Superficial acral fibromyxoma
Superficial acral fibromyxoma
Clinical features
Superficial acral fibromyxoma (SAFM), also called digital fibromyxoma, is a distinct clinicopathological entity, described by Fetsch et al. in 2001.1
Similar tumors of the nail bed have also been reported as ‘cellular digital fibromas’.2,3
This neoplasm has a wide age range with a peak incidence in middle-aged adults. It shows a predilection for males and occurs mainly on the fingers and toes, with more than 50% of cases involving the nail bed (Fig. 23.68).4,5 The lesion presents as a solitary, slow-growing, and painless tumor. Erosion of the underlying bone is present in 3% of the cases.
SAFM is a benign tumor, but local recurrences are observed in 24% of the cases with positive margins on initial biopsy. Occasional cases with atypical histologic features (see below) are reported, but this is not associated with aggressive behavior.6 To date, no tumor has metastasized.6 Complete excision and follow-up are recommended.
1152 Diseases of the nails
membrane antigen (EMA) are rarely expressed. Recently, loss of Rb1 immunoexpression and Rb1 deletion confirmed by FISH have been reported in a few tumors.8
Differential diagnosis The differential diagnosis of SAFM encompasses benign and malignant myxoid and spindle cell tumors showing a predilection for the distal extremities. Myxoid neurofibroma is rare at acral sites and is consistently positive for S100 protein. Sclerosing perineurioma is composed of spindled and epithelioid cells arranged in a whorling pattern within a hyalinized collagenous stroma.9 It is positive for EMA and sometimes CD34. Superficial angiomyxoma is lobulated and composed of spindled or stellate cells usually admixed with neutrophils in a myxoid matrix with prominent small blood vessels in the background.10 Myxoid dermatofibrosarcoma protuberans is exceedingly uncommon and almost never occurs on the toes and fingers.11 It is more infiltrative, usually negative for EMA, and is associated with the t(17;22) translocation. Low-grade fibromyxoid sarcoma does not usually involve the fingers and toes and is characterized by curvilinear vessels, and long fascicles of spindle-shaped cells with mild cytological atypia. The tumor is associated with t(7;16) or t(11;16) translocations12 and MUC4 is positive in tumor cells, and this is a highly sensitive and relatively specific marker. Myxoinflammatory fibroblastic sarcoma, which has a predilection for subcutaneous soft tissue of the extremities, shows a prominent inflammatory infiltrate and characteristic bizarre tumor cells with vesicular nuclei and inclusion-like nucleoli.13 The proximal part of onychomatricoma, corresponding to the peduncle, is dome-shaped and its stroma can be very similar to superficial acral fibromyxoma, but onychomatricoma is covered by a characteristic hyperplastic onychogenic epithelium.14 A rare variant of synovial sarcoma described as minute synovial sarcoma is an important differential diagnosis.15 These rare lesions of less than 1 cm have a predilection for the hands and feet and may involve the digits but do not tend to involve the nail. Myxoid monophasic examples may be similar to SAFM. However, the former often displays calcifications and tumor cells are usually negative for CD34 and positive not only for EMA but also for keratin and CD99. Cytogenetic analysis demonstrates the t(X;18) translocation.
