Lentigo simplex
Lentigo simplex
Clinical features Lentigo simplex is a very common melanocytic lesion. Lesions – which are small (1–5 mm), uniformly pigmented, brown to black, sharply circumscribed macules – may be found anywhere on the integument, the conjunctivae, and mucocutaneous orifices (Fig. 25.3).1,2 They often develop in
1235 Laugier-Hunziker syndrome
childhood (juvenile lentigo) and become more conspicuous during pregnancy. Rarely, numerous lentigines may develop following an infection or an exanthem, and exceptionally they are generalized (generalized lentigines, lentigines profusa).1,3 Segmental lentigines have also been documented.4 Development of simple lentigines limited to areas treated with tacrolimus has been reported in children with atopic dermatitis.5 Simple lentigines have also been described in association with type I hereditary punctate palmoplantar keratoderma.6 Hyperpigmentation and increased numbers of lentigines are features of Addison disease. Simple lentigines have no malignant potential and, in contrast to ephelides, have no connection with sunlight.
Lentigines assume a particular importance when their presence is associated with a variety of inherited systemic conditions, including Peutz-Jeghers, LEOPARD (multiple lentigines), and Carney syndromes, centrofacial lentiginosis, and Laugier-Hunziker syndrome (idiopathic lenticular mucocutaneous pigmentation). The last is characterized by oral melanotic macules and longitudinal pigmentation of the nails (Figs 25.4 and 25.5). An association between somatic mutation in keratin 10 (KRT10) gene and development of numerous simple lentigos, linear epidermolytic nevus, and epidermolytic nevus comedonicus has also been reported.7
Histologic features The histologic features are those of slight to moderate elongation of the epidermal ridges associated with an increased number of basally located melanocytes (Figs 25.6 and 25.7).1,2 Generally, no atypia of melanocytes is seen. There is no junctional activity and pigmentation is increased, both within the epidermis and within melanophages in the papillary dermis. Rarely, giant melanosomes (macromelanosomes) may be identified (Fig. 25.8). A superficial dermal lymphohistiocytic infiltrate is often present. Not uncommonly, lentigo and junctional nevus may coexist – lentiginous junctional nevus (Fig. 25.9).
Interestingly, a recent study failed to demonstrate the presence of BRAFV600E mutations in simple lentigo.8 However, BRAFV600E mutations have been demonstrated in 17% of lentiginous/junctional nevi, in 55% of compound nevi, and in 78% of intradermal nevi.8
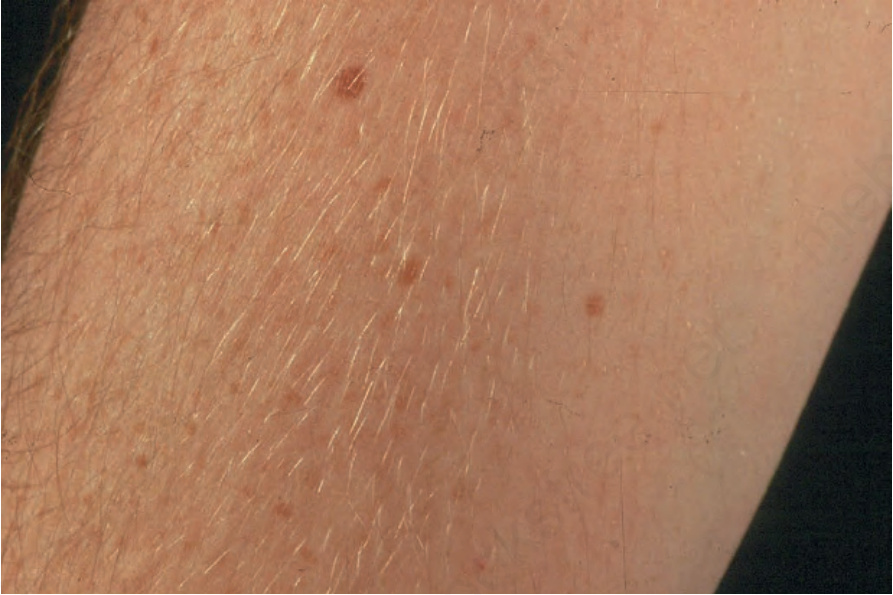
Fig. 25.1 Ephelides: these present as small pigmented macules that darken on exposure to sunlight.
