Acne fulminans
Acne fulminans
Clinical features Acne fulminans was originally described in 1959 as acne conglobata with septicemia by Burns and Colville.1 It is an exceedingly rare systemic disease which is generally restricted to young teenage males. Very occasionally, however, females are affected.2 Patients – who usually have a background of acne vulgaris – present with a sudden onset of multiple tender inflammatory nodules and plaques on the face, neck, upper chest, and back. These are soon replaced by extensive areas of liquefying necrosis which ulcerate and slowly heal with severe scarring (Fig. 22.196).3 The condition is generally self-remitting.
1123 Rosacea
Characteristics
Subtype Erythematotelangiectatic Flushing and persistent central facial erythema with or without telangiectasia.
Papulopustular Persistent central facial erythema with transient, central facial papules or pustules or both.
Phymatous Thickening skin, irregular surface nodularities and enlargement. May occur on the nose, chin, forehead, cheeks, or ears.
Ocular Foreign body sensation in the eye, burning or stinging, dryness, Itching, ocular photosensitivity, blurred vision, telangiectasia of the sclera or other parts of the eye, or periorbital edema.
Variant Granulomatous Noninflammatory; hard; brown, yellow, or red cutaneous papules; or nodules of uniform size.
*Wilkin, J., Dahl, M., Detmar, M. et al (2002) Standard classification of rosacea: Report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol, 46, 584–587.
Systemic manifestations may include arthralgia, myalgia, and hepatosplenomegaly. In addition, there is fever, malaise, anemia, headaches, weight loss, leukocytosis (sometimes with a leukemoid reaction), raised C-reactive protein, increased liver enzymes, and a raised erythrocyte sedimentation rate, although there is a subset of patients without systemic involvement.4–6 Joint swelling (particularly affecting the iliosacral, iliac, and knee joints) and osteolytic bone lesions predominantly involving the sternum and clavicle may also be present.3,5,7–9 Erythema nodosum is sometimes a feature.4,10 Acne fulminans has been associated with Marfan syndrome, hemophagocytosis, late-onset congenital adrenal hyperplasia, and following measles infection.11–14 Exceptionally, posterior scleritis and a pyoderma gangrenosum-like eruption have been associated.15 Acne fulminans can also be the dermatological manifestation of the synovitis-acne-pustulosis- hyperostosis-osteitis (SAPHO) syndrome.16,17
Severity Papules/pustules Plaques
Mild Few None
Moderate Several None
Severe Many Present
*Wilkin, J, Dahl., M, Detmar, M. et al (2004) National Rosacea Society Expert Committee. Standard grading system for rosacea: report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol, 50, 907–912.
Pathogenesis and histologic features Acne fulminans is of unknown etiology. The restriction to males suggests a hormonal influence. The condition has been reported in monozygotic twins, and occasionally in siblings with identical HLA phenotypes.3,7,18 Factors which may be of importance include infections, abnormal immune responses to P. acnes, immune complex deposition, adverse drug reactions, and after treatment with isotretinoin.3,19–22 Bacterial cultures, however, are negative.3,8 An association with Crohn disease has been documented.23
Histologically, follicular and sebaceous gland destruction with abscess formation is followed by epidermal necrosis and ulceration. Thrombosed hyalinized vessels are seen deep to the ulcer, and hemorrhage is present.3 The surrounding dermis is infiltrated by neutrophils, eosinophils, histiocytes, plasma cells, and giant cells. Lymphocytic vasculitis has been described in early lesions.15 The late stages are characterized by dermal scarring.
Recurrences are common. The term was initially applied to Scandinavians vacationing in Mallorca.3
Histologic features The histologic features are those of a neutrophil-rich folliculitis, followed by necrosis of the follicular epithelium. Abscess formation and comedones are later secondary lesions.1,4
Acne aestivalis should be differentiated from acne vulgaris aggravated by sunlight. With adequate clinical information, it is easy to reach a correct diagnosis.5
Linear IgM and fibrin deposition at the basement membrane region accompanied by fibrin around the sebaceous gland has occasionally been described.3
Bone lesions are characterized by abscess formation with granulation tissue.24

Fig. 22.196 Acne fulminans: note comedones joining together with associated ulceration and crusting. By courtesy of Department of Dermatology, Universidad de Antioquia, Medellín, Colombia.
