Melanoma
Melanoma
Clinical features Nail apparatus melanoma, also called subungual melanoma, is rare, accounting for only 1.4% to 2.8% of all cutaneous melanomas in the United Kingdom.1,2 Its incidence is higher in African-Americans (15–20%)3
1142 Diseases of the nails
Location Sex Age (years) Onset Clinical presentation Pathology
1 Soyer and Kerl1 Left, Toe 1 F 4 C Well circumscribed, blue-black, 1.2 × 0.4 cm lesion on the proximal nail fold with minute satellite lesions
Combined nevus
2 Vidal et al.2 Right, Toe 1 M 20 C 0.9 cm in diameter, bluish nodule in the distal nail bed and hyponychium
Common blue nevus
3 Duhard3 Left, Finger 1 F 50 Bluish macule in the matrix with distal fissuring of the nail plate
Atypical blue nevus
4 Causeret et al.4 Right, Toe 1 F 42 A Ovoid-shaped blue spot, in the distal matrix associated with ethnic longitudinal melanonychia on several nails
Cellular blue nevus
5 Smith et al.5 Right, Finger 3 M 61 A Wide (almost total) heterogeneous brown-black melanonychia
6 Moulonguet- Michau, Abimelec3
Common blue nevus
Right, Finger 1 M 42 A Triangular blue-black macule in the lateral part of the lunula, with longitudinal groove in the nail plate
7 Moulonguet- Michau, Abimelec3
Common blue nevus
Left, Toe 1 F 32 A Blue macule in the lateral part of the lunula Common blue nevus
8 Kim et al.6 Right, Finger 1 F 44 A Longitudinal melanonychia and bluish discoloration of the lunula
Common blue nevus
9 Dalle et al.7 Right, Finger 2 F 34 A Blue-gray, well-limited, semicircular spot in the middle of the lunula, with superficial linear erosion of the nail plate
10 Naylor et al.8 Left, Finger 4 F 40 A (during childhood)
Common blue nevus
Semicircular dark blue discoloration of the proximal nailbed and matrix, with pseudo clubbing
Combined blue nevus
11 Gershtenson et al.9 Right, Toe 2 F 21 C 1.7 × 2.3 cm irregularly shaped, sharply delineated, blue black plaque on the proximal and lateral nail folds, with longitudinal melanonychia
Cellular blue nevus
12 Lee et al.10 Right, Finger 3 F 64 A Black longitudinal melanonychia (?) Common blue nevus
and also in Japanese (up to 23%).4 The incidence, however, is actually the same across racial groups but, as nonacral skin melanoma is less frequently seen in pigmented people, their proportion of subungual lesions is higher.5 Nail melanoma is known to be associated with a poor prognosis, mainly because of late diagnosis.6–8 One study found that 52% of cases had been misdiagnosed by the first clinician to see the patient. This was responsible for an 18 months median delay in diagnosis.9
Melanoma and longitudinal melanonychia Melanoma was observed in 6% of single-digit longitudinal melanonychia cases in adults.10 It is extremely rare in children with only about 14 reported cases.11–14 In a series of 44 subungual melanomas, 30% presented as longitudinal melanonychia, 36% as total melanonychia, and 5% presented as a tumor with residual longitudinal melanonychia, meaning that about 70% of nail melanomas actually started with a longitudinal melanonychia.15 One should be particularly careful with longitudinal melanonychia appearing on a single digit in a patient older than 60 years, especially if the lesion is located on the thumb or big toe. In a pigmented population, longitudinal melanonychia caused by a melanoma can be associated with racial longitudinal melanonychia on other nails.16
The ABCDE rule for cutaneous melanoma also applies to the longitudinal pigmented band. Thus, if it is:
• Asymmetrical,
• has Blurred borders,
• has a heterogeneous Color,
• has a Diameter of greater than 6 mm,
• and if the lesion is Evolving, the probability of a melanoma is high. Periungual pigmentation (Hutchinson sign) or nail plate dystrophy are also clues to the diagnosis of nail melanoma (Fig. 23.39). An ABCDEF rule for subungual melanoma has also been suggested which includes a family or personal history of dysplastic nevi or melanoma.17
Dermatoscopic examination of longitudinal melanonychia due to melanoma reveals a brown color in the background and irregular brown longitudinal lines with disruption of parallelism.18 A pigmented band involving more than two-thirds of the nail plate, gray or black color together with irregular brown pigmentation, granular pigmentation, nail dystrophy, dots, and globules are also suggestive of melanoma.19–21
