Lichen planus
Lichen planus
Clinical features Nails are affected in 1% to 10% of patients with lichen planus and permanent damage of at least one nail occurs in up to 4% of patients.1,2
1136 Diseases of the nails
Approximately 25% of patients with nail lichen planus have clinical lesions at other sites before or after the onset of nail lesions.3 Fingernails are more frequently affected than toenails. Nail changes are not pathognomonic. However, a diagnosis should be considered when multiple nails are affected by lichenoid nail changes:
• longitudinal ridges and splitting,
• thinning of the nail plate, with or without dorsal pterygium (dorsal expansion of the PNF resulting from the fusion of the ventral aspect of the PNF with the underlying nail matrix and nail bed),
• erythematous patches in the lunula and longitudinal melanonychia (less frequent). All these features are caused by matrix involvement, the most frequent region affected. Involvement of the nail bed is also possible and results in subungual hyperkeratosis and onycholysis. Complete involvement of the nail matrix and the nail bed leads to a total loss of the nail plate with permanent atrophy of the nail area.1 Rarer presentations include erosive nail lichen planus, yellow nail syndrome-like features,4,5 onychopapilloma,6 and nail degloving.7 In children, nail lichen planus has three different presentations: typical nail lesions as above (Fig. 23.23), trachyonychia, and idiopathic atrophy of nails.8 Nail biopsies are frequently performed due to the risk of permanent nail destruction and because treatment often necessitates systemic corticosteroid therapy.
Histologic features Histologic features of nail lichen planus were first described by Zaias.1 He observed that it can involve each of the nail unit constituents separately or together. The matrix is more frequently affected than the nail bed and PNF.3 Punch biopsies confirmed the diagnosis in 85.5% to 100% of the cases.9 Indeed, histologic changes are usually typical showing acanthosis, hypergranulosis, liquefactive degeneration of the basal cell layer with apoptotic cells, and a bandlike superficial lymphocytic inflammatory infiltrate in the superficial dermis (Figs 23.24–23.26). In the matrix and nail bed, a compact horny layer replaces the normal nail plate above the zones of hypergranulosis. Spongiosis can be prominent.10 Numerous plasma cells in the infiltrate have been described.11
Differential diagnosis Matrix hypergranulosis is a major feature of nail lichen planus. However, it has also been observed in spongiotic trachyonychia, psoriasis, and pustular psoriasis.12 Nail lichen planus is indistinguishable from the nail changes seen in graft-versus-host disease13,14 and lichenoid drug reactions. In lupus erythematosus, the infiltrate is usually more perivascular, with thickening of the capillary wall.15 Lichenoid nail changes have been described in systemic amyloidosis and can be the first sign of the disease. Histology reveals typical amyloid deposits in the superficial dermis of the matrix.16–18
1137 Trachyonychia
