Keratoacanthoma
Keratoacanthoma
B
Keratoacanthoma (molluscum sebaceum) is a rapidly growing skin tumor arising predominantly on the exposed surfaces of the body.1–3 Although believed to be of follicular infundibular derivation and, therefore, not strictly speaking a tumor of the epidermis, it is included in this section because of its histologic similarities to squamous cell carcinoma.4,5
Few entities in dermatology have been responsible for as much controversy as keratoacanthoma.6 It has been variously described as a benign tumor, a pseudomalignancy, a regressing malignancy, and as a variant of squamous cell carcinoma.7–9 Cited examples have documented persistent10 and recurrent tumors, perineural infiltration, vascular involvement, and metastatic spread.8,11–16 Despite the presence of perineural infiltration these lesions are said not to show metastatic spread or recurrence.15 In contrast, however, there are cases that apparently fulfill both the clinical features and ‘diagnostic histologic criteria’ of keratoacanthoma and yet behave in a malignant fashion.17–19 Although regarded by many as a variant of squamous cells carcinoma, this view is controversial and not universally accepted.
more often in males than in females (2–3 : 1) and increases in incidence with age, most patients being in their sixth or seventh decade.20,42 Presentation in children is rare.43 Although it is not uncommon in colder, temperate climates, the incidence increases dramatically with diminishing latitude.42 Typical squamous cell carcinoma occurs at least three times more often than keratoacanthoma.20,44
Clinically, solitary keratoacanthoma presents as a smooth, hemispherical papule that rapidly enlarges over the course of a few weeks to produce a 1- to 2-cm diameter, discrete, round or oval, often flesh-colored umbilicated nodule with a central keratin-filled crater (Figs 24.178 and 24.179).20 Pigmentation is exceedingly rare.45 Lesions larger than 3 cm in diameter are sometimes known as giant keratoacanthoma (Fig. 24.180).46–50 Occasionally, multiple lesions are present.43,51–55 Usually, involution then occurs with tumor resorption and loss of the keratin plug, to leave a depressed, hypopigmented scar.7 The lifespan of a typical keratoacanthoma is 4–6 months. Recurrence following surgical intervention may occur in up to 8% of patients.3
Clinical features A variety of subtypes have been recognized.7,20,21 Most common is the solitary keratoacanthoma. This is predominantly a tumor of the white-skinned races, Asians and Afro-Caribbeans rarely being affected.22 Usually it appears to be related to excessive exposure to UVB and therefore lesions are most commonly found on sun-damaged skin, particularly of the face (Fig. 24.177), forearms, wrists, and backs of the hands.20,23–25 Conjunctival lesions have also been very rarely described, predominantly in middle-aged males.26–30 Other infrequently affected sites include the tongue, penis, vulva, oral mucosa, lip, sole, perianal skin, and anal canal.26,31–40 The lesions may be multiple.27,41 Intersex variation is evident: lesions on the calves are not uncommon in females but are rare in males, while the dorsum of the hand is a common site in males but not in females.3 Keratoacanthoma is diagnosed
Agglomerate keratoacanthoma consists of several lesions coalescing to form a single large plaque, which may persist for up to 6 months and then undergo regression.20
Keratoacanthoma centrifugum marginatum (multinodular keratoacanthoma) is extremely rare and is characterized by marked peripheral expansion; lesions up to 20 cm in diameter have been recorded.55–64 The central area heals as the tumor expands, but often resolution takes longer (6–12
1219 Variants of squamous cell carcinoma
months) than that of the more conventional variant. Multiple lesions may rarely be encountered.55,58–60,65 Some examples have persisted for many years, shown no tendency for spontaneous resolution, and have been associated with considerable tissue destruction.56 It would be particularly appropriate to regard these latter as low-grade squamous cell carcinomas.
A peculiar rare tumor known as subungual keratoacanthoma has also been delineated.66–77 Although histologically similar to the cutaneous type, its apparent derivation from the nail matrix rather than the follicular infundibulum suggests a different histogenesis, and it appears to behave in a more destructive fashion than ordinary keratoacanthoma.71–73 Lesions predominantly affect the thumb and forefinger and present with pain, swelling, and erythema67 and may mimic chronic paronychia.78 Radiological studies reveal a characteristic cup-shaped area of osteolysis with absent periosteal reaction or reactive new bone formation. The tumor appears to respond well to curettage, the recurrence rate being only 14%.69 These lesions are identical to the subungual tumors of incontinentia pigmenti.79,80 An association with steel wool has been postulated81 and a familial case has been reported to occur in association with ectodermal dysplasia.82
Keratoacanthoma may rarely develop within a pre-existent nevus sebaceous or represent a manifestation of the Muir-Torre syndrome.83–86
A variety of extremely rare syndromes have been described in which patients present with large numbers of keratoacanthomas:
• Familial primary self-healing squamous epitheliomata of the skin (Fergusson-Smith syndrome) has been documented, largely in a Scottish kindred, and is a rare, but distinct, clinical entity with an autosomal dominant mode of inheritance.87 It is three times more common in males than in females.20 Patients, usually in childhood or early adulthood, develop multiple (sometimes hundreds) recurrent tumors (Fig. 24.181). Although sun-exposed skin is predominantly affected, lesions may also be found on the external genitalia and scalp and are sometimes trauma induced.20,88 The lesions are much slower to resolve and may be associated with greater tissue damage and scarring than with the more commonly encountered variant.
• In eruptive keratoacanthoma (Grzybowski syndrome), patients develop enormous numbers (hundreds to thousands) of follicular papules 1–5 mm in diameter.89–102 The sex incidence is equal.20 The lesions, which are often pruritic and sometimes painful, often present on sun-exposed skin, but may become generalized. Ectropion is a distressing complication. Koebnerization is occasionally evident.