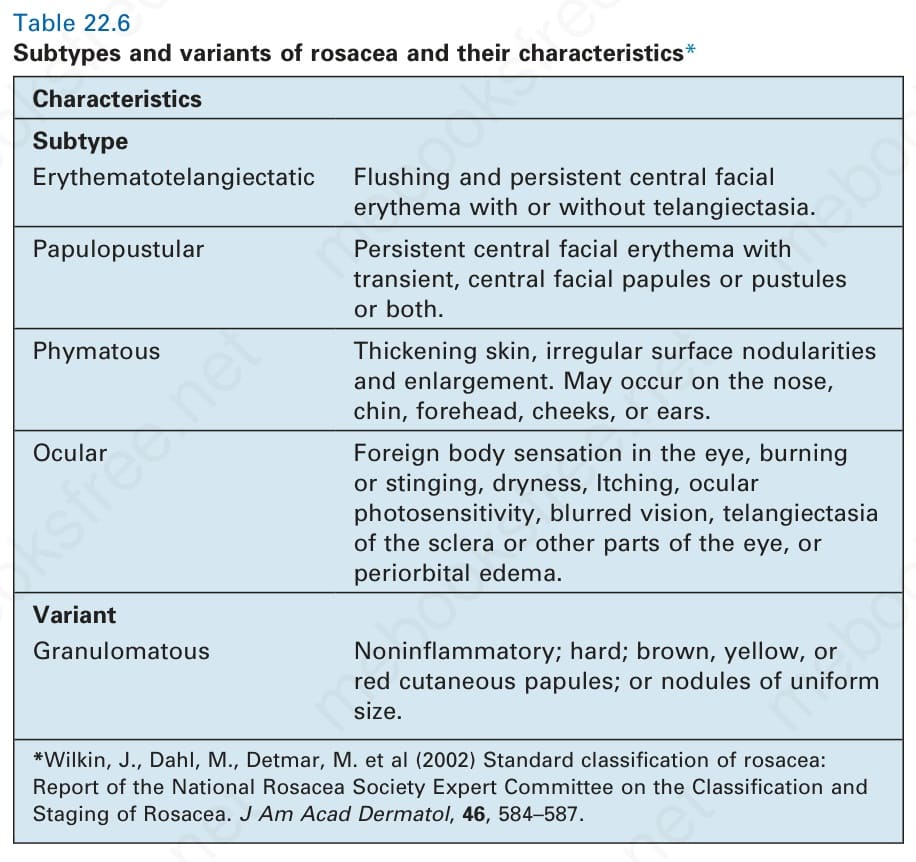
Table 22.6 Subtypes and variants of rosacea and their characteristics*
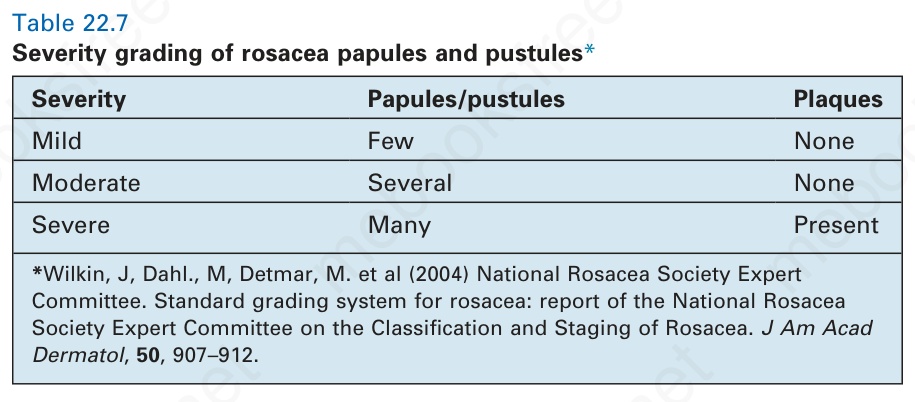
Table 22.7 Severity grading of rosacea papules and pustules*