A mass below the nail, loss of the nail, and ulceration of the nail bed are observed in later stages.22 Rarely, nail melanoma may present as a brown-black spot in the distal nail bed.23
1143 Melanoma
Amelanotic melanoma Amelanotic melanoma of the nail apparatus represents 20% to 30% of lesions compared with less than 7% in other cutaneous melanomas.24 It usually presents as a chronic paronychia, a torpid granulomatous ulceration, a wartlike keratotic tumor, or a pyogenic granuloma-like lesion (Fig. 23.40). Clinical misdiagnosis is particularly common in amelanotic melanoma.25 Four cases of in situ amelanotic melanoma have been described: three presented as lichenoid nail alterations and one as an erythronychia. 26,27
Pathogenesis and histologic features There is no demonstrable link between the development of subungual melanoma and excessive exposure to ultraviolet light. Although trauma is commonly reported in patients with these tumors, its role in pathogenesis has not been conclusively established.8
In situ melanoma In situ melanoma usually arises in the nail matrix from where it can extend to the ventral part of the PNF or to the nail bed. It is characterized by an increased number of melanocytes in the basal cell layer. In a study published in 2008, the mean number of melanocytes was 58.9 per 1 mm stretch of epithelial-stromal junction (range, 39–136) compared with 15.3 (range, 5–31) for benign melanocytic hyperplasia.28 Because of the distribution of matrix melanocytes, nail apparatus melanoma may also arise from suprabasal melanocytes with atypical melanocytes predominating in the lower third of the matrix epithelium and contrasting with sparse basal melanocytes.29 In in situ melanoma, single melanocytes predominate over nests in most fields but rare small nests are often present.22,28,30 Nuclear atypia is evident, as is pagetoid spread (Figs 23.41 and 23.42). In early lesions, the atypia is often focal and moderate, as is the pagetoid spread.
the melanoma, histologic alterations frequently only consist of mild atypical melanocytic hyperplasia with rare melanocytic pagetoid spread. It sometimes only reveals epidermal hyperpigmentation.
Invasive melanoma Invasive melanoma is characterized by atypical melanocytes infiltrating the dermis (Figs 23.43–23.45). Even if in situ melanoma starts in the nail matrix, dermal invasion tends to occur first in the nail bed dermis.35,36 Subungual melanoma with an intraepithelial component is often diagnosed as an acral lentiginous variant but many cases show overlapping features with superficial spreading melanoma.8 Indeed, marked acanthosis, elongation of the rete ridges, and lentiginous proliferation of atypical melanocytes typical of acral lentiginous melanoma are usually observed in thin subungual lesions. With increasing thickness, junctional tumor cell nests develop, with pagetoid spread of individual melanocytes and sometimes also nests of tumor cells.37
Scattered atypical melanocytes with hyperchromatic nuclei are a clue to the diagnosis.31 In more advanced lesions, a confluence of single cells is observed, nuclear atypia is more marked, and pagetoid spread can be florid. Most cases are diagnosed as acral lentiginous melanoma. Elongation of the rete ridges is usually less marked than in similar lesions on the palms and soles. Melanocytes are both spindled and epithelioid, and some have long pigmented dendrites.32 ‘Tumor-infiltrating lymphocytes’ have been described as a clue to the diagnosis,8 but this is not confirmed by other authors.31,33
Hutchinson sign Hutchinson sign corresponds to the lateral extension of a nail melanoma onto the periungual tissue (PNF, hyponychium, and digital pulp or lateral nail folds). It is malignant by definition.34 Although it is tempting for the clinician to take the biopsy from the periungual skin, this is unwise since the histologic appearances can be falsely reassuring. In this lateral part of
In nodular melanoma, the gross appearance varies from a large fungating mass to rather small inconspicuous lesions.38 By definition, there is no intraepithelial growth of tumor cells beyond the adjacent lateral three rete ridges.