1220 Tumors of the surface epithelium
Similar keratotic squamoproliferative lesions may develop in the mouth, pharynx, and larynx.89 Long-term follow up of patients with this variant has not disclosed any evidence of metastatic potential.90,91 Eruptive lesions may also develop in the immunosuppressed.103 Associations of eruptive keratoacanthomas have also been noted with pembrolizumab, laser resurfacing, skin grafting, photodynamic therapy, leflunomide, tattoos, ruxolitinib, quizartinib, imiquimod, and sorafenib.104–113 These lesions however, are not related to eruptive keratoacanthomas of Grzybowski type.
• A mixed syndrome (Witten and Zak syndrome) combining the features of the above two variants has also been documented.56,114,115
There is no evidence that solitary keratoacanthoma is associated with an increased incidence of internal malignancy.3
Pathogenesis and histologic features Keratoacanthoma may be induced in a variety of experimental animals by painting the skin with coal tar derivatives.116 Although now rare, a human counterpart has been described in people who had prolonged contact with pitch and tar.1 More recently, keratoacanthoma has occasionally been described in patients receiving coal tar preparations to treat psoriasis.
Keratoacanthomas have been shown to be clonal and numerous chromosomal abnormalities have since been identified including trisomy 7, gains of 1p, 8q, 9q and deletions of 3p, 9p, 19p, 19q, and a translocation involving chromosomes 2 and 8.117–120 RAS mutations (HRAS and NRAS) have been noted.121 Microsatellite instability has been observed in some lesions.86,122,123 Most tumors, however, appear to have a UVB-mediated pathogenesis.23,26 The great majority arise on sun-exposed skin and signs of actinic damage are usually evident. There is an increased incidence in xeroderma pigmentosum and in those who are chronically immunosuppressed, particularly following renal transplantation.20,42,124,125 Concurrent UVB-induced epidermal lesions, such as actinic keratoses and basal cell and squamous cell carcinoma, are commonly present.3
While most lesions are negative,126,127 HPV DNA has been demonstrated in a small number of lesions.121,128–132 Subtypes that have been identified include HPV types 5, 9, 10, 14, 16, 19, 20, 21, 25, 37, 38, 49, and 80.133 HPV is identified more frequently in tumors from immunosuppressed rather than immunocompetent patients.133
Rarely, keratoacanthoma may develop at the site of scarring due to prior trauma, radiation or skin grafting, or in association with inflammatory dermatoses, such as lichen planus, hypertrophic lichen planus, vitiligo, discoid lupus erythematosus, atopic eczema, and psoriasis.3,134–152 It has also been reported to complicate lesions such as linear epidermal nevus, nevus sebaceous, a pigmented patch in incontinentia pigmenti, pseudoxanthoma elasticum, stasis dermatitis, and sites of treatment for, as well as within, lesions of psoriasis.153–160 Keratoacanthoma may also be associated with Dowling-Degos disease, hidradenitis suppurativa, suramin therapy, PUVA therapy, and radiotherapy.161–165
