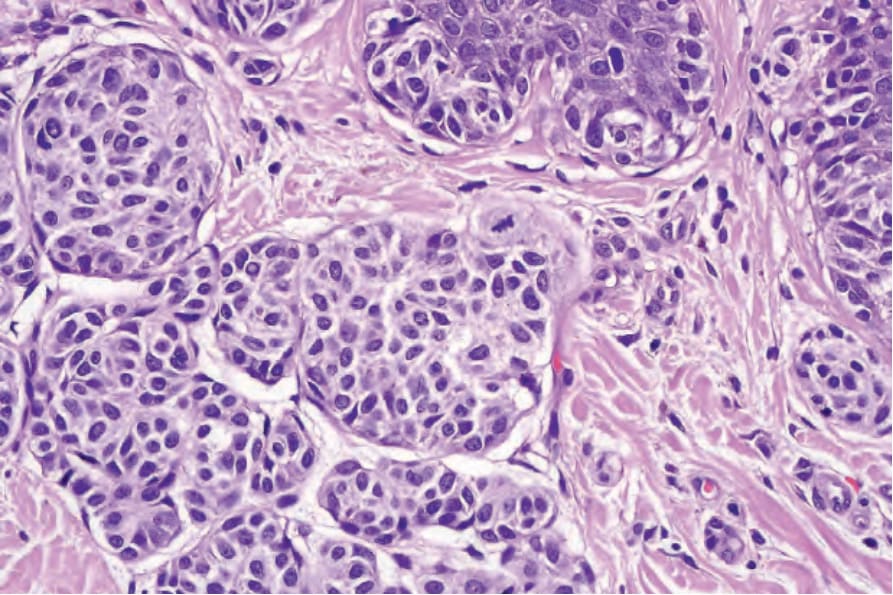
Fig. 25.69 Scalp nevus: note the mitotic figure in the superficial dermal component.
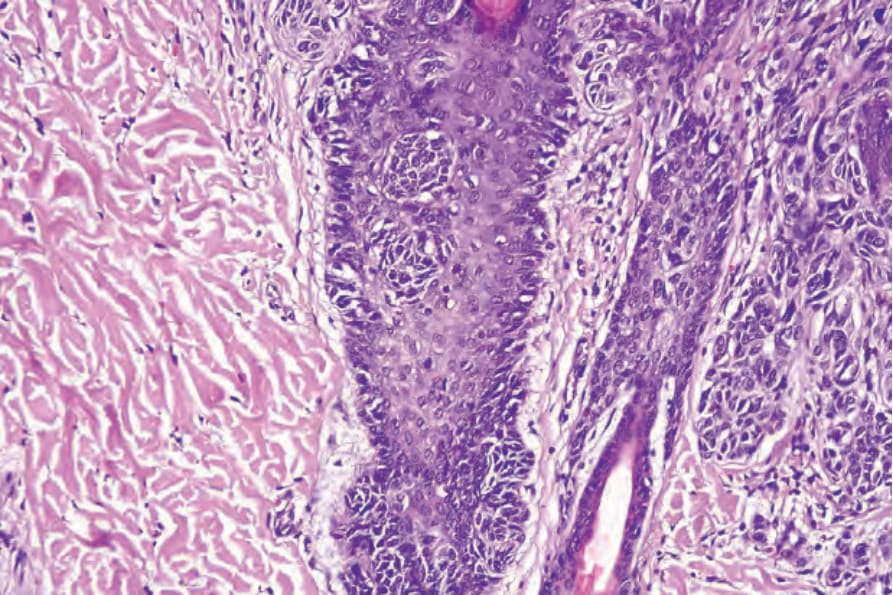
Fig. 25.70 Scalp nevus: there is follicular involvement accounting for the significant recurrence rate for these lesions.

Fig. 25.71 Nevus of ear: note the ill-defined pigmented, macular lesion.
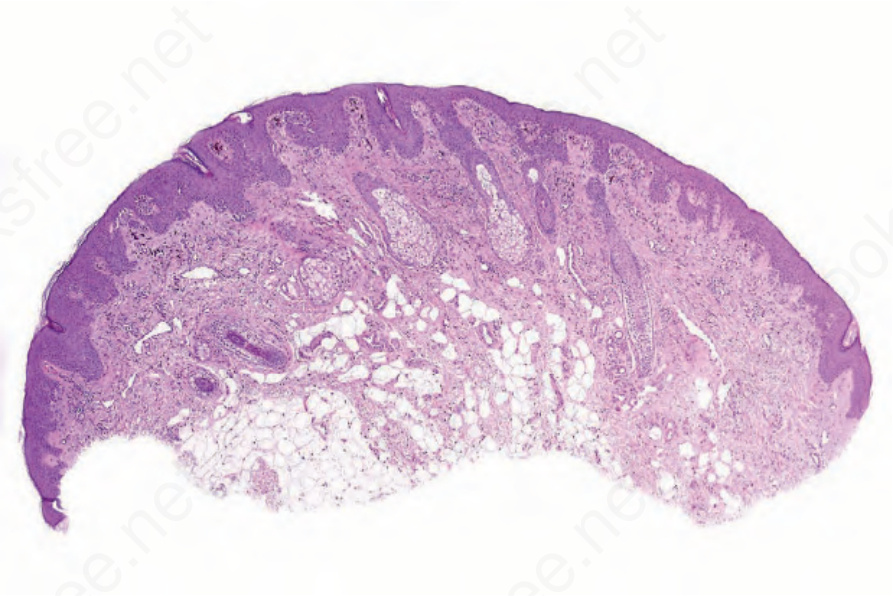
Fig. 25.72 Nevus of ear: scanning view of a largely junctional lesion.