Acne vulgaris
Acne vulgaris
Clinical features Acne vulgaris is an extremely common dermatological disorder, predominantly affecting teenagers and adolescents (85%), or 15% of the general population.1,2 It shows no racial predilection and has a worldwide distribution, although clinical presentation can be different in patients with white and black skin.3–5 The sex incidence is equal, although it is often more severe in males than in females, presumably reflecting androgen levels. It is a cosmetically serious and disfiguring condition, which may be associated with considerable scarring, and often causes important psychological effects.6,7 Acne is associated with seasonal variation, worsening in winter and improving in summer.
follicular epithelium in the sebaceous gland duct and hyperkeratosis of the sebaceous duct, proliferation of P. acnes with subsequent inflammatory changes, and inflammatory and immunological responses.9–12
The process is mediated by production of IL-1α and tumor necrosis factor-alpha by keratinocytes and T lymphocytes with resultant increased proliferation of keratinocytes, diminished apoptosis, and consequent hypergranulosis.10 As a result, the sebaceous follicle becomes blocked with dense, compact keratin to form a microcomedone.
Acne vulgaris is primarily a disorder of the sebaceous follicle, and it particularly involves the face, the nose and forehead, back, and chest (Fig. 22.189).1 Sebaceous follicles have widely dilated follicular channels, fine vellus hairs, and numerous associated sebaceous glands. The distribution of the lesions of acne vulgaris reflects that of sebaceous glands and there is a close relationship between the amount of sebum produced and the severity of the disease.
Patients present with comedones (see below), which in many patients are accompanied by abscess formation, nodules, ‘cysts’, and scarring (Fig. 22.190). In the most seriously affected patients, groups of nodules joined by multiple sinuses may be present (acne conglobata). In patients of African descent and Africans, the disease is typically milder than in the white population. Postinflammatory hyperpigmentation is, however, a common problem. Nodulocystic disease is rare but, when it does occur, keloidal scarring is a significant problem (Fig. 22.191).4,5,8
Pathogenesis and histologic features The pathogenesis of acne vulgaris is complex and includes: production of androgens, excessive sebum production, abnormal desquamation of the
Acne can be classified into noninflammatory (purely comedonal) and inflammatory (mild papular, scarring papular, pustules and nodular or scarring acne). A severity grade (mild, moderate, or severe) is based on the approximate lesion count. A noninflammatory comedone is a consequence of impaired sebum secretion followed by subsequent dilatation of the follicle. Closed comedones are known as whiteheads; open comedones are called blackheads because the contents of the comedone oxidizes upon exposure to the air. Subsequent further overgrowth of P. acnes (a habitual follicular resident) results in inflammatory changes and damage to the follicular epithelium with eventual rupture and scarring.2 It is likely that hypersensitivity to P. acnes plays a role in the pathogenesis of the inflammatory response.13 This is associated with a foreign body reaction and the development of pustules, inflammatory cysts, nodules, and scarring. In addition to activating both the classic and indirect complement cascades, P. acnes also promotes neutrophil chemotaxis. Subsequent release of hydrolytic enzymes damages the follicular epithelium.2,14
1121 Chloracne
Patients in whom the clinical history or physical examination suggests hyperandrogenism should have endocrinological testing. Acne has been associated with disorders such as Alpert syndrome, polycystic ovarian syndrome, and Cushing syndrome.2,21
Early comedones show a cystically dilated hair follicle with either a narrow or a wide opening associated with infundibular hyperkeratosis (Fig. 22.193). Later, due to rupture, an acute dermal inflammatory response develops, which may be complicated by a foreign body granulomatous reaction (Fig. 22.194). In severe cases, abscesses are frequently present and cysts and sinuses often form. Dense dermal scarring (sometimes with keloidal change) is an important long-term sequel.22 Occasionally, dystrophic calcification with bone formation is a feature.23
Circulating androgens are also of importance in acne vulgaris, the development of the disease at puberty coinciding with a rise in the levels of circulating androgens.15 Androgens directly stimulate sebum secretion and also hair growth.2,16 Hypersecretion of androgens or increased 5-α-reductase (5-ARD) activity may play an etiopathogenetic role.16 It is uncertain, however, whether acne necessarily develops as a result of excess circulating androgens or because increased 5-ARD activity results in enhanced sensitivity of the pilosebaceous unit to normal levels of serum androgens. Increased androgen levels have been demonstrated in women with polycystic ovaries and in cases of adrenal hypersecretion, but increased target organ responsiveness may be responsible in some patients. Androgen receptors have been shown to be present in the nuclei of epidermal basal keratinocytes, the sebaceous glandular epithelium, the outer root sheath of hair follicles, and in the eccrine sweat glands. They are also present in the nuclei of fibroblasts, smooth muscle cells, and endothelium.16 What role they may play in the development of acne vulgaris is as yet unknown.