An accurate diagnosis of keratoacanthoma is totally dependent upon an adequate clinical history. In the absence of this or when only tissue fragments are available for histologic interpretation, it is most inadvisable to make this diagnosis.
The histologic diagnosis depends upon the identification of the typical crateriform architecture.25 Excisional or deep incisional biopsies across the center of the lesion are therefore required. An established tumor is symmetrical and has both exophytic and endophytic components (Figs 24.182 and 24.183). It consists of an often large central keratin plug (sometimes showing continuity with dilated follicular infundibula) accompanied by marked squamous epithelial proliferation. The epidermis on either side of the lesion is thrown up into a well-formed collarette.
Although the epithelium may occasionally appear mildly pleomorphic, typical keratoacanthoma is characterized by well-differentiated, often pale-staining, eosinophilic, glassy cytoplasm showing a striking tendency towards keratinization (Fig. 24.184). Intracytoplasmic glycogen is often abundant. Necrosis may be evident and microabscesses containing neutrophils are frequently present (Fig. 24.185). Entrapped elastic fibers, particularly when associated with marked solar elastosis, are said to be characteristic.166,167 The presence of these does not necessarily discriminate
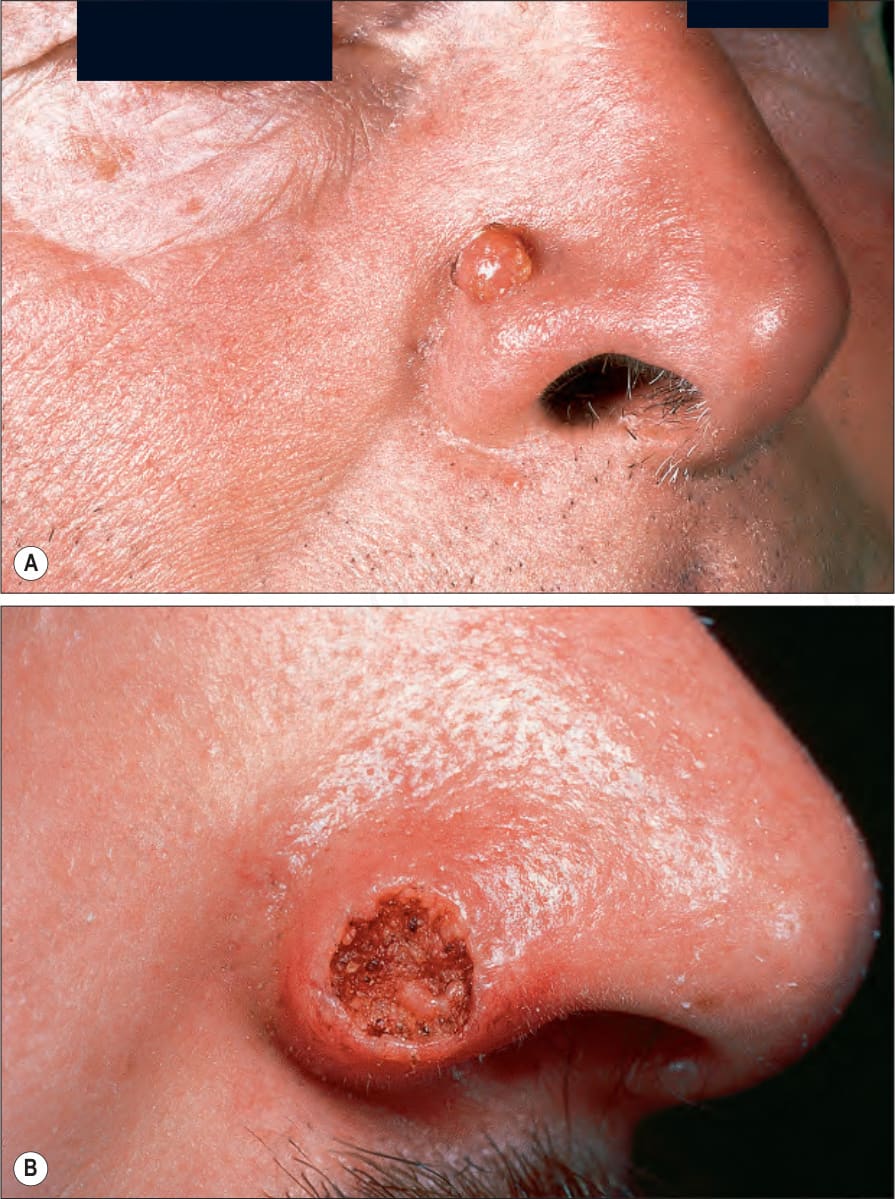
Fig. 24.177 Keratoacanthoma: (A) typical dome-shaped lesion on the nose, a commonly affected site; (B) in this example, the central crater is particularly well developed. By courtesy of the Institute of Dermatology, London, UK.

Fig. 24.178 Keratoacanthoma: close-up view of keratotic plug. By courtesy of the Institute of Dermatology, London, UK.

Fig. 24.179 Keratoacanthoma: the crater border is clearly seen in this example. By courtesy of the Institute of Dermatology, London, UK.

Fig. 24.180 Giant keratoacanthoma: massive variants, such as seen here, are associated with considerable tissue damage and scarring. By courtesy of the Institute of Dermatology, London, UK.

Fig. 24.181 Fergusson-Smith syndrome: numerous small, but otherwise typical, lesions are evident. By courtesy of the Institute of Dermatology, London, UK.
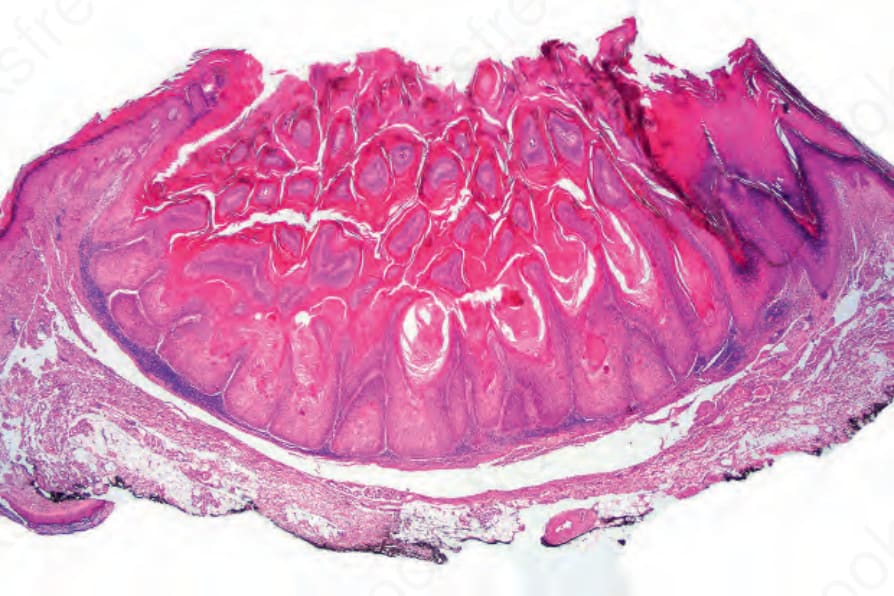
Fig. 24.182 Keratoacanthoma: scanning view of a typical keratoacanthoma showing a welldeveloped collarette.
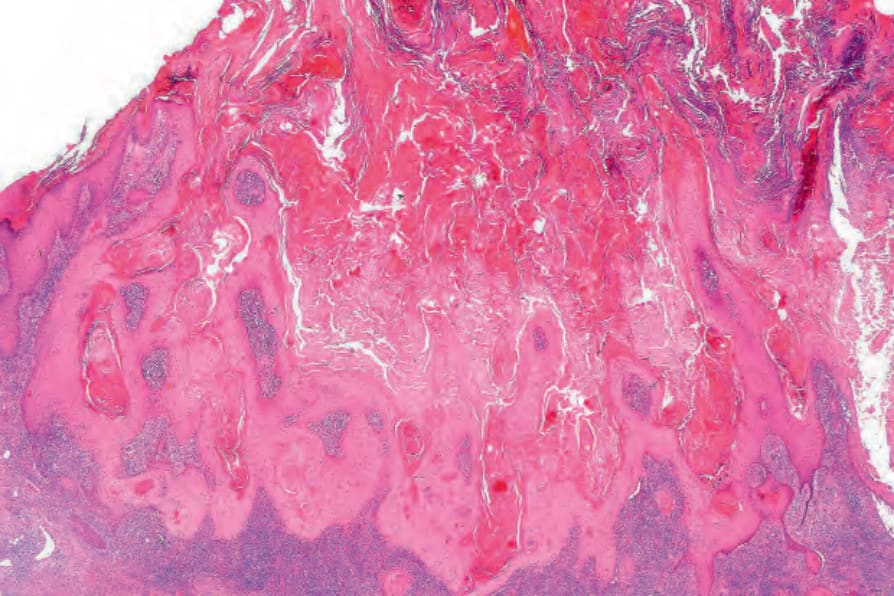
Fig. 24.183 Keratoacanthoma: this example shows the lateral collarette, keratin plug, and underlying proliferating well-differentiated squamous epithelium.
