Chloracne
Chloracne
Clinical features Chloracne (halogen acne) was first described by Herxheimer in 1899.1 It is a cutaneous manifestation of systemic poisoning by dioxin (2,3,7,8-tetra chlorodibenzo-p-dioxin) known as TCDD.2 It is characterized by follicular hyperkeratosis with the formation of open comedones in the absence of a significant inflammatory component. Exposure is usually due to accidental industrial release of chloracnegens (e.g., as the ICMESA plant explosion in Seveso, Italy in 1976; Yusho, Kyushu Island, Japan in 1968; and Yu-Cheng, Taiwan in 1979), contamination of material sprayed into the atmosphere (e.g., agent orange in Vietnam) or as a deliberate poisoning method.3–9
Drugs – in particular the progestin-only contraceptives, anticonvulsants, lithium, isoniazid, corticosteroids, ciclosporine A, and anabolic steroids – may exacerbate acne.2,17 Topical medicaments such as coal tar, hair oil (pomade acne), and mineral oil (engine oil) are also of importance (Fig. 22.192).18 Cosmetics may have a similar effect (so-called acne cosmetica).19 Cosmetics may directly promote the development of comedones but, also by virtue of chemical irritation, they can cause folliculitis with resultant pustules and papules. Hemodialysis has been associated with development of nodulocystic acne.20
The characteristic cutaneous manifestations of chloracne include open comedones (blackheads), milia, and epidermoid inclusion cysts.3,4 Lesions are predominantly found on the malar crescent, the crow’s foot region, the postauricular region, the penis, scrotum, and axillae (Fig. 22.195). Nasal involvement is characteristically absent.10 In severe cases, lesions may be more widespread (shoulders, chest, and back) and inflammatory features may be evident. The meibomian glands are typically affected (ophthalmic chloracne).11 Other cutaneous manifestations have included solar elastosis, severe xerosis, facial gray pigmentation, conjunctivitis, follicular hyperkeratosis, and erythema confined to exposed areas.10,12,8 Palmoplantar hyperhidrosis has also been described.10
Systemic involvement may present as hepatotoxicity, peripheral neuropathy, central nervous system manifestations (headache, fatigue, irritability, insomnia and impotence), chronic obstructive pulmonary disease, hypertriglyceridemia, diabetes, hypertension, cardiovascular disease, and, rarely, hepatic porphyria (porphyria cutanea tarda).10,6,13 There is a significant risk of carcinogenesis related to lymphatic/hematopoietic tissue neoplasms, breast cancer, and soft tissue sarcomas.14–17 A form of chloracne has been associated with smoking which permanently activates the AhR signaling pathway in the skin. 18,19 It has equally been reported associated to the use of sorafenib.20,21
Pathogenesis and histologic features Dioxin accumulates in the sebum leading to dysregulation of sebaceous gland homeostasis, and to apoptosis of sebocytes.2
The primary histopathological lesion in chloracne is noninflammatory and comprises follicular infundibular dilatation and plugging (hyperkeratosis) with comedone formation in association with stimulation of the outer root sheath and sebaceous duct epithelium. Inflammatory changes are minimal. Squamous metaplasia of the sebaceous glands results in milia formation and eventual epidermoid cysts with disappearance of sebaceous glands.22
The final diagnosis of chloracne should always be confirmed in serum and tissues by direct chemical analysis or a biological assay.3,23
1122 Diseases of the hair
A
B
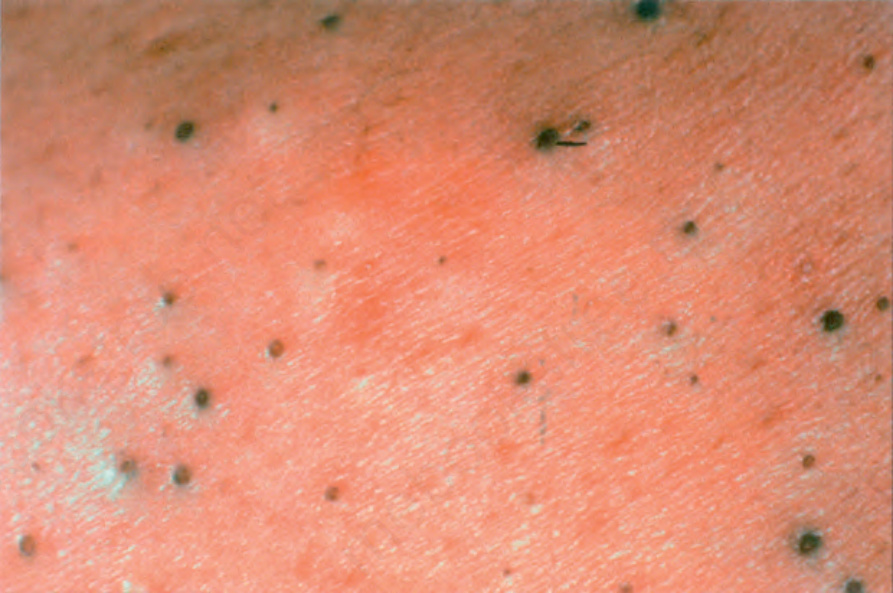
Fig. 22.192 Oil acne: these lesions follow use of hair oil or exposure to mineral oil. By courtesy of the Institute of Dermatology, London, UK.