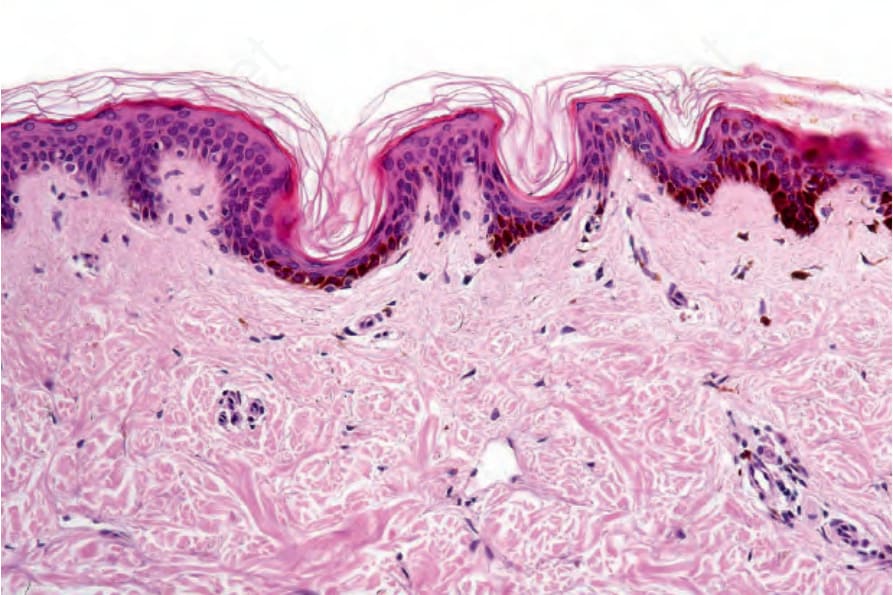
Fig. 25.2 Ephelis: note the hyperpigmentation of the basal layer of the epidermis. The number of melanocytes is within normal limits and there is no evidence of junctional activity.

Fig. 25.3 Lentigo simplex: this is a small, uniformly pigmented macule clinically indistinguishable from an ephelide. It is unrelated to sun exposure.
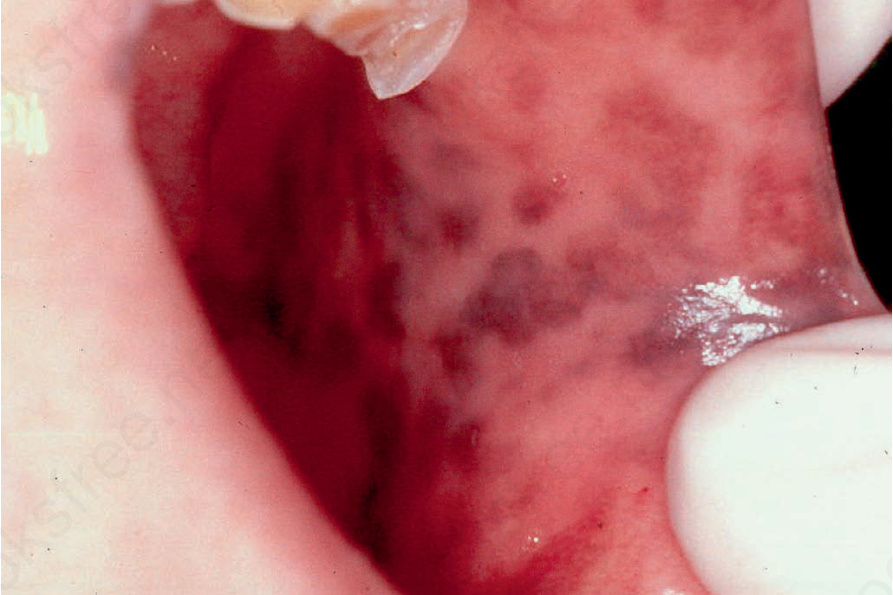
Fig. 25.4 Laugier-Hunziker syndrome: oral melanotic macules. By courtesy of S.-B. Woo, MD, Harvard Medical School, Boston, USA.