Clinical features Trachyonychia means rough nail. The nail is opaque and covered with thin scales (Fig. 23.27). It shows excessive superficial longitudinal ridging. Thinning of the nail plate is responsible for brittleness, which may be associated with koilonychia (spoon nail deformation) and splitting at the free edge. The cuticles are often hyperplastic and ragged. Baran et al. described another form of trachyonychia, called the shiny type, characterized by multiple punctuate depressions that reflect light.1 Trachyonychia may affect one, several, or all 20 nails (twenty-nail dystrophy syndrome). Trachyonychia is mainly observed in three dermatological diseases: lichen planus, psoriasis, and alopecia areata. In alopecia areata, trachyonychia is observed in 12% of the cases in children2 and 3% in adults.3 The incidence of trachyonychia in psoriasis and lichen planus is unknown. Trachyonychia has also been described in association with atopic dermatitis, ichthyosis vulgaris, IgA deficiency, incontinentia pigmenti, pemphigus, and vitiligo.4 Idiopathic trachyonychia, i.e., without any concomitant skin or hair disease, has been reported mostly in children and males.5 Total resolution or marked improvement is observed within the first 6 years in 50% of cases. A nail biopsy is not routinely recommended.6,7
Histologic features Trachyonychia is best investigated with longitudinal biopsies. Trachyonychia associated with alopecia areata usually shows a mild to moderate lymphocytic infiltrate in the superficial dermis, exocytosis of lymphocytes, and mild to moderate spongiosis, without vacuolar degeneration of the basal cell layer (Figs 23.28 and 23.29). The changes predominantly affect the ventral PNF, the proximal matrix, and the hyponychium.5 In so-called idiopathic trachyonychia, spongiotic alterations were observed in 83% of the cases, a psoriatic pattern in 13%, while 4% of cases were due to lichen planus.8 In another series, the proportion was different, with spongiotic dermatitis occurring in 45%, psoriasis in 26%, lichen planus in 18.5%, and non-specific changes in 10%.9 The results yielded in a third study cannot be compared, as 65.6% of cases were not idiopathic but associated with different known dermatoses.10
Differential diagnosis The possibility that idiopathic spongiotic trachyonychia is actually a variant of alopecia areata limited to nails has been suggested.3 However, the exact significance of spongiosis is not fully understood. Spongiosis is frequently
1138 Diseases of the nails
Histologic features A longitudinal nail biopsy from two cases of lichen striatus restricted to a nail showed a moderately dense bandlike lymphohistiocytic inflammatory cell infiltrate affecting the PNF, the nail bed, and the dermis of the nail matrix.1 It was associated with exocytosis, slight spongiosis, focal hypergranulosis, and dyskeratotic cells in the nail matrix epithelium and with slight focal spongiosis and exocytosis in the ventral PNF, nail bed, and hyponychium. Dyskeratotic cells surrounded by lymphocytes were also present in the nail bed.1

Fig. 23.19 Psoriasis: note the scar from the prior lateral-longitudinal biopsy. The nail plate is dystrophic and thickened. Courtesy of B. Richert, MD, PhD, Université Libre de Bruxelles, Belgium.
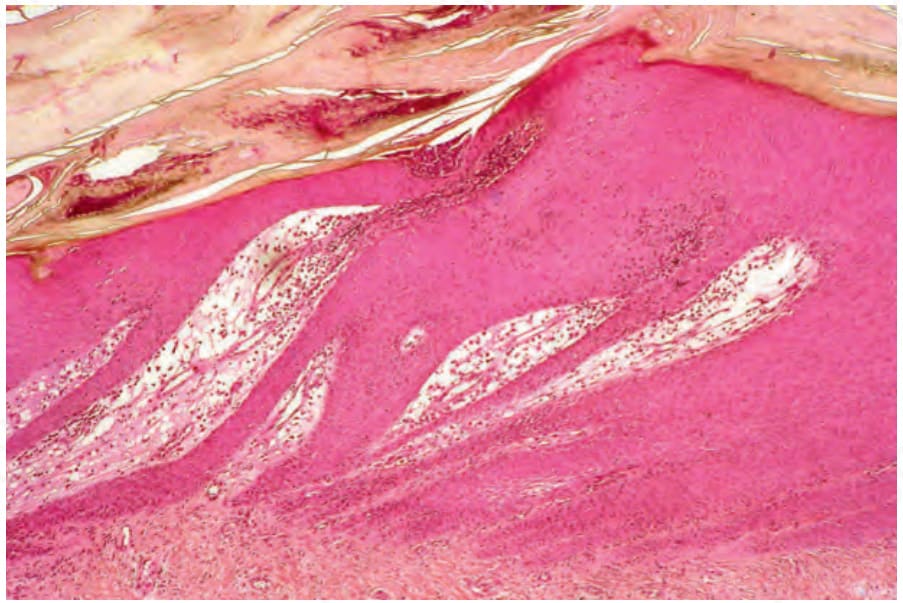
Fig. 23.20 Psoriasis: distal matrix involvement. Note the psoriasiform hyperplasia, neutrophil exocytosis, and subungual hyper- and parakeratosis. There is edema in the superficial dermis with vasodilatation.

Fig. 23.21 Pustular psoriasis: there is crusting, parakeratosis, and a macropustule.