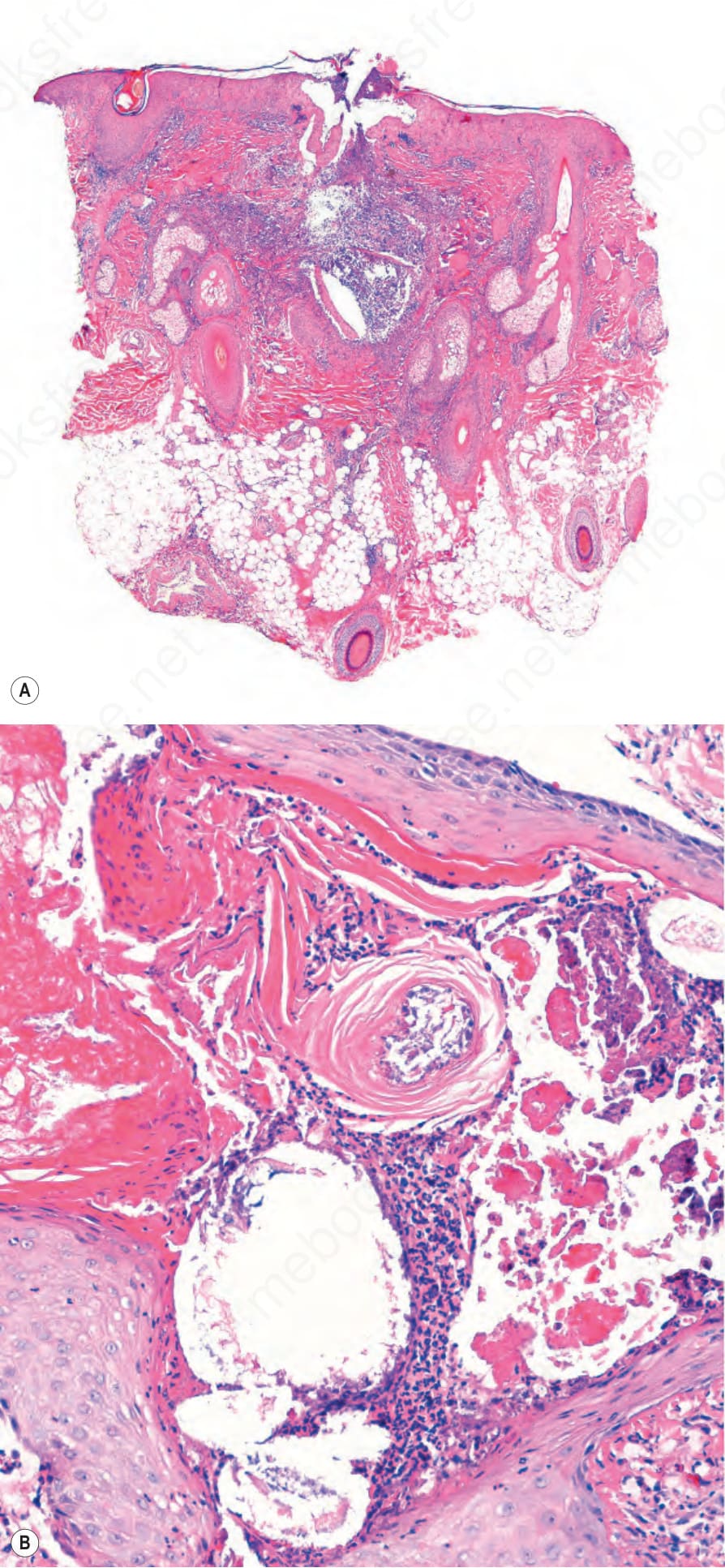
Fig. 22.193 (A, B) Acne vulgaris: rupture of a comedone releases keratin into the dermis with a resultant intense inflammatory reaction.