In nail apparatus melanoma, the histogenic type, Clark level, and Breslow thickness are more difficult to assess than in comparable skin lesions because the biopsies are often partial and because of the unique nail
1144 Diseases of the nails
anatomy. Equally, the accurate definition of the junction between papillary and reticular dermis can be problematical. In addition, in most cases there is no adipose tissue between the nail bed and periosteum.39 This is why it has been suggested that melanoma extending to the periosteum or invading the underlying bone should be classified as Clark level V.8,38 Concerning Breslow thickness, there is usually no granular layer in the nail matrix and nail bed. The epithelium is often markedly acanthotic, thereby giving a false measurement of tumor thickness.38 A simple classification of Breslow thickness of ≤ 2.5 or > 2.5 mm has produced different survival curves.8 In an English series of 105 patients, the mean Breslow thickness was 4.8 mm. The 5-year survival was 88% for Breslow thickness of 2.5 mm or less, and 40% for melanomas greater than 2.5 mm.1 Other clinicopathological features that have been found to correlate with adverse prognosis in subungual melanoma include advanced age at diagnosis, high number of dermal mitoses, tumor-associated ulceration, amelanotic tumors, and higher stage of disease.8 In a large Australian retrospective study published in 2007, 9% of cases were in situ acral lentiginous melanoma, the commonest histogenic subtype of invasive melanoma was acral lentiginous (67%), followed by nodular (25%) and desmoplastic (7%).8 The majority of tumors were locally advanced at presentation with 79% being Clark level IV or V. The median Breslow thickness was 3.2 mm. The median mitotic rate was 3 per mm2 and 33% of cases demonstrated tumor ulceration.8 In this study, the AJCC (American Joint Committee on Cancer melanoma staging system) staging40 at diagnosis was the most significant predictor of survival to the exclusion of all other variables. Sentinel lymph node biopsy has been reported to be positive in 17% to 24% of patients.8,41

Fig. 23.39 Invasive melanoma: this tumor presented with total melanonychia. Note the Hutchinson sign – pigmentation spreading to the adjacent skin.

Fig. 23.40 Invasive melanoma: this example is amelanotic. Courtesy of J. Van Geertruyden, MD, Hôpital Erasme, Université Libre de Bruxelles, Belgium.
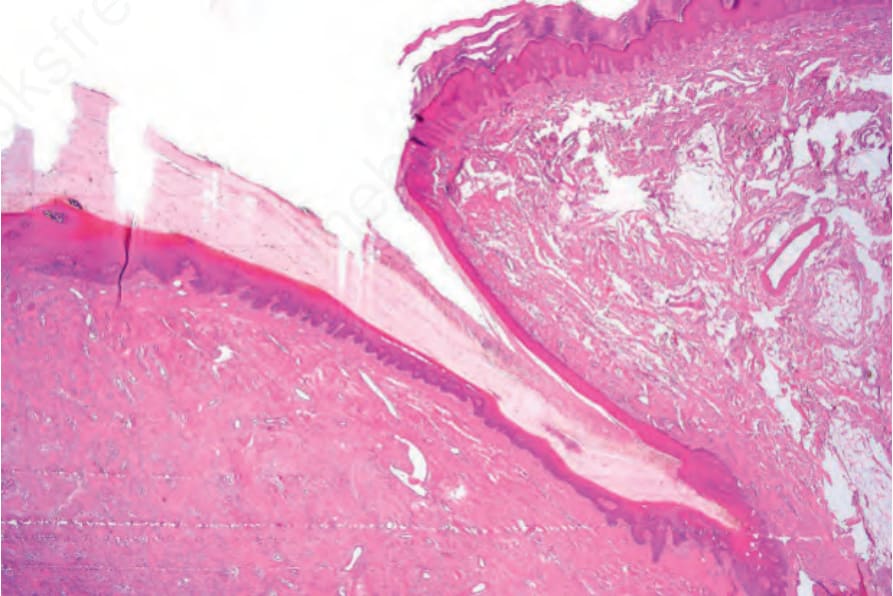
Fig. 23.41 In situ melanoma: scanning view showing nail matrix.