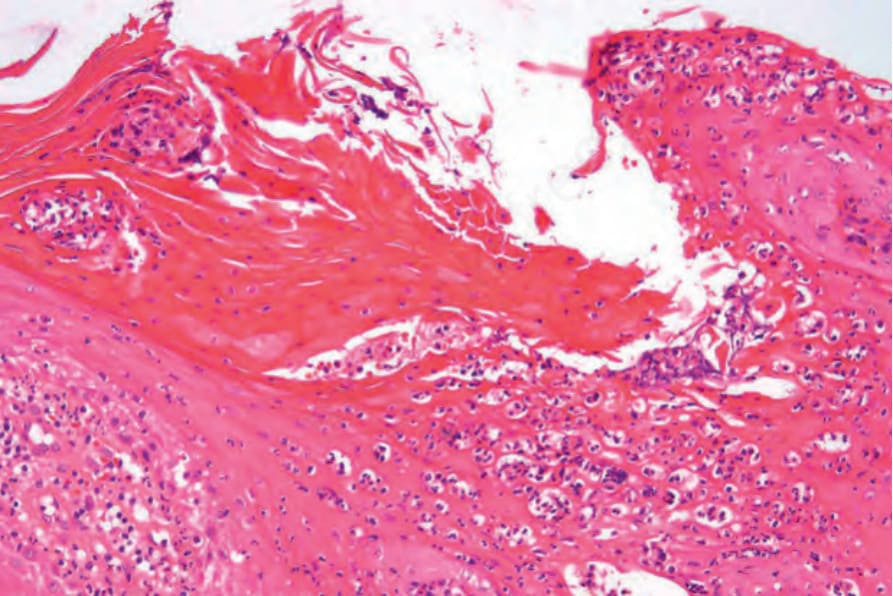
Fig. 23.22 Pustular psoriasis: high-power view showing conspicuous spongiform pustules. Cases such as this should always be examined for the presence of fungi.

Fig. 23.23 Lichen planus: typical nail changes in a 3.5-year-old boy.
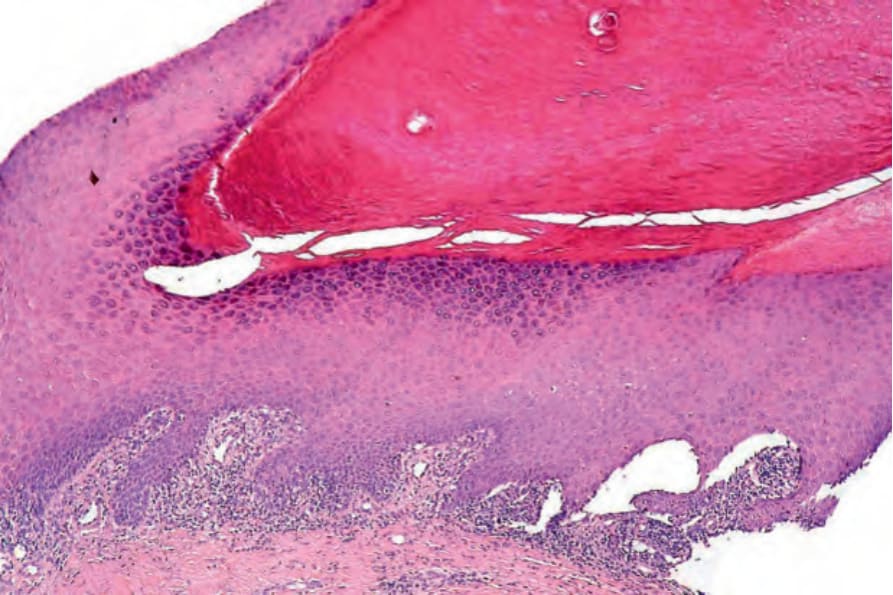
Fig. 23.24 Lichen planus: this is a biopsy of the proximal nail matrix. Note the hypergranulosis, hypertrophic acanthosis, and superficial bandlike infiltrate.
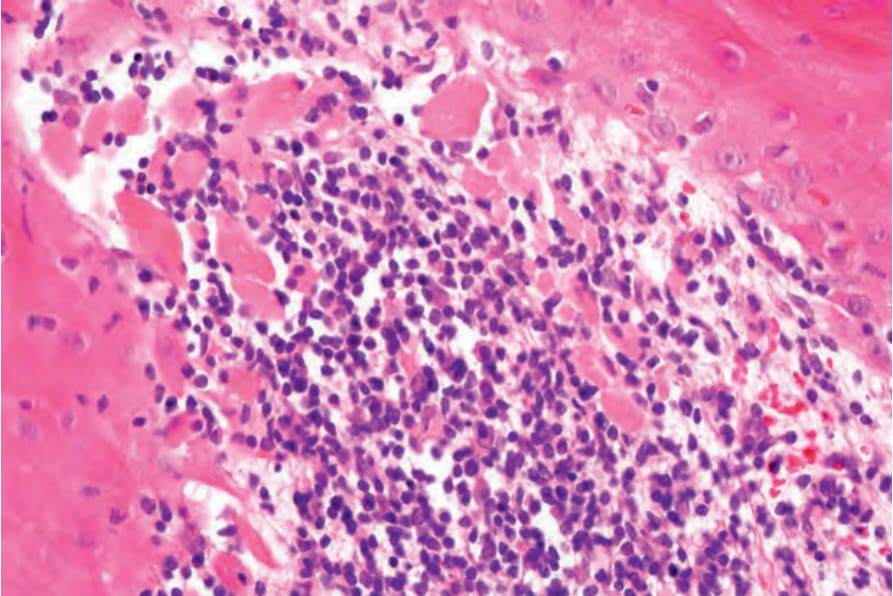
Fig. 23.25 Lichen planus: high-power view showing conspicuous cytoid bodies.