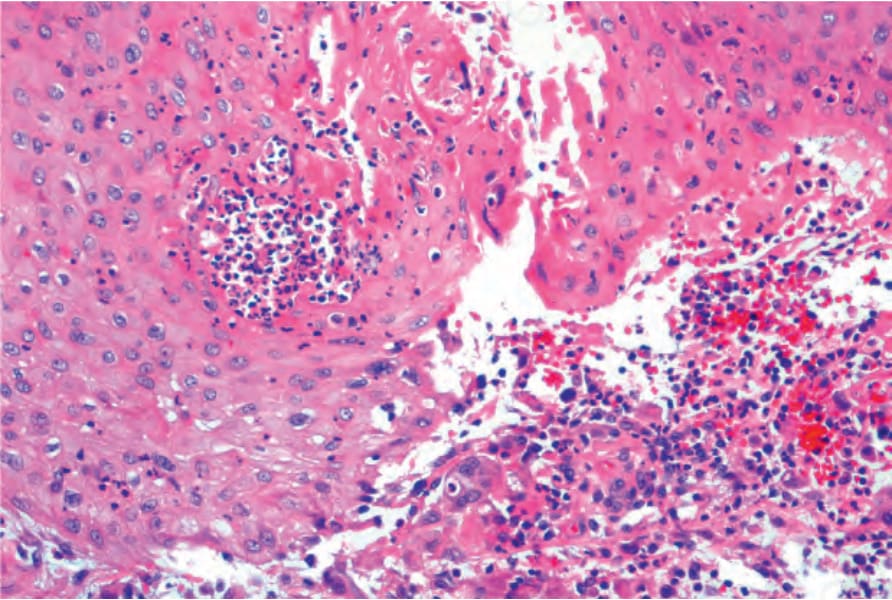
Fig. 22.194 Acne vulgaris: intense foreign body granulomatous reaction is present.
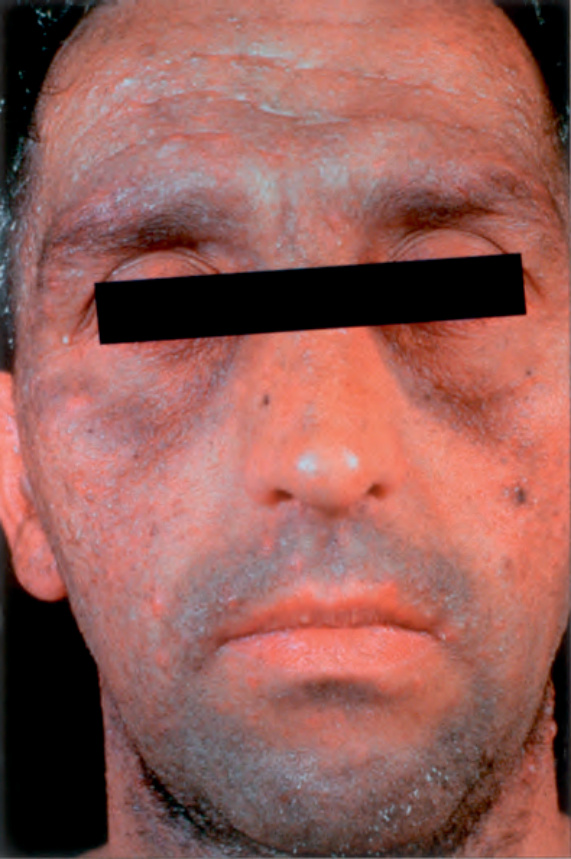
Fig. 22.195 Chloracne: there is a diffuse grayish discoloration. Comedones, milia, and cysts are present. By courtesy of the Institute of Dermatology, London, UK.