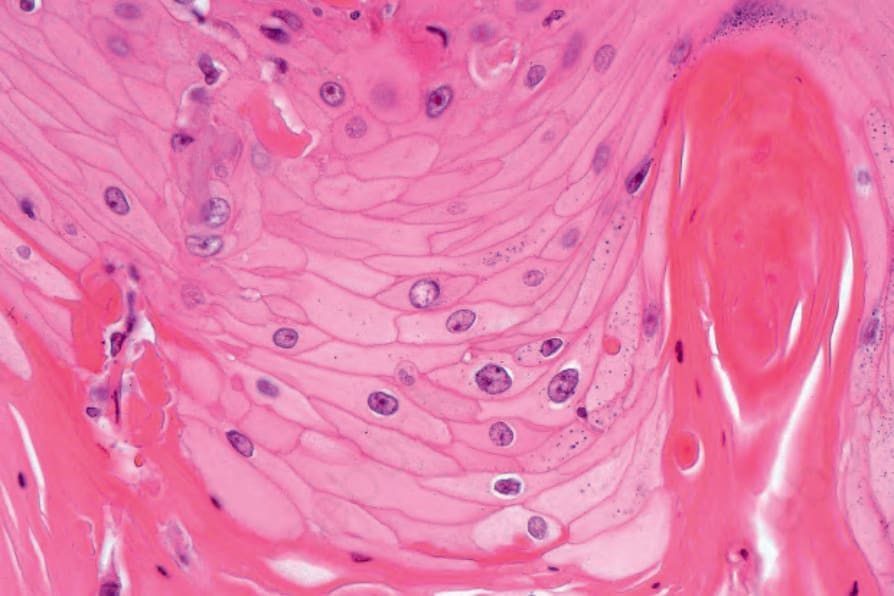
Fig. 24.184 Keratoacanthoma: the proliferating epithelium is well differentiated. The epithelial pallor is characteristic.
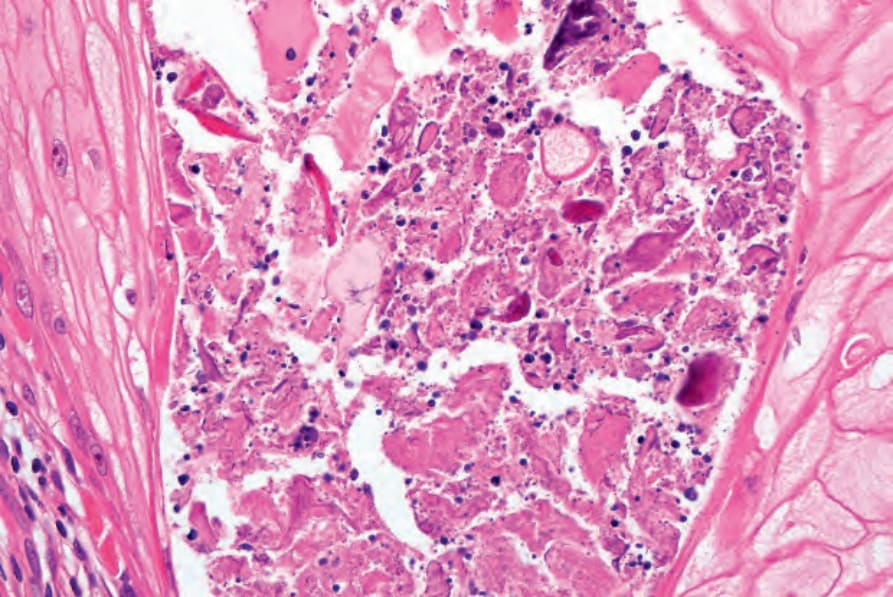
Fig. 24.185 Keratoacanthoma: intraepithelial abscesses as seen in this field are a common finding.
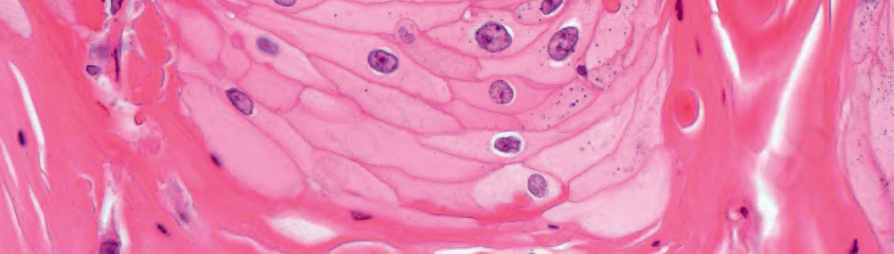
Fig. 24.186 Keratoacanthoma: mitoses are generally limited to the basal epithelial layer.