Differential diagnosis The granulomatous reaction may be difficult to distinguish from other granulomatous disorders, and the presence of fragments of hair or keratin may be helpful diagnostic pointers. Often, the clinical information as to the location of the lesions and the age of the patient is useful.
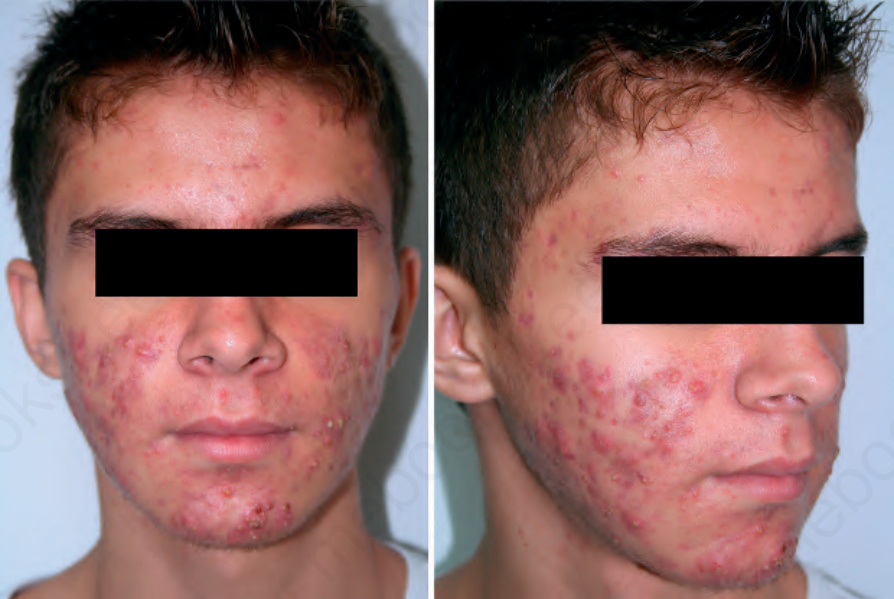
Fig. 22.189 Acne vulgaris: note the numerous papules and pustules. By courtesy of J. Cadavid, MD, Clinica Medellín, Medellín, Colombia.

Fig. 22.190 Acne vulgaris: there are prominent blackheads which develop as a result of