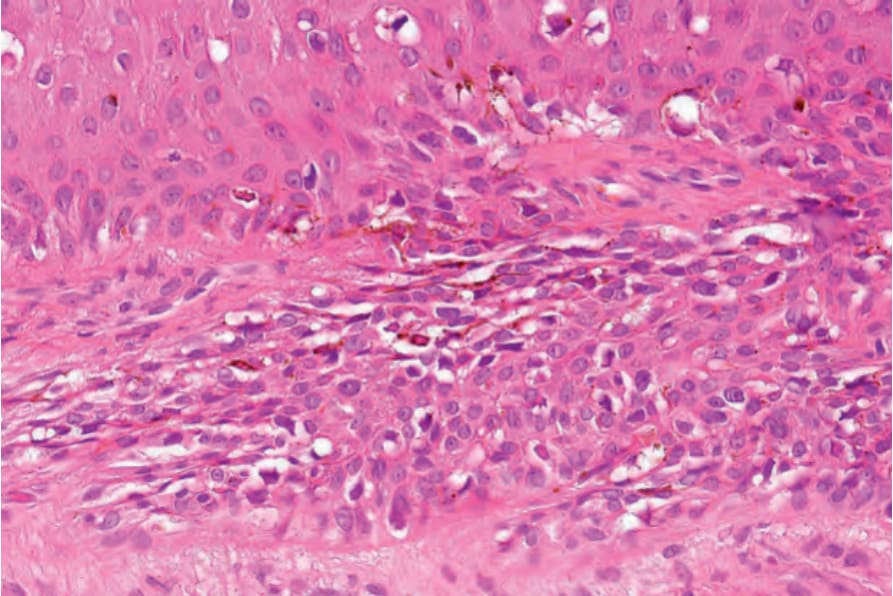
Fig. 23.42 In situ melanoma: basally and suprabasally located atypical melanocytes with surrounding halo are present. The crowded appearance in the lower field results from tangentional sectioning.
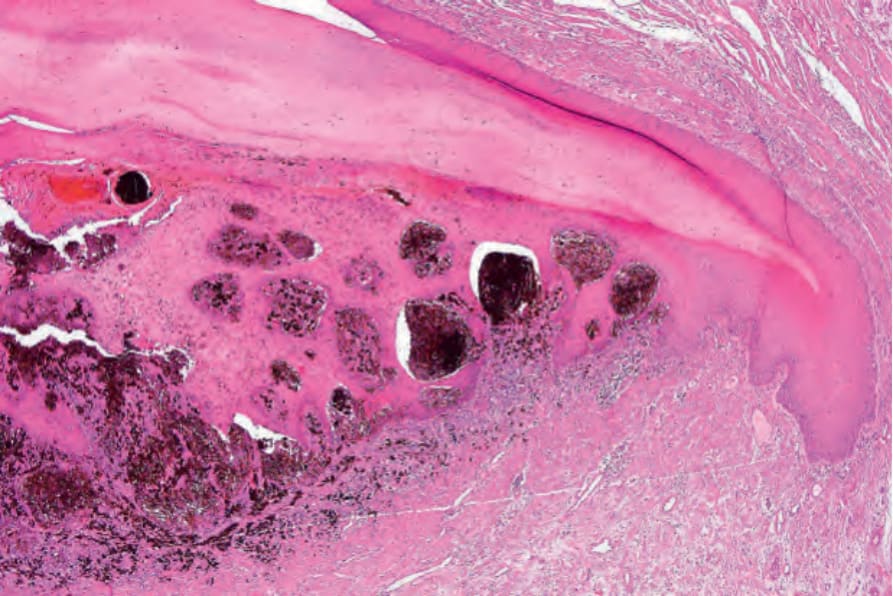
Fig. 23.43 Invasive melanoma: low-power view showing large pigmented nests within the epithelium. Note the lymphocytic infiltrate in the underlying dermis (a useful diagnostic clue) and the conspicuous melanophages.