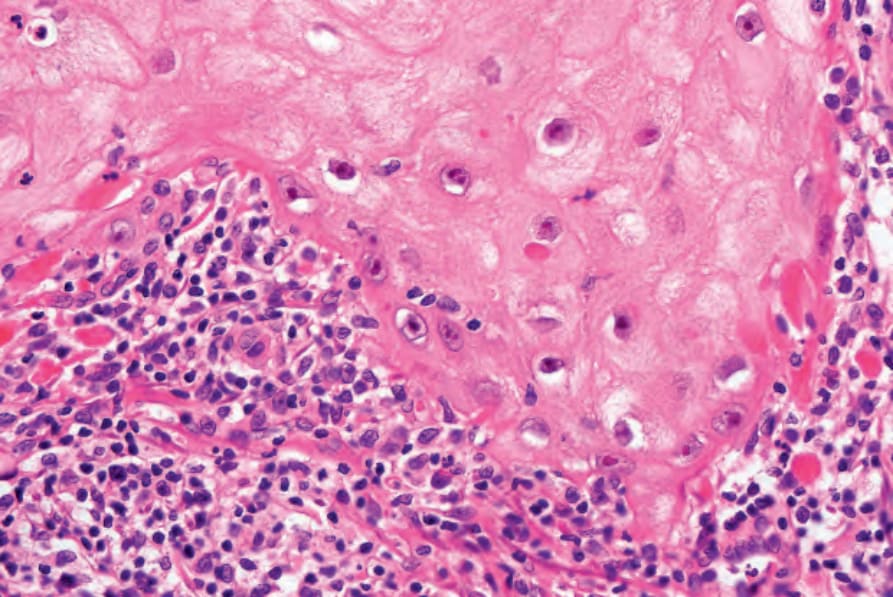
Fig. 24.187 Keratoacanthoma: the tumor is commonly associated with a mixed chronic inflammatory cell infiltrate.
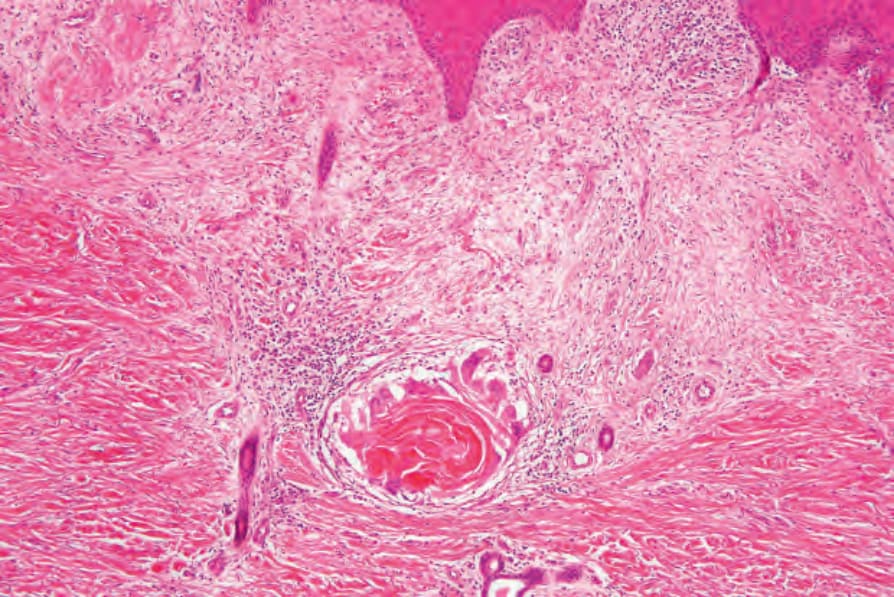
Fig. 24.189 Regressing keratoacanthoma: a prominent giant cell reaction to free keratin is often present at the base of the lesion with adjacent scarring.
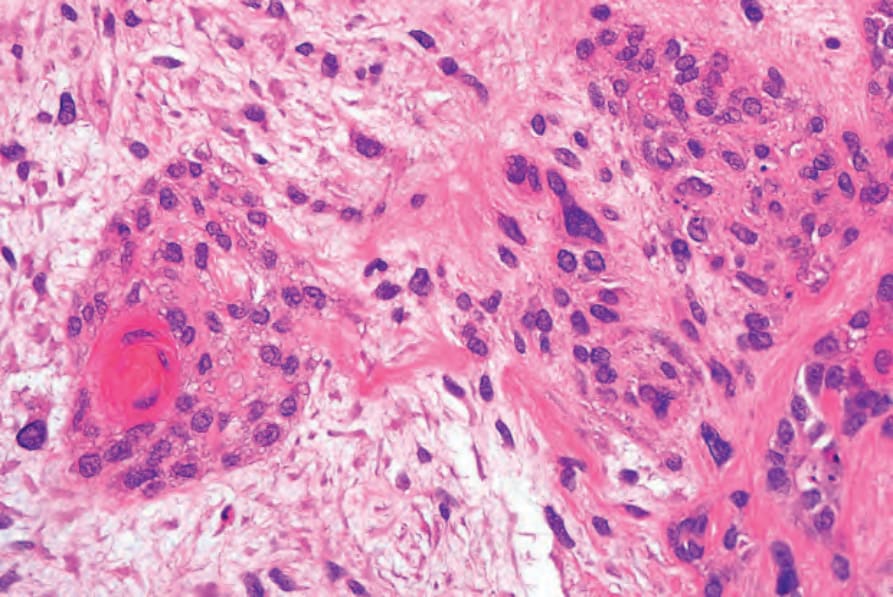
Fig. 24.192 Metaplastic squamous cell carcinoma: high-power view of squamous component.
1221 Variants of squamous cell carcinoma
Analysis of keratin and filaggrin expression points to differentiation towards the outer root sheath in keratoacanthoma.171
Unusual histologic features include atypical sweat duct hyperplasia and glandular proliferation, as well as coexistence with basal cell carcinoma and melanoma in situ.172–175
With progressive aging (and regression) of the lesion, the keratin horn is lost and the proliferating epithelium tends to flatten out, leaving a somewhat papillomatous base with underlying chronic inflammation and fibrosis (Figs 24.188 and 24.189).168 The infiltrate sometimes adopts a lichenoid distribution and is composed predominantly of cytotoxic T cells that may play a role in lesion regression (Fig. 24.190).20,169,170 At the edges a residual collarette may sometimes be evident. Not infrequently, regressing keratoacanthoma is accompanied by a foreign body giant cell reaction to released keratin. The mechanism of regression is uncertain. Although immunological factors are likely to be of significance, it has been suggested that apoptosis may be particularly important.20
Classic squamous cell carcinoma arising from typical keratoacanthomas is a rare phenomenon seen in the elderly.176
So-called subungual keratoacanthoma arises from the nail matrix and presents as a keratin-filled cystic cavity lined by abundant, well-differentiated squamous epithelium showing marked dyskeratosis.67 Mitoses are few and basally located. Because the diagnosis invariably follows surgical treatment, the biological behavior of this tumor is uncertain. Regression has not been documented. Despite some histologic overlap with verrucous carcinoma, the absence of frequent recurrences argues against this diagnosis.
