Lobular capillary hemangioma (pyogenic granuloma)
Lobular capillary hemangioma (pyogenic granuloma)
Clinical features Lobular capillary hemangioma (pyogenic granuloma) is common in ingrowing toenails, where it is thought to be induced by the interaction of the nail plate and the lateral nail fold. Nail plate alterations are sometimes present. It is mostly seen in the early decades and presents as a rapidly growing, painful, ulcerated and bleeding, exophytic tumor.1 Subungual location has also been reported.2 There may be local recurrences after excision. Multiple periungual pyogenic granuloma-like lesions may be induced by systemic drugs such as retinoids, ciclosporine, chemotherapeutic agents, and antiretroviral therapies.3–7
The tumors are small (usually less than 1 cm) flesh-colored or red-blue nodules (Fig. 23.71), often associated with paroxysmal pain in relation to minor tactile stimulation or cold exposure.3,4 Nail deformity and osseous defect can be present.5 The recommended treatment is complete surgical excision. Recurrences are rare.2
Pathogenesis and histologic features Glomus tumor arises from modified smooth muscle cells located in glomus bodies. Multiple familial glomus tumors with an autosomal dominant pattern of inheritance have been linked to inactivating mutations in the glomulin gene.6,7 In these ‘familial glomangioma’, the tumors rarely occur in the subungual region1. An association between subungual glomus tumors and neurofibromatosis type I has been reported (with NF1 inactivation or chromosomes copy number change).8–11 MIR143-NOTCH fusions have been described in a series of benign and malignant glomus tumors encompassing some acral lesions.12 The translocation t(1;5) has been reported in only one case of sporadic tumor.13
Histologic features In many cases, histology reveals a mass of exuberant small vascular channels. The epidermis is hyperplasic and frequently ulcerated. There is a proliferation of capillaries associated with a prominent mixed inflammatory cell infiltrate in the dermis. Neutrophils and plasma cells are usually predominant. The stroma can be loose and edematous or fibrotic in the late stages. Rarely, ungual lesions are polypoid and show a well-developed lobular architecture. The lobules are composed of aggregates of capillaries and venules with or without discernible lumina, lined by plump endothelial cells, and surrounded by a layer of smooth-muscle actin positive pericytes.8
Glomus tumors are composed of glomus cells, vessels, and smooth muscle cells. According to the relative proportions of these components, they are divided into three groups: ‘solid glomus tumor’, ‘glomangioma’, and ‘glomangiomyoma’.11
Glomus tumor is usually well circumscribed, but some clusters of cells can be observed around vessels outside the main tumor mass. Solid glomus tumor is composed of sheets of glomus cells surrounding capillaries. Glomus cells are uniform and round, with pale eosinophilic cytoplasm and a centrally located round nucleus (Fig. 23.72). A basal lamina, highlighted by PAS, surrounds each cell. In glomangioma, the vascular component is prominent and composed of numerous dilated vascular spaces. Glomangiomyoma is characterized by gradual transition from glomus cell to elongated cells resembling mature smooth muscle cells. Glomus tumors are positive for smooth muscle actin and type IV collagen. h-Caldesmon, desmin, and CD34 may also be positive.4
Differential diagnosis In elderly patients or patients with acquired immunodeficiency syndrome, the differential diagnosis encompasses nodular Kaposi sarcoma, which is characterized by a prominent spindle cell component and positivity for human herpesvirus 8.
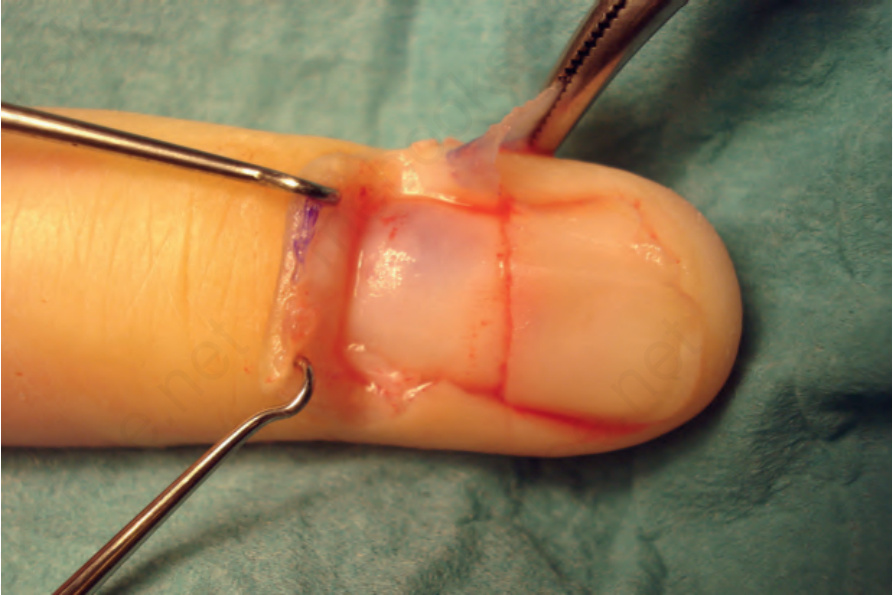
Fig. 23.71 Glomus tumor: there is an ill-defined bluish tumor deep to the proximal nail plate. Courtesy of B. Richert, MD, Université de Liège, Belgium.
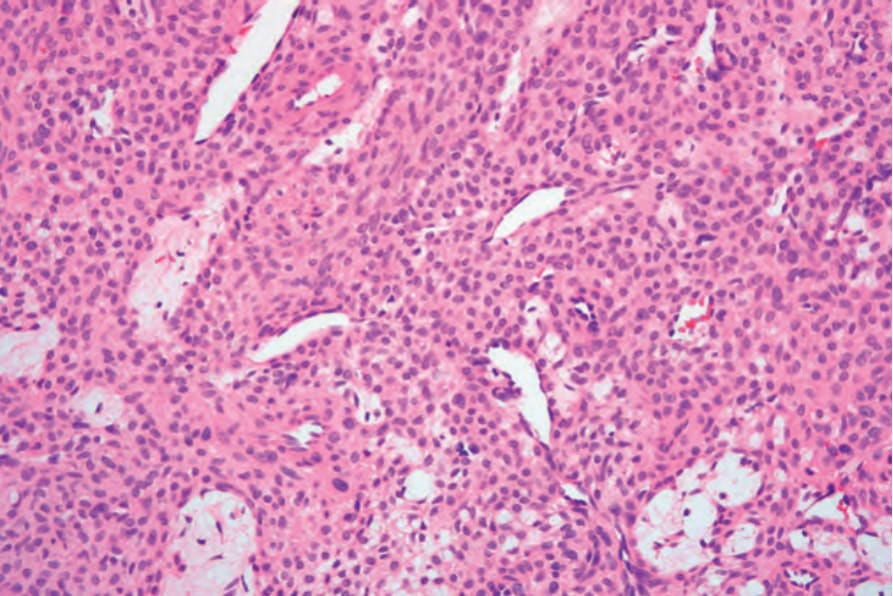
Fig. 23.72 Glomus tumor: medium-power view showing thin-walled dilated vessels surrounded by typical glomus cells.