Histologic features Tumors are dermal and/or subcutaneous, with only rare bone involvement. Lesions can be circumscribed but not encapsulated or ill defined.1,6 Some tumors have a collarette or are polypoid. A ‘grenz zone’ is often seen separating the epidermis from the tumor. Lesions are moderately cellular, composed of stellate and spindled cells with pale eosinophilic cytoplasm with random, loose storiform, or fascicular growth patterns. The cells are embedded in a myxoid, myxocollagenous, or collagenous matrix, often with accentuated vasculature and increased numbers of mast cells (Figs 23.69 and 23.70). Occasional multinucleated cells can be present, and a lipomatous component has been described in one case that probably represents a spindle cell lipoma.7 Cartilaginous or osseous metaplasia rarely occurs. Occasional cases present scattered cells with atypical features such as enlarged, irregular, and hyperchromatic nuclei (‘degenerative change’). No necrosis, lymphovascular, or perineural invasion is seen.6
SAFM appears to be of fibroblastic origin. Immunohistochemically, most of the cases express CD34. CD10 is often positive.7 CD99 and epithelial
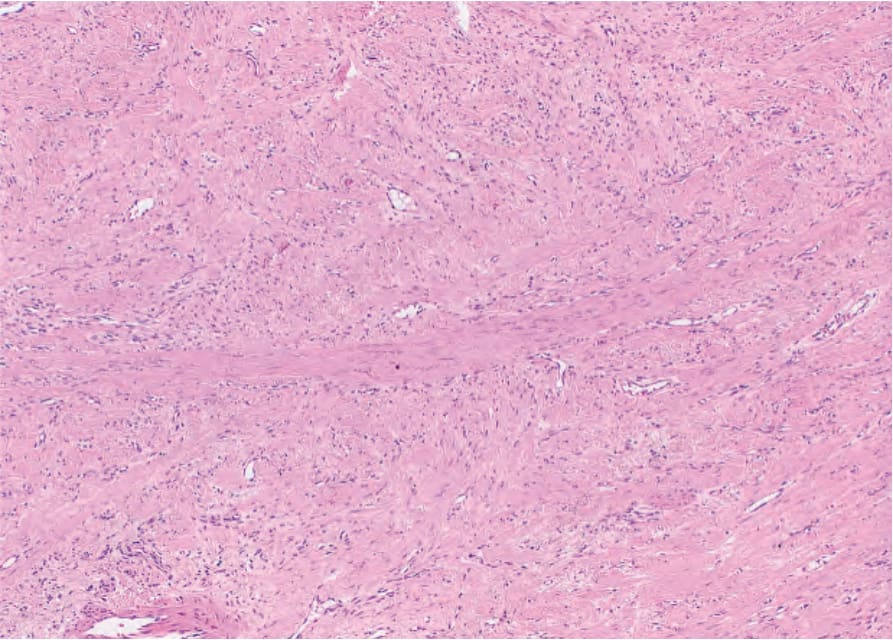
Fig. 23.69 Superficial acral fibromyxoma: fibrous dermal tumor with spindled cells and numerous capillaries.
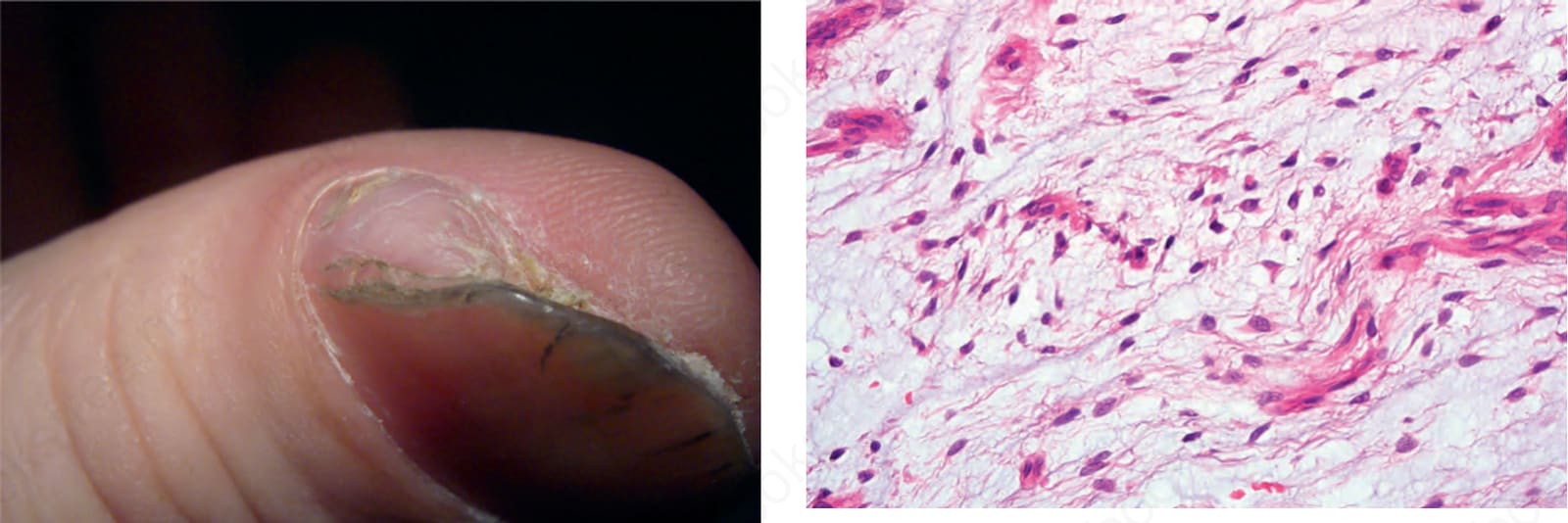
Fig. 23.70 Superficial acral fibromyxoma: high-power view of a sparse population of spindled cells in a myxoid stroma. Courtesy of B. Cavellier-Balloy, MD. Paris, France.