Differential diagnosis There are marked similarities between keratoacanthoma and squamous cell carcinoma and occasionally it may be impossible to distinguish the two on clinical, let alone histologic, grounds though many exert great effort to do so.25,177,178
1222 Tumors of the surface epithelium
and the cytolytic receptor P2X7.179–192 Expression of TP53 and MIB-1 may also differ in subungual keratoacanthomas compared to subungual squamous cell carcinoma.193 Flow cytometric analysis of proliferation indices and S-phase fractions, however, fail to discriminate between these two lesions and studies on proteins related to tumor invasion such as matrix metalloproteinases, E-cadherin, catenins, and syndecan-1 also revealed only subtle differences in the staining pattern between keratoacanthoma and invasive squamous cell carcinoma.194–196 There is some evidence to suggest that vascular cell adhesion molecule (VCAM) and intercellular adhesion molecule (ICAM) expression may be of some value in distinguishing between keratoacanthoma and more typical well-differentiated squamous cell carcinoma.197 All of these are only relative guides and distinction requires careful observation and clinical correlation.
Usually, the clinical history and histopathological features allow a diagnosis of keratoacanthoma and predict a trouble-free outcome, but if there is any doubt about the potential biological behavior of a lesion, complete surgical excision, as for squamous cell carcinoma, is recommended.
Metaplastic carcinoma of the skin (carcinosarcoma, carcinoma with heterologous differentiation)
Clinical features Metaplastic carcinoma of the skin is an exceedingly rare malignant cutaneous neoplasm with only a few cases reported in the literature.1–13 It typically arises on sun-damaged skin as a nodular lesion ranging in size from 1 to 15 cm and often showing ulceration. The duration of these tumors ranges from several months to many years, frequently presenting with recent change. The most commonly affected sites include the face and scalp.1-7,14,15 Although it presents in a wide age range, metaplastic carcinoma is predominantly a tumor of the elderly. Clinically, there are no distinguishing features and the differential diagnosis is broad. Metaplastic carcinoma of skin has also been reported in patients with nevoid basal cell carcinoma syndrome and Brooke-Spiegler syndrome.16,17 In contrast to its counterparts in visceral organs, cutaneous metaplastic carcinoma does not appear to be necessarily associated with a high mortality rate.14 Based on the few reported cases in the literature with albeit limited follow-up intervals (median: 19 months), the overall recurrence and metastasis rate is 22% with a mortality of 11%.1–7,15 Data from a recent meta-analysis indicate that younger age at presentation, a history of recent growth in a long-standing tumor, as well as size greater than 2 cm correlate with poor prognosis.18 This analysis further suggests that ‘epidermal derived’ tumors, in which the epithelial component represents either squamous cell carcinoma or basal cell carcinoma, are associated with a better prognosis and a 5-year disease-free survival of 70% compared to ‘adnexal derived’ tumors that are associated with a malignant skin adnexal epithelial component. These tumors are characterized by poor 5-year disease-free survival of 25%.18 While ‘epidermal derived’ metaplastic carcinoma is largely a tumor of sun-exposed sites of the head and neck with a strong predilection for elderly males, those associated with a skin adnexal component are often characterized by a long-standing mass and younger age at presentation.18
Keratoacanthomas showing a deeply infiltrative growth pattern, perineural invasion, and vascular (venous) involvement have occasionally been reported. Such lesions commonly affect the head, particularly the lips and the nose. Despite the apparent absence of metastases, it is difficult to reconcile such features with a biologically benign condition.12 Personal experience (EC) suggests that they do not have a more aggressive behavior. Just as with conventional squamous cell carcinoma, such histologic changes do not necessarily always correlate with an aggressive clinical outcome. Nevertheless, the presence of these traditionally malignant features in an otherwise clinically and histologically typical lesion adds considerable weight to the concept that keratoacanthoma represents a variant of squamous cell carcinoma. Perhaps keratoacanthoma constitutes the most benign end of a spectrum with intermediate more aggressive stages finally merging with overt squamous cell carcinoma. Progression is likely to be dependent on genetic, environmental, and immunological factors.
While earlier studies failed to identify significant differences in H-ras activation, p53 expression, nucleolar organizer region enumeration, cyclins, cyclin-dependent kinases and Ki-67 (MIB-1) proliferation fractions in classical solitary keratoacanthoma, regressing keratoacanthoma and variably differentiated squamous cell carcinomas, data suggest significant differences in the expression of bcl-xL, TP53, and COX-2 as well as telomerase activity
Pathogenesis and histologic features Although metaplastic carcinoma has been described at multiple sites other than the skin, little is known about their histogenesis. Possible explanations include the development of separate neoplasms at the same site, so-called collision tumors, although this appears to be an exceedingly rare phenomenon. Alternatively, epithelial tumors may (by as yet unknown mechanisms) induce sarcomatous change in the adjacent stroma.19 Currently favored, however, is the hypothesis that epithelial tumors undergo further genetic change, enabling metaplastic differentiation towards other epithelial as well as mesenchymal components. This theory is favored by the identification of a single monoclonal population of both epithelial and mesenchymal elements in such tumors from various sites including uterus, gastrointestinal tract, lung, breast, soft tissue, and bladder.20 Recent genomic profiling of cutaneous carcinosarcoma cases suggests that TP53 mutations are common and other perturbations such as inactivating mutations in CDKN2A or
1223 Xeroderma pigmentosum
A
The osteoblastic and chondroblastic components are readily identified on hematoxylin and eosin stained sections while skeletal and smooth muscle differentiation can be confirmed with immunohistochemistry for smooth muscle actin, desmin, or myogenin.