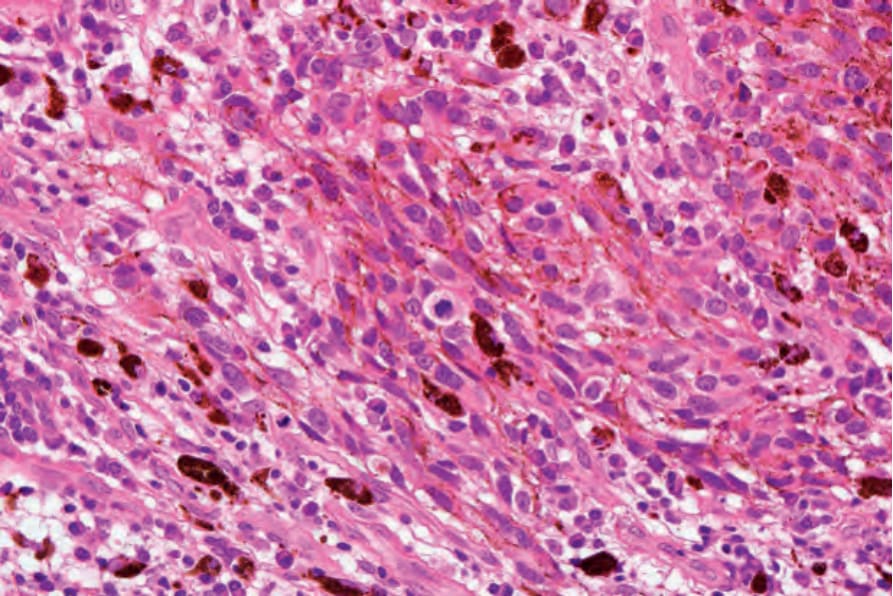
Fig. 23.44 Invasive melanoma: high-power view of the invasive component showing spindled cells and a central mitotic figure.
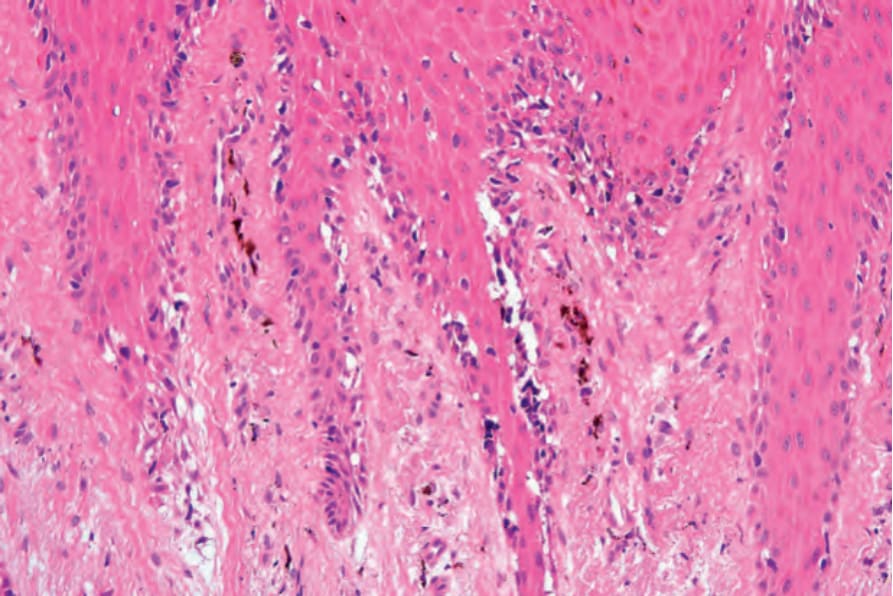
Fig. 23.45 Invasive melanoma: in situ changes are evident in the adjacent epithelium.
