Trichorrhexis nodosa
Trichorrhexis nodosa
Clinical features Trichorrhexis nodosa is the most common hair shaft defect. It is mainly found in patients who complain of fragile and easily breakable hair, and it is not a specific disease. The defect arises from trauma imposed on the hair shaft either congenitally or by acquired disorders. The genetic type is related to genodermatoses and metabolic disorders and the traumatic type to damage by mechanical and chemical trauma.1
The condition presents with beaded thickening of the proximal or distal end of the hair shaft. These changes resemble minute spheres or dust particles adherent to the hair shaft and represent fractures (Fig. 22.171).2
Disease Affected gene Role of encoded protein Hair phenotype
Monilethrix hHb6 or hHb Hair keratin (structure protein) Thin fragile hair with a beaded appearance under light microscope
Netherton’s syndrome SPINK5 Serine protease inhibitor LEK1 Defective hair shart differentiation (‘bamboo hair’)
Generalized atrichia with papular lesions Hairless (HR) Putative transcription factor Failure of first postnatal hair growth cycle
Human nude WHN Transcription factor Hair shafts fail to emerge from skin
X-linked hypohidrotic ectodermal dysplasia Ectodysplasin (EDN) Intercellular signaline molecule Sparse hair
Autosomal hypohidrotic ectodermal dysplasia Ectodysplasin receptor (EDN)
Ectodermal dysplasia/familial incontinentia pigmenti
Receptor for ectodysplasin Sparse hair
IKK-gamma (NEMO) Kinase required for activation of the transcription factor NF-kB
Sparse hair
Naxos disease Plakoglobin Adhesion molecule Woolly hair
Ectodermal dysplasia/skin fragility syndrome Plakoglobin 1 Desmosomal adhesion molecule Sparse hair
Menke’s disease ATP7a Copper-transporting P-type ATPase Hair loss; abnormal hair texture
Tricho-rhino-phalangeal syndrome type I TRPS I Zinc finger protein, putative transcription factor
Sparse and unruly scalp hair
X-linked dominant chondrodysplasia puntata EBP Δ(8), Δ(7) sterol isomerase emopamil-binding protein
Coarse hair, alopecia
Giant axonal neuropathy Gigaxonin (GAN) Unknown Curly or kinky hairs
*Cheng, A.S., Bayliss, S.J. (2008). The genetics of hair shaft disorders. J Am Acad Dermatol, 59, 1–22.
Trichorrhexis invaginata
Tapered fracture Trichorrhexis nodosa Trichoptilosis Monilethrix
1111 Fractures of the hair shaft
Trichoclasis Trichoschisis Peripilar cast Trichonodosis
Pili torti Pili multigemini Pili multi-bifurcati Pili bi-bifurcati
Pili bifurcati
The distal form of the condition is very common and often results from general weathering of the hair. It presents in all races, especially in people with long hair.
There are two types of proximal trichorrhexis nodosa: one variant is restricted to patients of African heritage and presents as plaques of alopecia on the scalp, moustache, beard area, or pubis. It is generally associated with other wear-and-tear changes such as split ends (trichoptilosis).