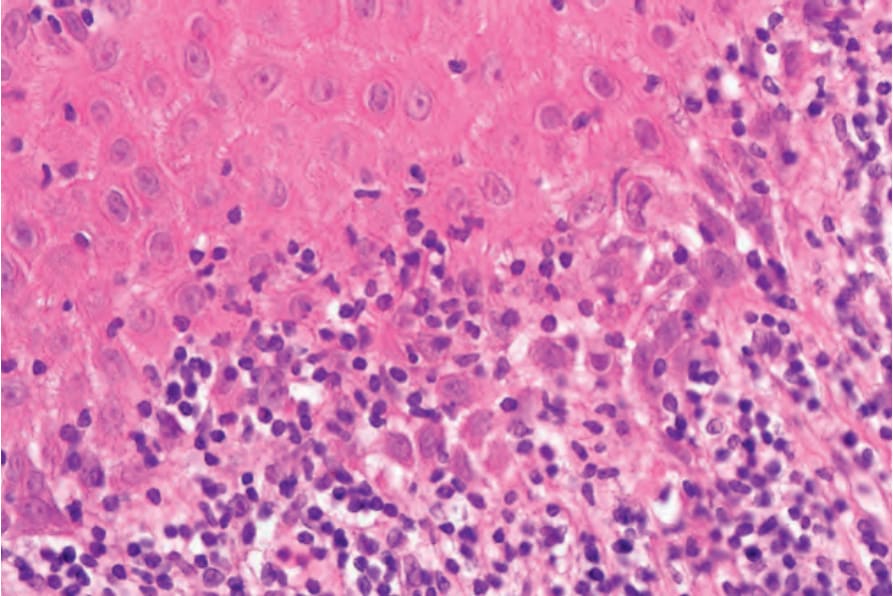
Fig. 23.26 Lichen planus: high-power view showing interface change and lymphocytic infiltration.

Fig. 23.27 Trachyonychia: there is loss of translucency and the nails appear rough and jagged at their distal borders. The cuticles are hyperplastic and ragged. Courtesy of B. Richert, MD, PhD, Université Libre de Bruxelles, Belgium.
