Subungual (distal digital) keratoacanthoma
Subungual (distal digital) keratoacanthoma
Clinical features Subungual keratoacanthoma is a rare variant of keratoacanthoma. It has a predilection for the thumb, index, and middle fingers. It is more frequently observed in males with an age range of 28–76 years.1 Characteristically, it is a rapidly growing tumor (within a period of weeks), always painful and located in the distal part of the nail bed. Partial onycholysis precedes the appearance of a keratotic crusted nodule. The distal digit is sometimes erythematous and edematous. More rarely, the lesion affects the PNF and may cause a painful paronychia (Fig. 23.50).1 Radiological examination reveals a well-circumscribed osteolytic area, with no sclerosis or periosteal reaction. It results from pressure erosion. Spontaneous regression is uncommon. Multiple subungual keratoacanthomas have been described as a late manifestation of incontinentia pigmenti in which case they present almost exclusively in females. These are also named subungual tumors of incontinentia pigmenti.2,3
Pathogenesis and pathological features The pathogenesis of subungual keratoacanthoma is poorly understood. The role of trauma, oncogenic HPV, and exposure to steel wool has been inconclusively reported.1,4,5 The presence of many dyskeratotic cells in the subungual tumors of incontinentia pigmenti may result from increased apoptosis. Interestingly, incontinentia pigmenti is due to mutations in the NEMO gene involved in the regulation of apoptosis.3
amelanotic melanoma,9 or basal cell carcinoma10 causing longitudinal erythronychia have been reported.11,12
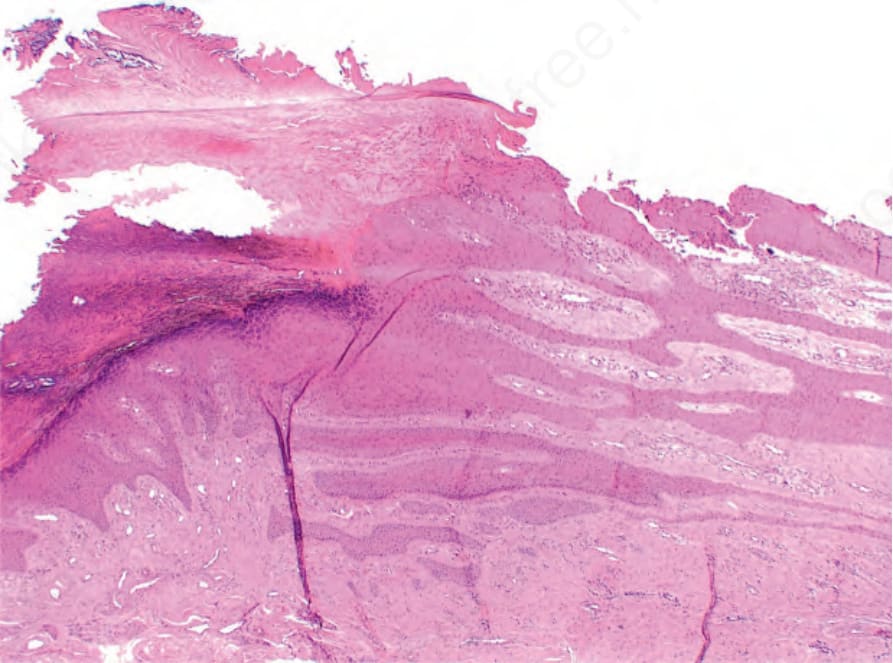
Fig. 23.49 Onychopapilloma: distal subungual hyperkeratosis and marked nail bed papillomatosis. The nail plate had been avulsed during surgery.

Fig. 23.50 Keratoacanthoma: the tumor is located in the proximal part of the nail apparatus. There is painful paronychia and focal nail plate destruction.