blockage of the pilosebaceous duct by keratotic debris. By courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

Fig. 22.191 Acne vulgaris: multiple keloids have complicated areas of previous acneiform scarring. By courtesy of the Institute of Dermatology, London, UK.
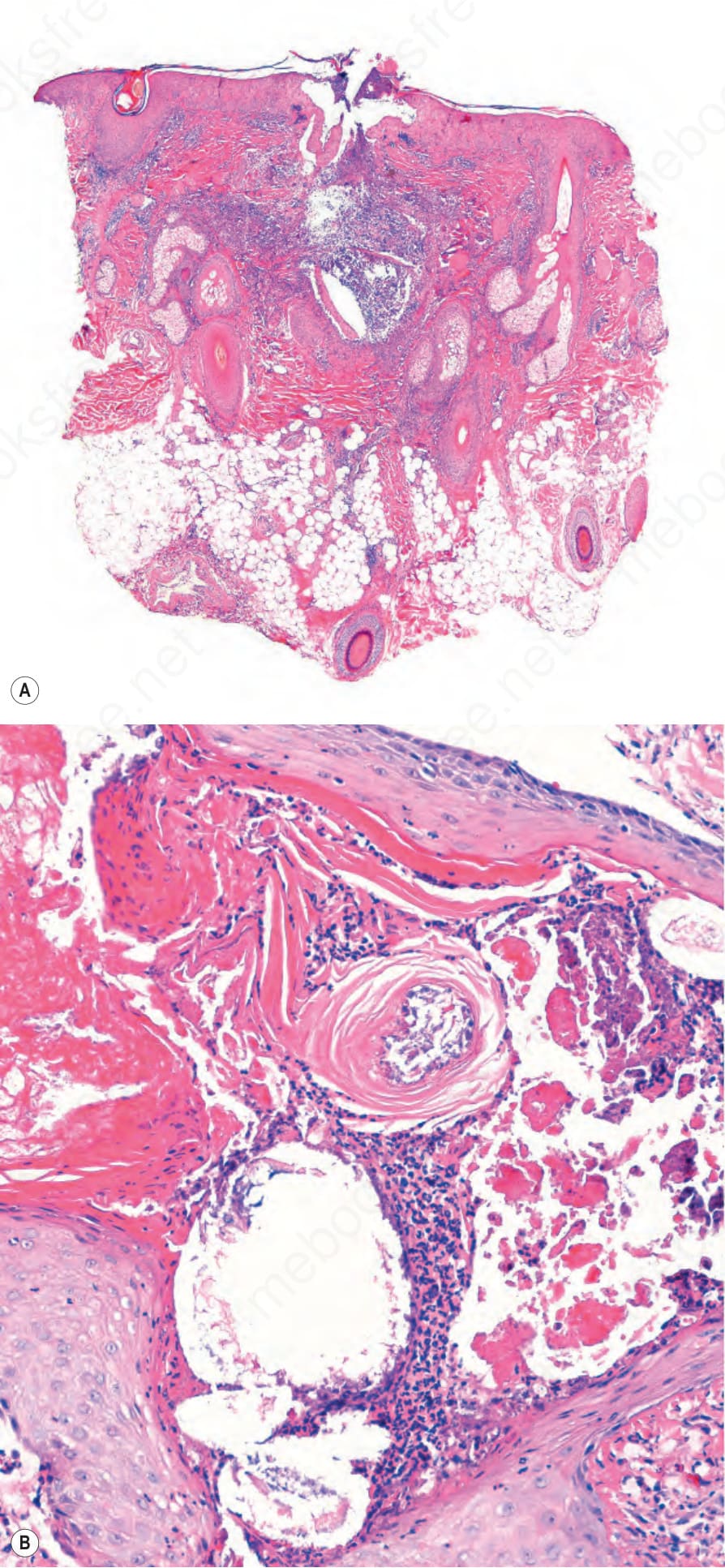
Fig. 22.193 (A, B) Acne vulgaris: rupture of a comedone releases keratin into the dermis with a resultant intense inflammatory reaction.
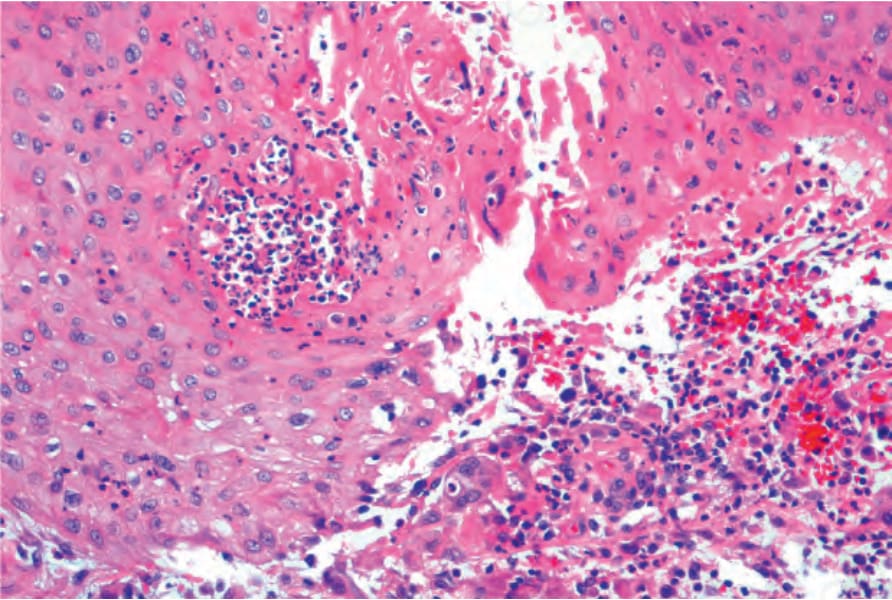
Fig. 22.194 Acne vulgaris: intense foreign body granulomatous reaction is present.