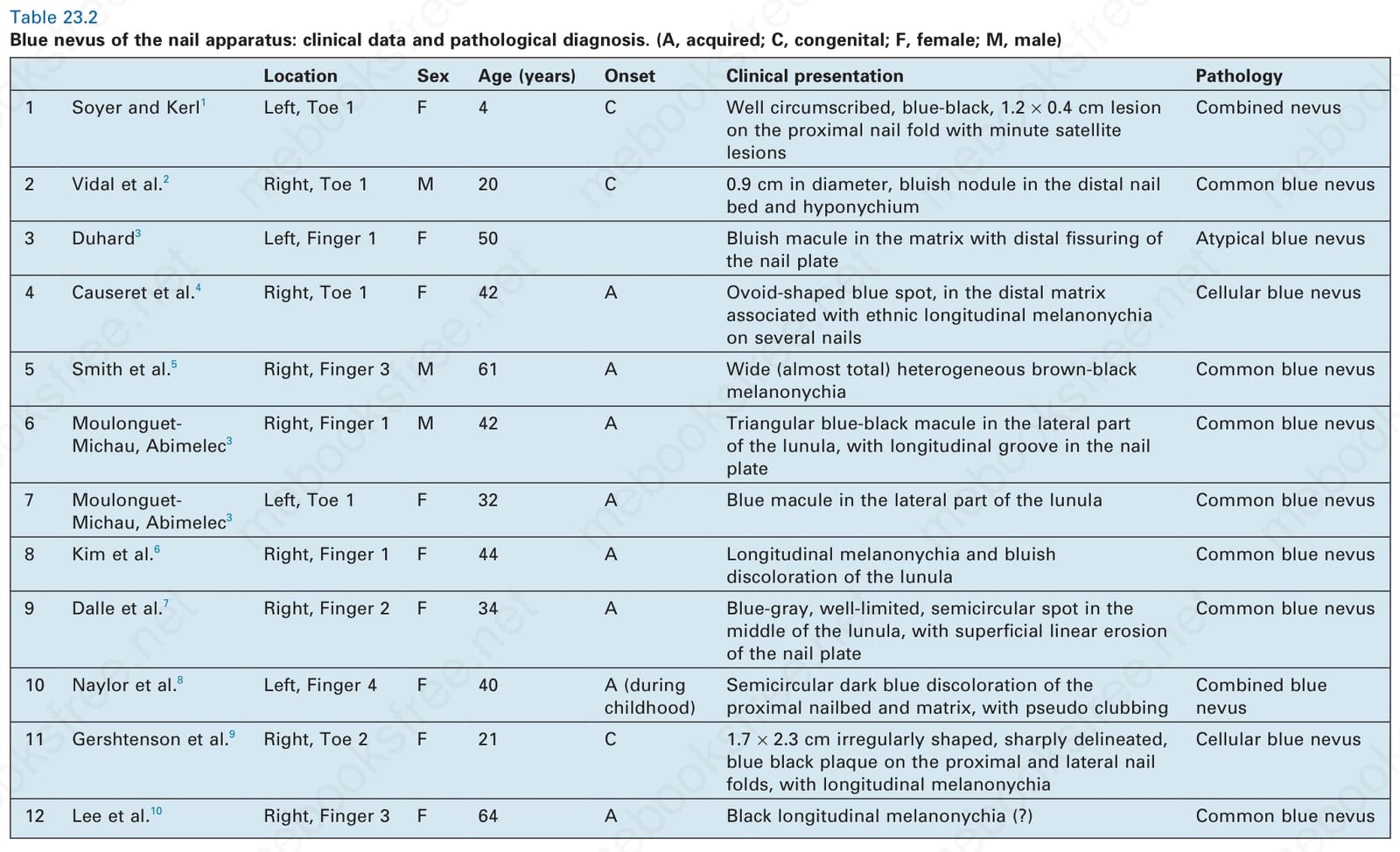
Table 23.2 Blue nevus of the nail apparatus: clinical data and pathological diagnosis. (A, acquired; C, congenital; F, female; M, male)
Fifteen cases of melanoma with osteocartilaginous differentiation (metaplastic melanoma) have been reported (Fig. 23.46), 53% of which were subungual melanomas.42
Immunohistochemistry Limited data have been published about the role of immunohistochemistry in nail apparatus melanoma. In an in situ lesion, HMB-45 has been shown to be the best method for detecting nail apparatus melanocytes.43 Similarly, in another study of nine cases of in situ acral lentiginous melanoma including four subungual lesions, strong positive staining with HMB-45 was seen while S100 protein was only weakly positive or even negative in the atypical melanocytes.32
In our experience of nail melanocytic lesions, immunochemistry is particularly useful for the diagnosis of early melanomas and for the determination of the margins in acral lentiginous tumors. When dealing with intraepithelial melanocytes, the sensitivity is better with HMB-45 than with Mart-1 (Melan A). S100 protein is the least valuable. However, in invasive subungual melanoma, S100 protein is the most sensitive and was the only positive
marker in cases of desmoplastic melanoma and in foci of chondroid differentiation.44 Nuclear markers such as microphtalmia transcription factor and Sox-10 give a more precise quantification of melanocytes as the dendrites are not highlighted and can be more helpful in determining localization of the melanocyte within the matrix.45
Genetics In acral melanoma, mutations in BRAF occur in only 15% of the cases. Activating mutations or amplifications of wild type KIT are found in 15% to 40% and approximately 15% have NRAS mutations. A unique feature is the high frequency of gene amplifications throughout the genome, with amplifications already present in the early phases of the disease.46 A recent fluorescent in situ hybridization (FISH) analysis of seven cases of nail melanoma shows multiple abnormalities, including gain of RREB1, CCND1, and MYC. Loss of CDKN2A appears less common.47
