Onychomatricoma
Onychomatricoma
Clinical features Onychomatricoma is a rare benign matrix tumor, with distinct clinical and histologic features, first described in 1992 by R. Baran.1 Similar tumors of the nail matrix have also been reported as ‘onychoblastoma’, ‘unguioblastoma’, and ‘unguioblastic fibroma’.2,3 It mainly occurs on fingers, less frequently on toes, with no sex predilection. It usually occurs in Caucasian middle-aged and elderly patients.4 The lesion is solitary, rarely multiple.5,6 It is characterized by thickening of the nail plate with pronounced longitudinal ridging, yellow discoloration (xanthonychia) along the entire length of the nail plate, multiple splinter hemorrhages, and a tendency towards transverse overcurvature of the nail (Fig. 23.61). Unusual clinical presentations such as longitudinal melanonychia or pterygium have also been described.7,8 Surgical excision is the recommended treatment. Recurrence may be observed. Association of onychomatricoma with onychomycosis is not infrequent.5.
1150 Diseases of the nails
Histologic features Nail avulsion discloses a pedunculated villous tumor of the matrix with characteristic distal digitations extending into multiples holes in the proximal nail plate (Fig. 23.62).9 This results in the thickened funnel-shaped nail plate. Distal nail plate clipping, showing multiple lacunar spaces may be a clue to the diagnosis.10
positive fibroblastic cells with random orientation and increased numbers of mast cells. In some cases, cells with bizarre hyperchromatic and pleomorphic nuclei and multinucleated giant cells have been reported (Fig. 23.64).3 The matrix is collagenous, myxocollagenous, or myxoid. In the deeper part of the lesion, the stroma is usually less cellular with thicker collagen bundles oriented around the same horizontal axis. Stromal cells express CD34. In very few cases, CD10, a marker of the onychodermis, was tested and reported diffusely expressed in the stroma.11–14
This fibroepithelial tumor has the configuration of an ‘anemone’, and the histologic features are quite different in the distal and proximal zones of the tumor.
The distal zone is characterized by multiple ‘glove finger’ papillary projections covered by a matrix-type epithelium which is devoid of stratum granulosum and keratinizes through an eosinophilic keratogenous zone (Fig. 23.63).6,9 The proximal zone, corresponding to the peduncle, is dome-shaped in transverse sections. It is lined by a papillomatous matrix-type epithelium, with vertically oriented deep invaginations into the stroma. These invaginations surround optically empty cavities in a characteristic V-shaped configuration. The recognition of matrix-type epithelium with V-shaped depressions is crucial to make the diagnosis of onychomatricoma on fragmented or incomplete specimens which lack the ‘glove finger’ papillary projections. The stroma is moderately to highly cellular, composed of CD34
Differential diagnosis The differential diagnosis includes fibrokeratoma and fibroma of the nail matrix.15 Both are characterized by the absence of multiple papillary projections and the presence of a granular layer and hyperkeratosis. According to Perrin, the papillomatous type of onychocytic matricoma may mimic onychomatricoma, but displays smaller holes in the nail plate, more basaloid cells and lacks the typical fibrous stroma of onychomatricoma.16
Onychomatricoma, especially its proximal part, can also be confused with superficial acral fibromyxoma (AFM; acral fibromyxoma); however, the latter lacks the matrix-type epithelium with characteristic V-shaped invaginations.
1151 Soft tissue and bone tumors

Fig. 23.61 Onychomatricoma: note the thickening of the nail plate with longitudinal ridging, yellow discoloration, and excessive curvature.
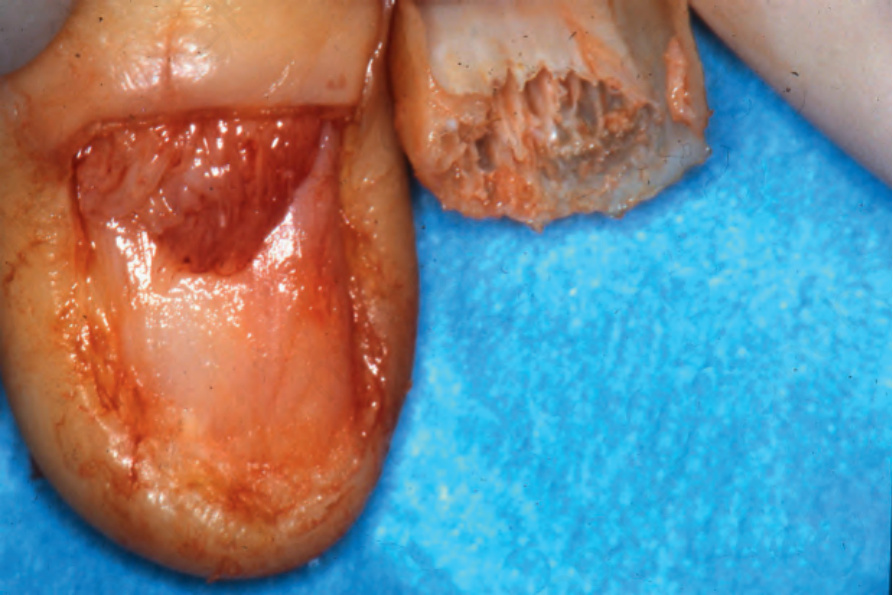
Fig. 23.62 Onychomatricoma: the typical gross appearances are seen after avulsion of the nail plate.
