Melanocytic activation
Melanocytic activation
Clinical features Longitudinal melanonychia due to melanocytic activation or stimulation is also called hypermelanosis, functional melanonychia, or melanotic macule.1 The etiologies are multiple and can be classified as physiological, local and regional, dermatological, systemic, and iatrogenic. Laugier-Hunziker syndrome as well as Peutz-Jeghers and Touraine syndrome can be added to this list.2,3 Melanocytic activation is more frequent in patients with darker phototypes and increases with age.4 The pigmented bands frequently involve several nails, but melanocytic activation is also responsible for 73% of single-digit longitudinal melanonychia in adults.5 Dermatoscopic examination reveals a grayish background usually associated with thin regular gray lines.6
Histologic features By definition, there is no increase in the density of melanocytes. Only some melanocytes with pigmented dendrites and pigmented keratinocytes are observed (Figs 23.34 and 23.35). If the pigment is barely visible, a Fontana-Masson stain should be performed. A few melanophages are frequently present in the superficial dermis.
Melanocytic activation is sometimes difficult to differentiate from a lentigo with a slight increase in the melanocyte density.7 Immunostainings with HMB-45 and Mart-1 may be helpful. This, however, is of little therapeutic consequence, as both entities are benign.

Fig. 23.34 Melanocytic activation: scanning view of nail matrix.
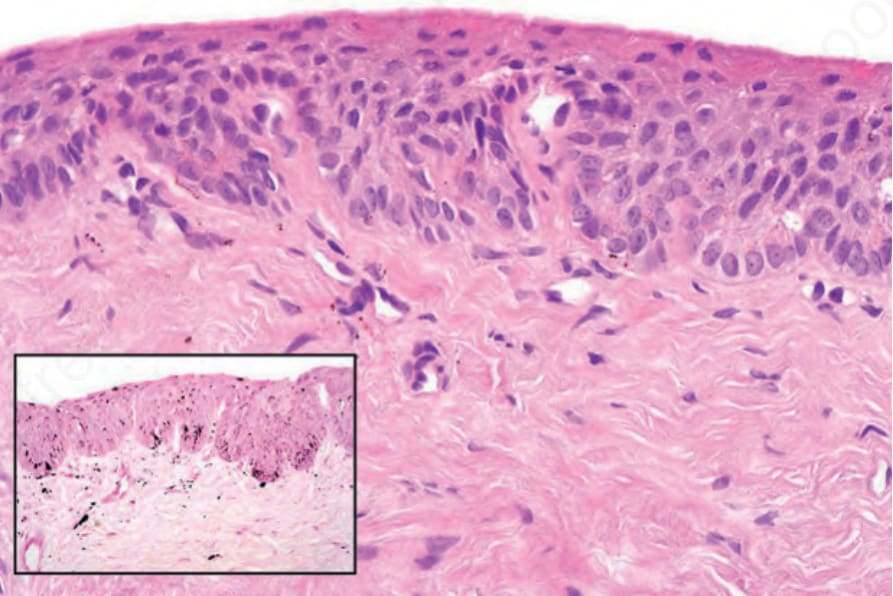
Fig. 23.35 Melanocytic activation: high-power view showing increased pigmentation within the epithelium and melanophages in the dermis (inset: Masson-Fontana stain).