B
Differential diagnosis Since metaplastic carcinoma of the skin is a rare tumor, the diagnosis may be difficult and includes a broad differential. The mesenchymal component must be distinguished from reactive or desmoplastic stroma as well as from atypical fibroxanthoma or spindle cell squamous cell carcinoma. Cutaneous sarcomas such as dermatofibrosarcoma protuberans or leiomyosarcoma may also enter the differential diagnosis. Cutaneous metastases from high-grade sarcomas of bone and soft tissues are infrequent, and only very few cases of primary cutaneous osteosarcoma have been reported in the literature.43,44 It is imperative to recognize the biphasic nature of this neoplasm, i.e., the presence of both the malignant epithelial as well as the malignant mesenchymal components, and careful sampling of the tissue is essential. Metastasis from metaplastic carcinoma of visceral origin constitutes the main differential diagnosis. This is of great importance since metastatic lesions are associated with a much poorer prognosis than primary cutaneous tumors.
oncogenic mutations in PIK3CA are present in both the malignant epithelial and mesenchymal components.21,22 Carcinosarcomas with a basal cell carcinoma epithelial element show the same mutations in PTCH1 characteristic of classic basal cell carcinoma.23
Metaplastic carcinoma of the skin is a biphasic tumor composed of malignant epithelial and heterologous mesenchymal components similar to its counterpart in visceral organs including uterus, ovary, lung, bladder, breast, and larynx. The malignant epithelial component in cutaneous tumors comprises squamous cell carcinoma, basal cell carcinoma, and malignant adnexal neoplasms including malignant pilomatrixoma, spiradenocarcinoma, and eccrine porocarcinoma as well as malignant trichoblastoma and Merkel cell tumor.1–7,14,18,24–37 The mesenchymal component shows histologic features of malignancy and consists of spindled and pleomorphic cells showing marked nuclear atypia, necrosis, and numerous as well as atypical mitotic figures. Osteoblastic differentiation is