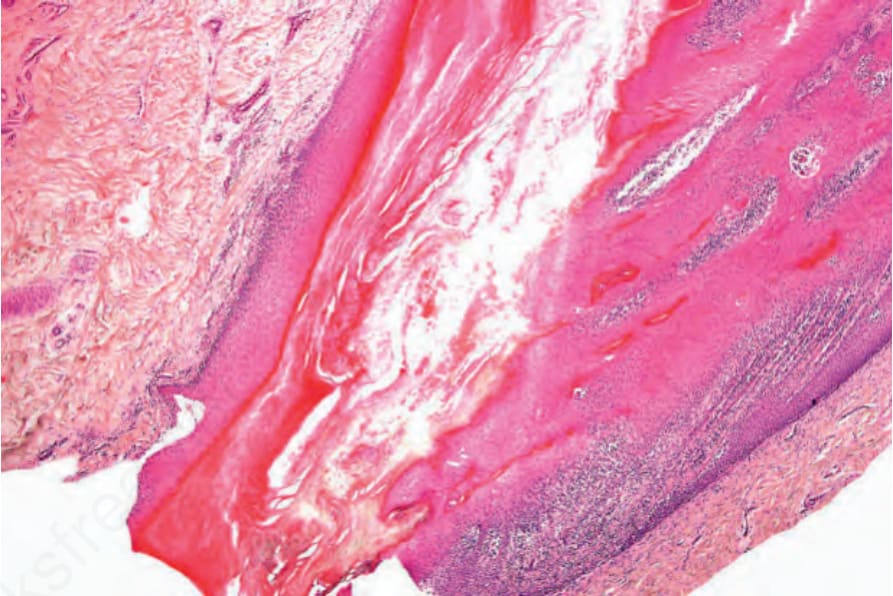
Fig. 23.28 Trachyonychia: there is florid spongiosis with lymphocytic exocytosis. Trachyonychia
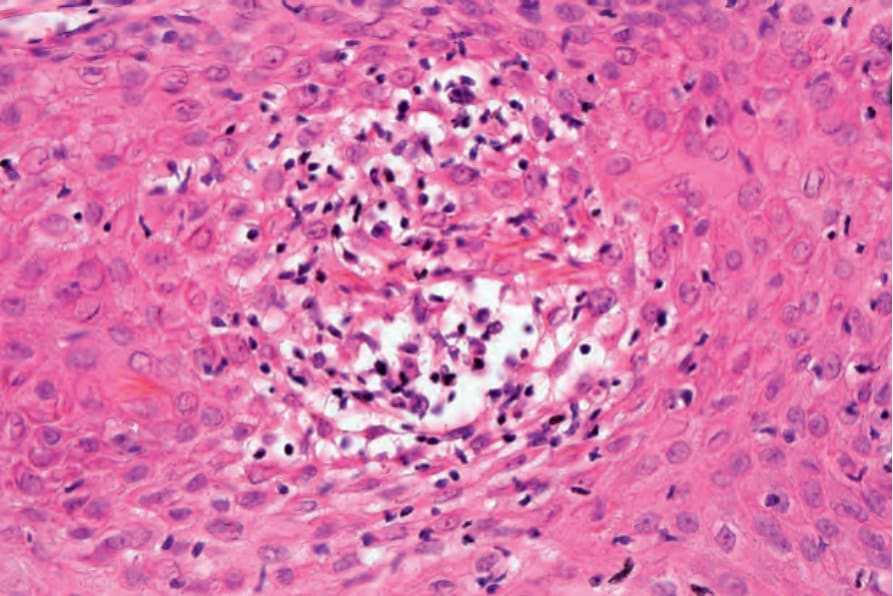
Fig. 23.29 Trachyonychia: high-power view of a spongiotic vesicle.
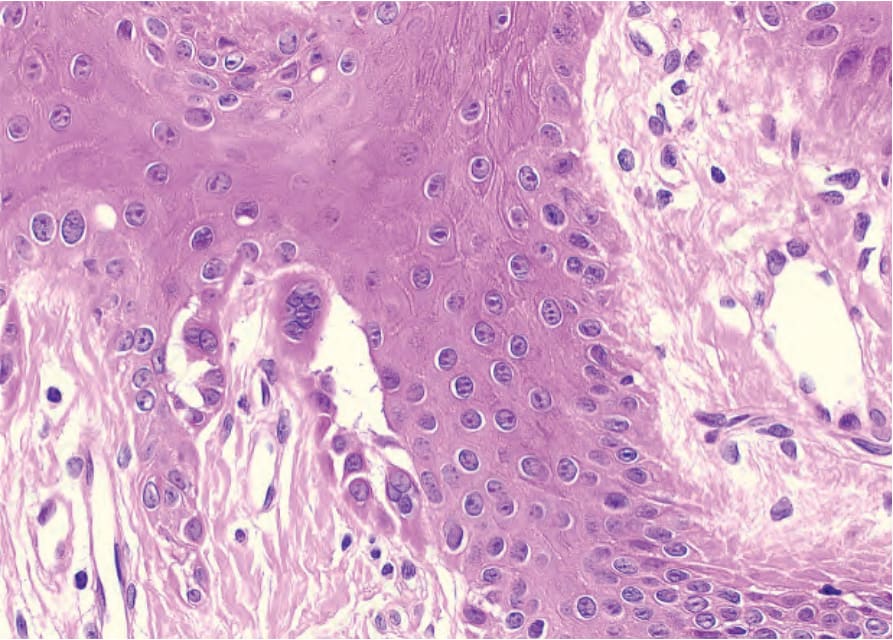
Fig. 23.31 Darier-White disease: suprabasal acantholysis with multinucleated cells.