The second variant is much less frequent and includes congenital and hereditary defects of the hair shaft, the most important of which is TTD (see below). The abnormal hair in these patients, which is highly susceptible to daily wear and mild trauma, fractures easily. Other abnormalities of the hair shaft are also commonly present. The hair breaks so easily that even people with short hair develop areas of alopecia. Trichorrhexis nodosa has been associated with ectodermal defects and multiple genetic syndromes including Netherton, Basex-Dupré-Christol, Menkes, Kabuki, and Tay syndromes. Metabolic disorders associated with trichorrhexis nodosa are anomalies of the urea cycle such as argininosuccinic aciduria and citrullinemia. Other reported metabolic disorders are acquired deficiencies or congenital deficiencies in biotin and zinc metabolism. Trichorrhexis nodosa has also been associated with many other conditions including untreatable infant diarrhea, tricho-hepato-enteric syndrome, mitochondrial diseases, trichorrhexis invaginata, monilethrix, pseudomonilethrix, pili torti, pili annulati, ectodermal dysplasia, giant axonal neuropathy, hypothyroidism, adrenoleukodystrophy, improper use of ceramic flat irons, combing habits, hair transplantation, and after tumor necrosis factor-α inhibitor therapy.3–22
Box 22.2 Hair shaft diseases
Fractures of the hair shaft Trichorrhexis nodosa Trichothiodystrophy Trichoschisis and trichoclasis Trichorrhexis invaginata Tapered fracture Trichoptilosis
Irregularities of the hair shaft Uncombable hair syndrome Pili bifurcati Pili multigemini Trichostasis spinulosa Pili annulati Monilethrix Bubble hair
Hair shaft coiling and twisting Pili torti Woolly hair Acquired progressive kinking of the hair Trichonodosis Circled and rolled hair
Extraneous matter on the hair shaft Hair casts
Pathogenesis and histologic features Microscopic study shows a normal hair shaft except for the beaded areas where the cortex has herniated through the cuticular cells (see Fig. 22.1). The latter are fragmented and in many cases totally absent. In specimens with good preservation, where the hair has not broken up completely, the appearances are reminiscent of two worn-out paintbrushes joined by their hairs (Figs 22.172 and 22.173).23,24
Differential diagnosis Hair shaft fractures may be seen in a variety of other conditions including trichoschisis, trichoclasis, trichorrhexis invaginata, tapered fracture, and trichoptilosis. Extensive clinical and laboratory studies are often required to establish the correct diagnosis. Distal forms can simulate dandruff, peripilar casts, and pediculosis. The differential diagnosis in these cases can be easily made by microscopic examination of the hair.
1112 Diseases of the hair
neutropenia, and mental retardation) and Tay (ichthyosiform erythroderma, hair shaft abnormalities, mental and physical retardation) Sabinas, and Pollitt syndromes.3–7
Sporadic cases of patients with TTD without any associated neuroectodermal defects have also been documented.8,9 The condition may also present with urological malformations and primary hypercalciuria, sideroblastic anemia, hypereosinophilic syndrome, congenital heart disease, and beta-thalassemia.10–14
Pathogenesis and histologic features Patients with TTD and photosensitivity have a defect in the DNA nucleotide excision repair (NER) mechanism. The NER pathway involves at least 28 genes and is linked to DNA repair and transcription.15,16 Three NER genes are part of the basal transcription factor, TFIIH.
Three autosomal recessive syndromes are associated with NER defects: the photosensitive form of TTD, xeroderma pigmentosum (XP), and Cockayne syndrome. TTD results from mutation in the XPB, XPD, or TTD-A genes. These three genes encode for proteins that are part of the basal transcriptor factor TFIIH, including XPB and XPD, helicases that excise and repair DNA.
It is thought that the clinical features of XP are linked to mutations in the repair function of NER genes, while mutations affecting the transcription-related function of NER genes result in the TTD phenotype. Patients with TTD do not have an increased risk in cancer susceptibility, as seen in XP patients (1000-fold increase risk).17,18
The diagnosis of TTD can be confirmed by demonstrating DNA repair defects after exposure to ultraviolet light. Abnormalities in excision repair of ultraviolet-damaged DNA are recognized in about half of the patients.