the most commonly identified heterologous element, followed by chondroblastic differentiation (Figs 24.191 and 24.192). Only rare examples showing skeletal, smooth muscle, myofibroblastic, fibrosarcomatous, or angiosarcomatous differentiation have been reported.29,32,38–41 The mesenchymal component is scattered throughout the tumor and sometimes focally merges with the epithelial proliferation.1–7,24 The pleomorphic spindled cell population may infrequently express cytokeratin but is usually negative for most immunohistochemical markers except vimentin. Expression of p63 may be retained at the transition between epithelial and sarcomatoid components of the tumor.42
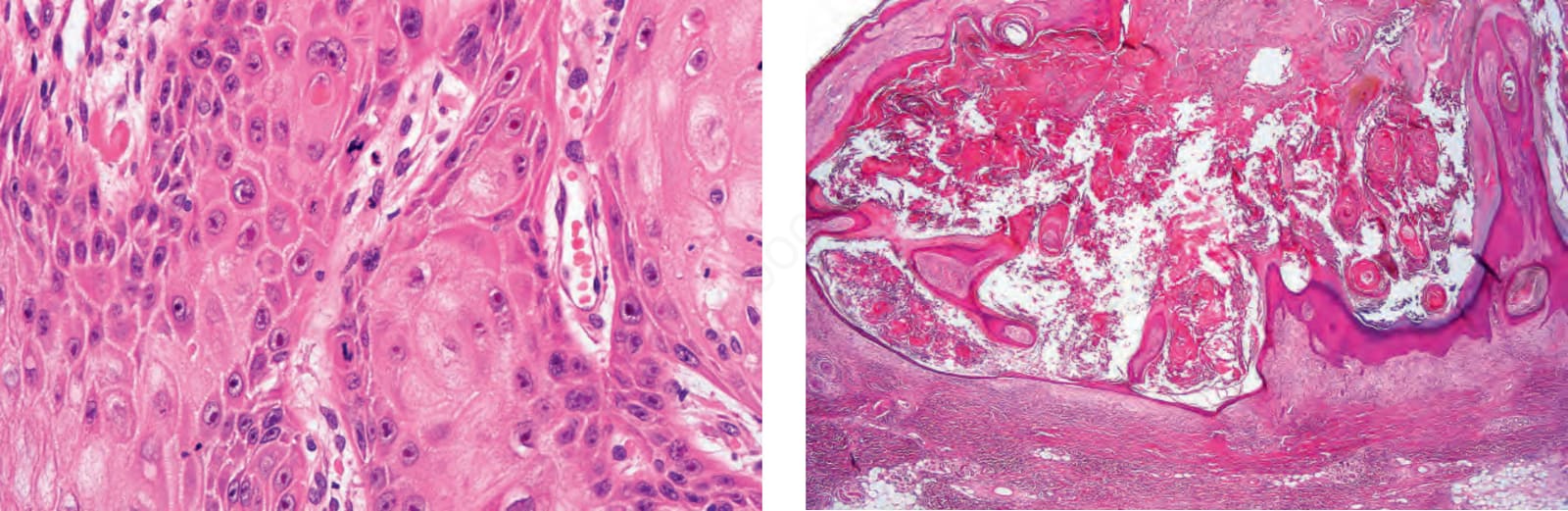
Fig. 24.188 Regressing keratoacanthoma: the keratin plug is still present, but epithelial proliferation is markedly diminished and the floor of the lesion is beginning to flatten. Note the collarette on either side. between keratoacanthoma and frank squamous cell carcinoma. However, their identification within foci of differentiating epithelium in the center of the lesion and/or their disposal by transepidermal elimination appears to correlate well with a diagnosis of keratoacanthoma.129 Rarely, acantholysis is a feature.20 The tumor may show conspicuous mitotic figures, but these are almost invariably normal and are found predominantly within the proliferative epithelium at the periphery of the tumor lobules (Fig. 24.186). Growth of the lesion rarely extends beyond the depth of the sweat glands and is frequently accompanied by a vascular stroma, often heavily infiltrated by lymphocytes, histiocytes, plasma cells, neutrophils, and variable numbers of eosinophils (Fig. 24.187).20
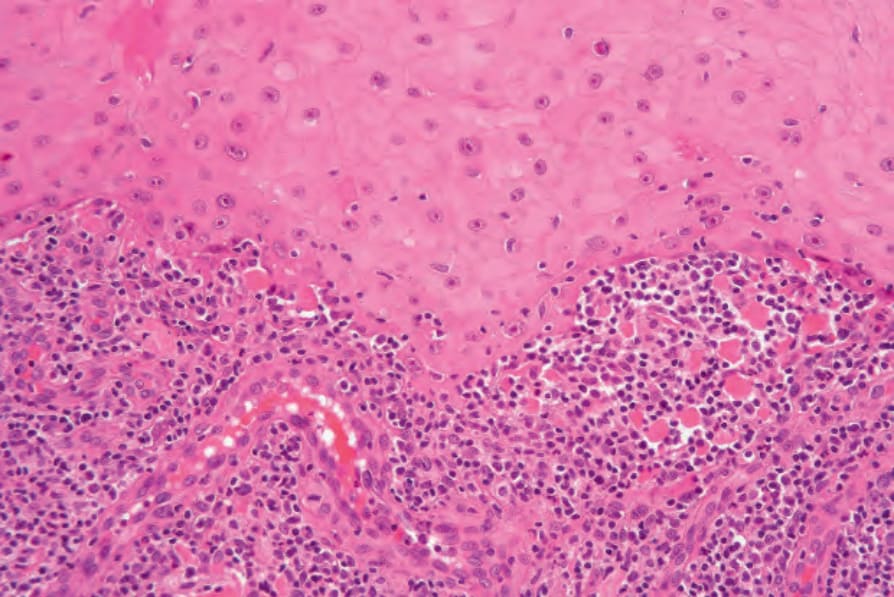
Fig. 24.190 Keratoacanthoma: in this example there are marked interface changes with conspicuous cytoid bodies.
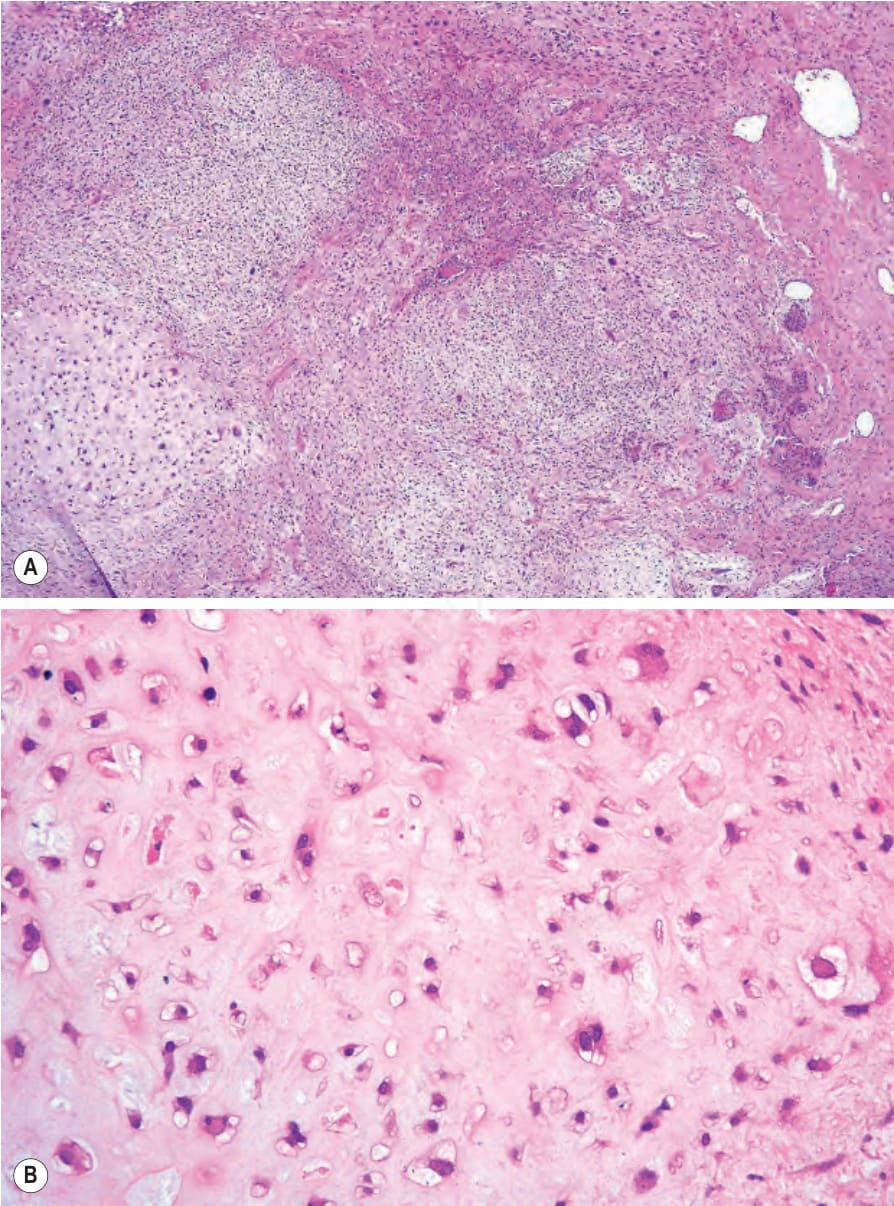
Fig. 24.191 (A, B) Metaplastic squamous cell carcinoma: this example displays chondroid differentiation in addition to squamous elements, hence its alternative designation of carcinosarcoma.