Trichonodosis (knotted hair)
Trichonodosis (knotted hair)
Clinical features Trichonodosis was first described by McCarthy.1 It is a fairly frequent incidental finding, particularly in people with curly hair.2,3 Generally, only a few hairs are affected. The knot induces weakness in the cortex and the cuticle (Fig. 22.187). One or multiple knots are seen, and as a result of trauma the hairs may break at the site of the knot. The knots are usually located on the outer third of the hair shaft.1
Two variants have been described: primary, which particularly occurs in girls with no other associated disease and sometimes affects families,4–6 and secondary, which develops as a consequence of inflammatory diseases accompanied by intense parakeratosis of the scalp such as psoriasis, seborrheic dermatitis, or pityriasis capitis.7,8
Pathogenesis and histologic features A significant number of patients with the primary variant wear their hair in ponytails or pigtails.6 Repeated traction of the scalp or mild trichotillomania may lead to hair casts.9
Trichonodosis may also be observed in pubic hair and other areas of the body, and a variant with multiple large knots has been documented.4 The condition has been described in association with zinc deficiency and trichoschisis.1,5
In the secondary variant, the hair casts are composed of parakeratotic debris derived from the external root sheath and most probably originating in the follicular infundibulum and external root sheath.10
A number of transmission and scanning electron microscopic studies have shown that the typical cast is composed of two concentric layers of keratinized cells: the internal layer originates from Huxley layer while the outer derives from Henle layer.11 Other studies, however, have shown three layers: two emerging from the internal root sheath and an external layer originating from the external root sheath.10 Energy dispersive X-ray microanalysis has shown that the casts contain silica, aluminum, and molybdenum.6
The histologic appearance is quite characteristic. The material surrounds and adheres to the cuticle without affecting the hair structure (Fig. 22.188).
1120 Diseases of the hair
Differential diagnosis
The differential diagnoses include pediculosis capitis, tinea alba, trichorrhexis nodosa, and deposits of extraneous material.12,13 Hair casts may be distinguished since peripilar casts are circumferential rather than eccentric matter and can be easily moved up and down the hair shaft. Hair casts stain blue with toluidine blue due to the presence of the internal root sheath.14

Fig. 22.187 Trichonodosis: the knots are readily seen by light microscopy.
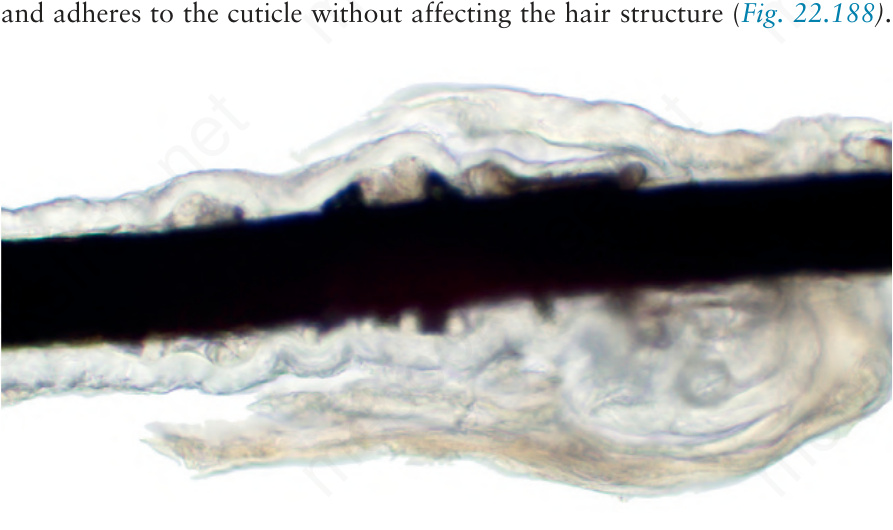
Fig. 22.188 Hair casts: amorphous material surrounds the hair shaft. Courtesy of J.C. Garcés, MD, Hospital Luis Vernaza, Guayaquil, Ecuador.