Lentigo and nevus
Lentigo and nevus
Clinical features Lentigo is frequently considered together with melanocytic activation and nevus. In a series of 15 ‘subungual melanotic macules’, 6 lesions showed increased pigmentation only (melanocytic activation) while 9 lesions proved to be a lentigo with an increased density of melanocytes.1 The clinical appearances are indistinguishable from a nevus.2 Lentigo has been reported to account for 9% of single-digit longitudinal melanonychia in adults3 and for 30% in children.2
Differential diagnosis The pathologist can only diagnose melanocytic activation, but cannot determine its precise cause except in pigmented onychomycosis or pigmented Bowen disease.
Longitudinal melanonychia due to fungal infections may show melanin pigmentation of the matrix and nail plate together with nonpigmented fungus in the nail plate. It may also reveal brown-colored hyphae as in onychomycosis caused by the dematiaceous family.
In cases due to pigmented Bowen disease, typical features of Bowen disease are observed (see below) together with melanin pigmentation of the epithelium.
A nevus was observed in 12% of single-digit longitudinal melanonychia in adults but in almost 50% in children. Nevi can be congenital or acquired. Longitudinal melanonychia due to nevi prevails on the fingers, mainly the thumb. Their width measures 3 mm or more, in half of the cases (Fig. 23.36). A brown-black coloration is observed in two-thirds of the cases, periungual pigmentation (benign pseudo-Hutchinson sign) in one-third.2 However, nail matrix nevi can also present as scarcely pigmented bands. The only clinical feature that suggests a diagnosis of nail matrix nevus is onset during childhood. However, nevus can also appear after puberty.3 Dermatoscopic examination of a nevus reveals a brown coloration of the background and regular parallel longitudinal brown lines.4
1141 Melanoma
20% of cases.2 Small numbers of melanophages are commonly scattered throughout the superficial dermis.
Differential diagnosis In situ melanoma is associated with a higher melanocyte density and confluence compared with lentigo.1,5 The pagetoid spread is usually multifocal and can reach the upper epithelial layers. Atypia characterized by angular hyperchromatic nuclei is present. In children, the diagnosis of in situ melanoma should be made cautiously6 and only when there is a severe increase in melanocyte density together with both atypical hyperchromatic nuclei and an obvious pagetoid migration reaching the onychogenous band. Clinical-pathological correlation is also useful: childhood longitudinal melanonychia present for more than 2 years with continuous widening and darkening, and the appearance of periungual pigmentation or nail plate dystrophy is of concern, as is a stable lesion present since childhood that starts to change in adulthood.7 In adults, if the melanocytic hyperplasia is atypical and the biopsy only partial, an early in situ melanoma cannot be excluded and complete excision of the nail apparatus is advisable, especially if the clinical presentation is worrying.
Histologic features Lentigo is characterized by a mild to moderate increase in the number of matrix melanocytes (10 to 31 cells per mm).1 The melanocytes remain in individual units, without confluence. The epidermal rete ridges are often less prominent than in cutaneous lentigo. Cytological atypia is absent or mild. Pagetoid spread can be observed but it is rare or focal. Pigmentation is usually limited to the lower third of the nail epithelium but can be observed throughout its full thickness. Scattered melanophages are frequently observed in the superficial dermis.1,2

Fig. 23.36 Melanocytic nevus: this example presenting as total melanonychia occurred in a 10-year-old boy. (Courtesy of B. Richert, MD, PhD, Université Libre de Bruxelles, Belgium.)
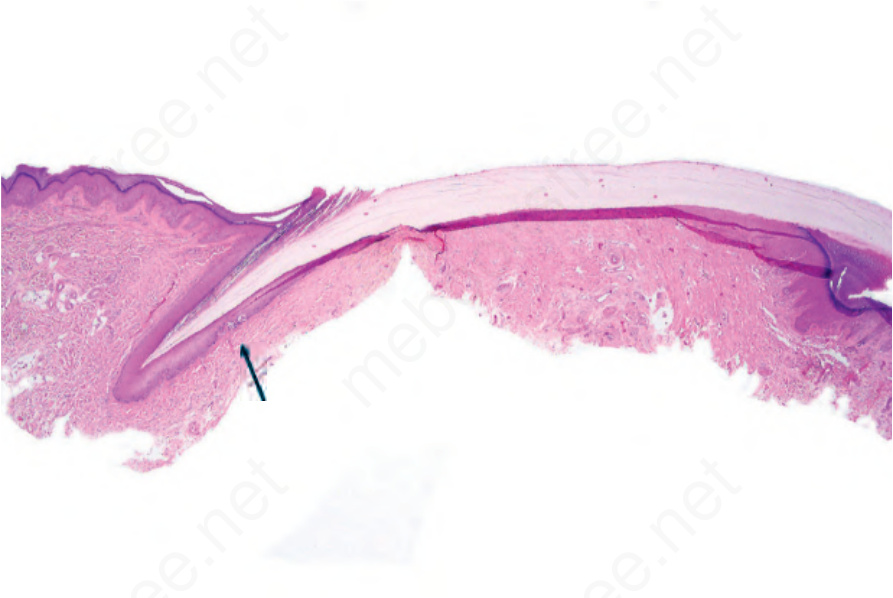
Fig. 23.37 Junctional melanocytic nevus: scanning view showing two junctional nests in the nail matrix (arrowed).
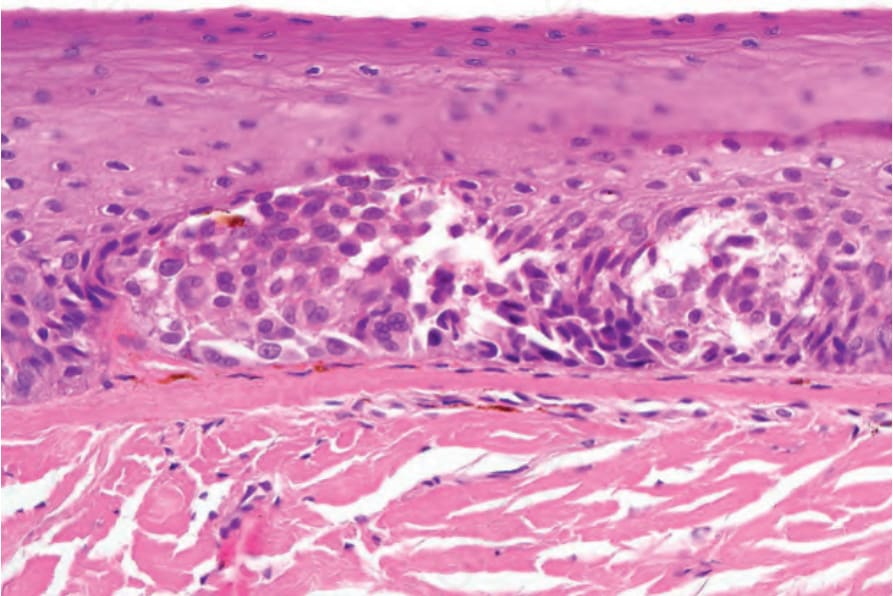
Fig. 23.38 Junctional melanocytic nevus: the nevus cells are uniform. There is no atypia or mitotic activity.