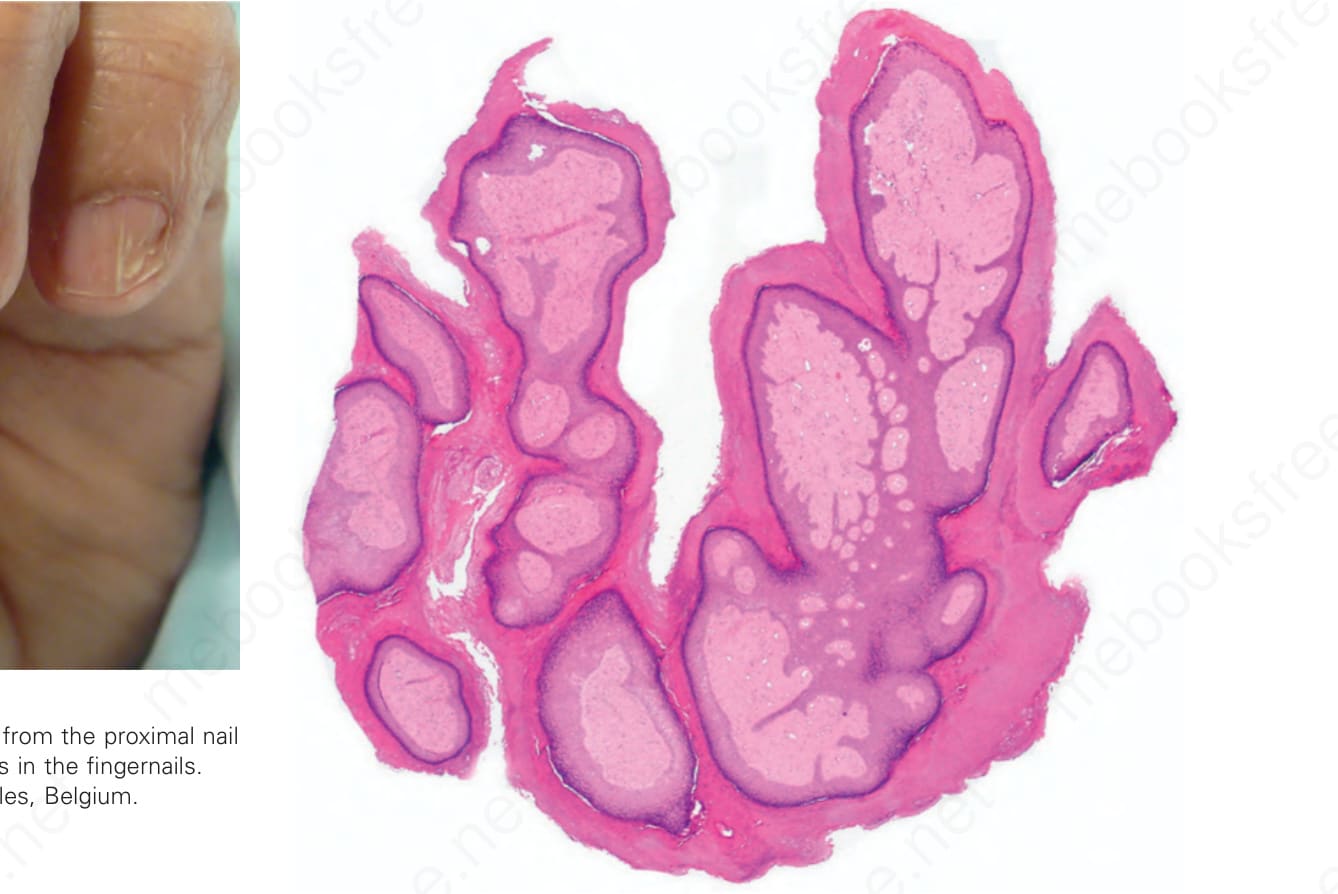
Fig. 23-68 (caption embedded in image / 圖說烘焙於圖內)