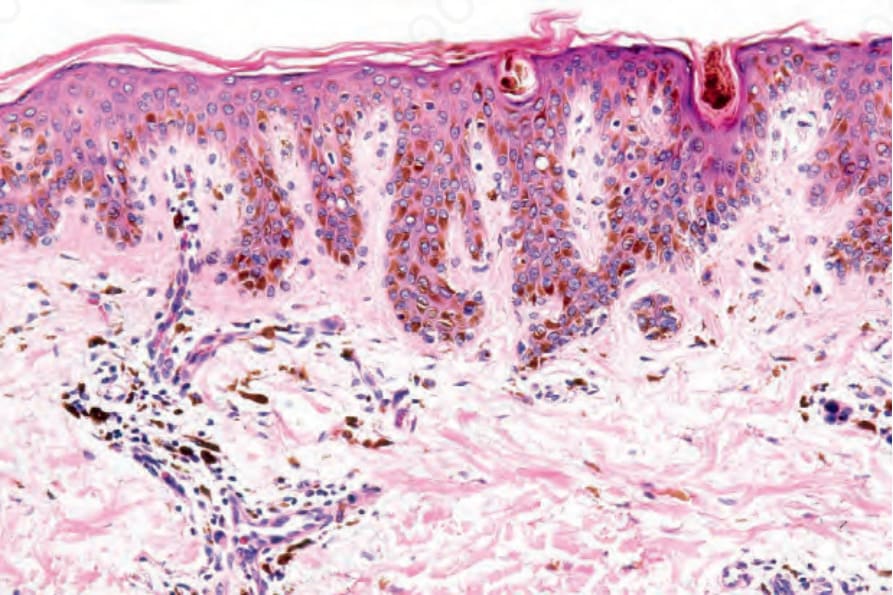
Fig. 25.6 Lentigo simplex: there is acanthosis with elongation of the epidermal ridges. Basally located melanocytes are increased in number. There is excessive pigmentation of the epidermis, but no junctional activity is present.
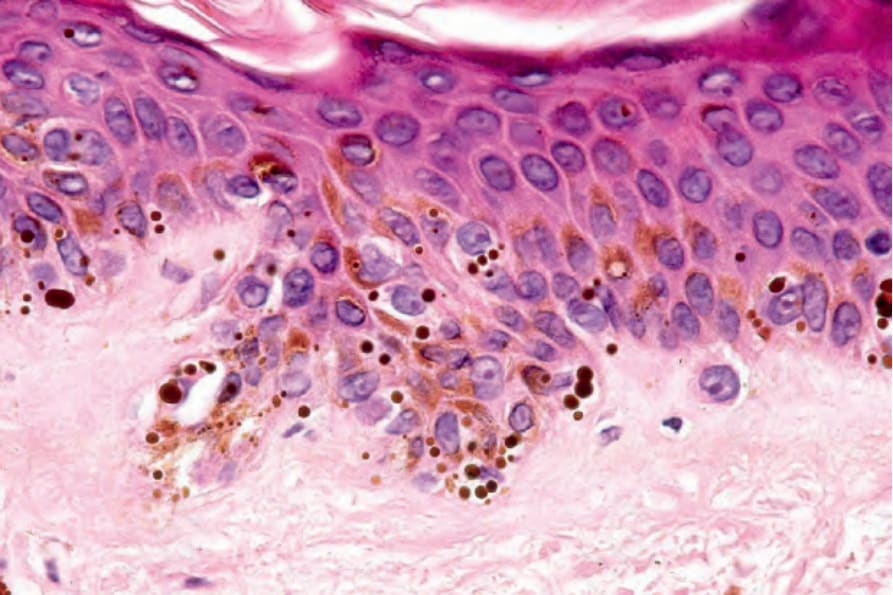
Fig. 25.8 Lentigo simplex: note the presence of macromelanosomes.
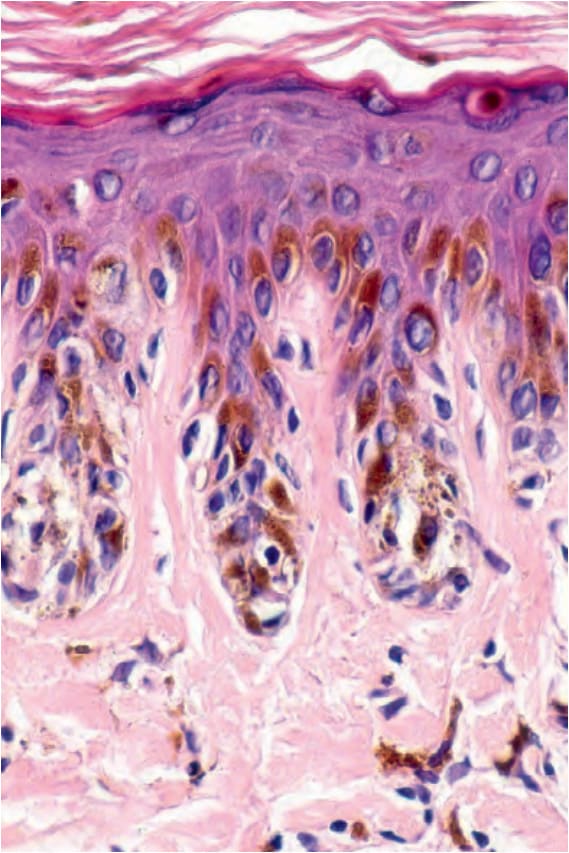
Fig. 25.9 Lentiginous junctional nevus: the rete ridges are elongated, and increased numbers of melanocytes are present as nests at the tips of the rete ridges and single cells distributed along the sides.