1145 Epithelial tumors
melanoma is rare and few pathologists have significant experience in this field. Moreover, absolute criteria for the diagnosis in early lesions have not been agreed upon.24
It is often a difficult challenge to differentiate very early melanoma from benign conditions.29 Criteria to differentiate in situ melanoma from lentigo have recently been suggested but require validation. Features include high melanocyte density, melanocyte multinucleation, multifocal pagetoid spread, cytological atypia, and/or the presence of a moderately dense lichenoid inflammatory infiltrate. It is equally important, however, not to overinterpret focal pagetoid spread as this is commonly seen in benign nail lesions.28 In nevi, nests usually predominate over single melanocytes, while the reverse is true for in situ melanoma. If the intraepithelial component of the melanoma is lacking, immunohistochemistry may be necessary to differentiate an amelanotic melanoma, and especially a desmoplastic variant,48 from epithelial or mesenchymal tumors.
Differential diagnosis Firm diagnosis of melanoma is often problematic in nail biopsy specimens because the tissue fragment(s) are often tiny. In addition, nail apparatus
When assessing small biopsies, the possibility of nonrepresentative sampling should always be considered and should be clearly stated in the report. A further biopsy should always be considered if clinically appropriate.8
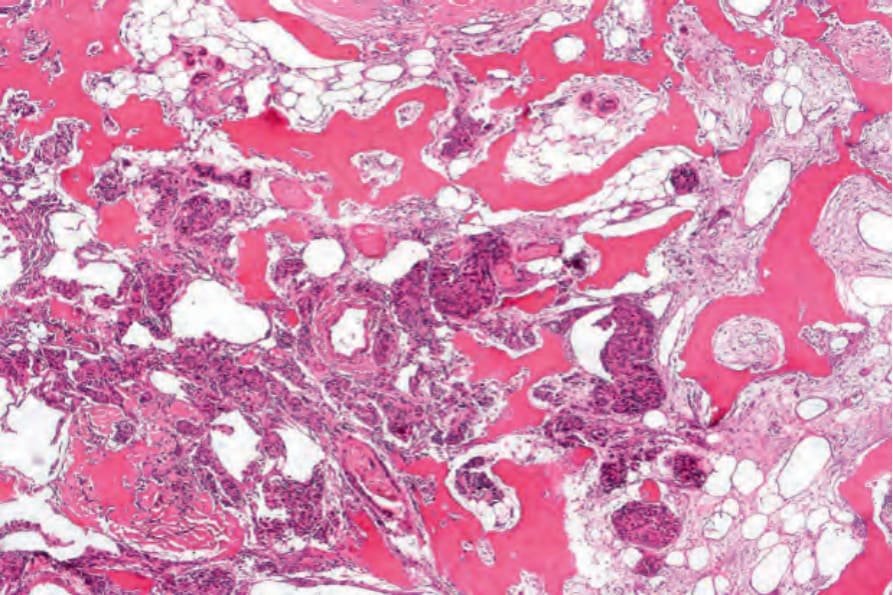
Fig. 23.46 Metaplastic melanoma: this example shows extensive malignant osteoid. Courtesy of Z. Tannous, MD, Massachusetts General Hospital, Boston, USA.