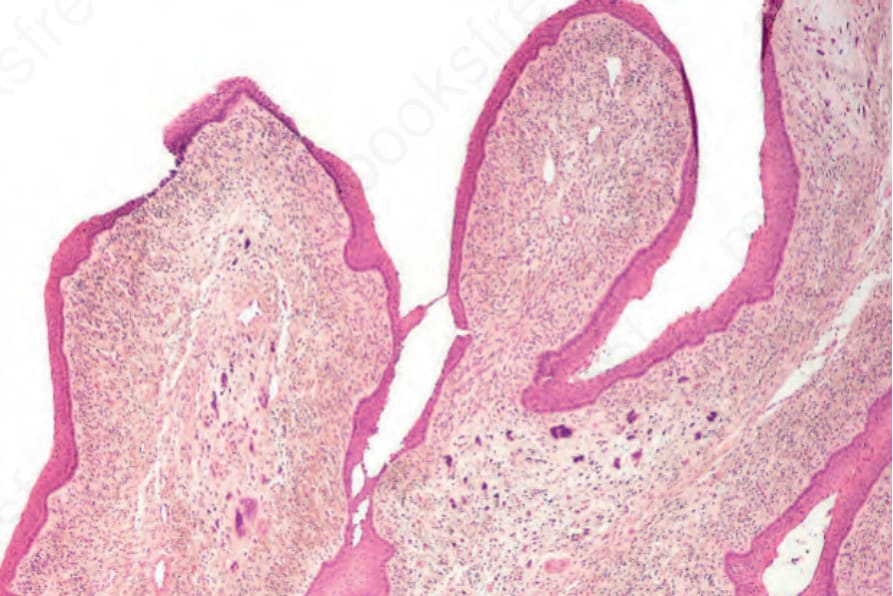
Fig. 23.63 Onychomatricoma: scanning view showing the ‘glove finger’ papillary projections covered by matrix type epithelium.
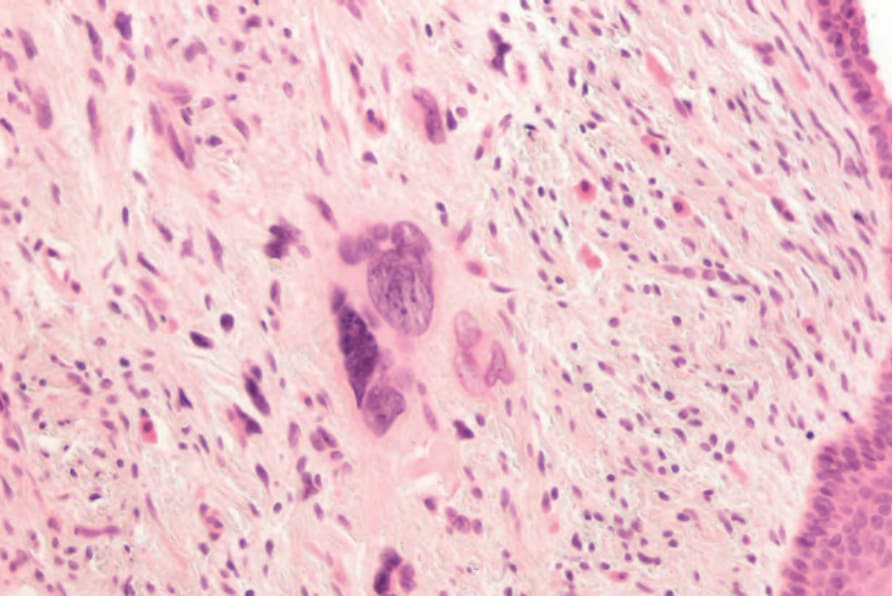
Fig. 23.64 Onychomatricoma: the stroma is highly cellular with marked nuclear pleomorphism. Note the conspicuous mast cells.
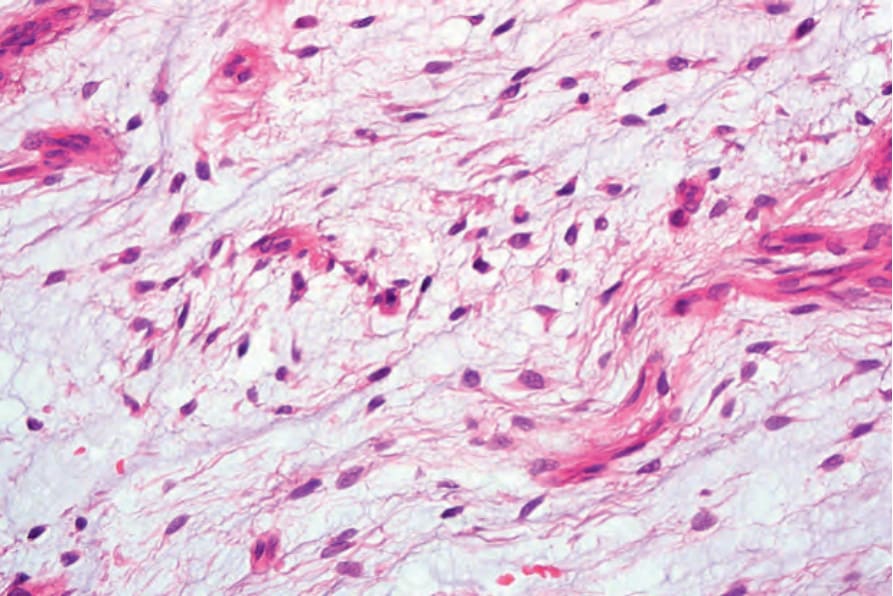
Fig. 23.65 Koenen tumors (tuberous sclerosis): typical lesion emerging from the proximal nail fold of the fourth finger and multiple longitudinal depressions in the fingernails. Courtesy of B. Richert, MD, PhD, Université Libre de Bruxelles, Belgium.