The hair of patients with TTD, which shows loss of sulfur bonds, is characterized by a significant decrease in the concentration of cystine.19 The sulfur and cystine content of the hair is reduced in the order of 50%.3 The cuticular cells become weak, fracturing readily with formation of trichorrhectic nodules (Fig. 22.174).20 The hair shafts appear flattened, with trichoschisis and absence or deficiency of the cuticle.21,22 Examination with polarized light is essential to visualize the typical alternating dark and light band pattern resulting from the undulation of cortical pilar fibers. The appearance resembles a tiger’s tail (Fig. 22.175).23,24
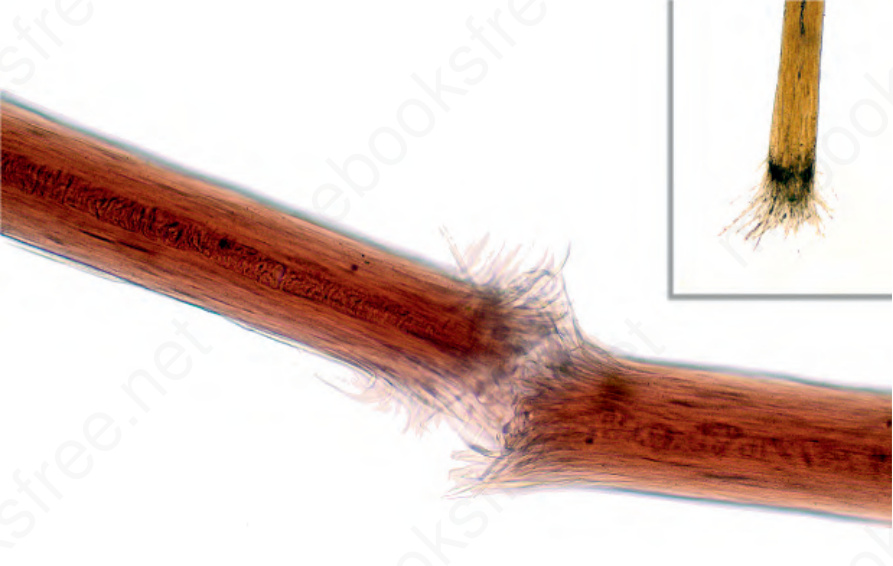
Fig. 22.1 Hair shaft sample. Trichorrhexis nodosa. The sample must not be taken using pull traction but rather by cutting it proximally. Otherwise, the sample will only show the distal end as shown in the upper right-hand corner. Courtesy of J.C. Garcés, MD, Hospital Luis Vernaza, Guayaquil, Ecuador.

Fig. 22.170 Hair shaft defects.

Fig. 22.171 Trichorrhexis nodosa: example from a localized form. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
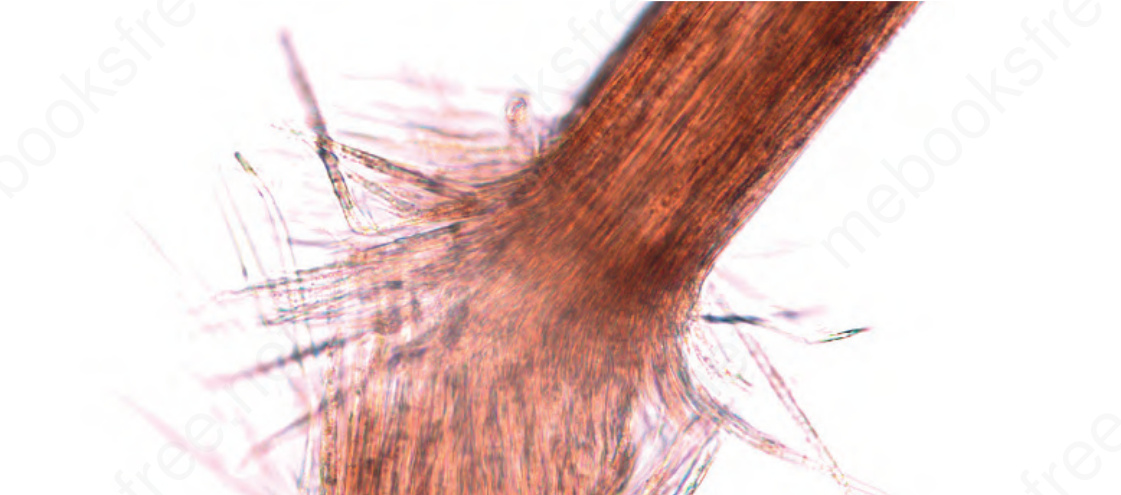
Fig. 22.172 Trichorrhexis nodosa: typical node as a result of fracture of cortical fibers protruding through a broken cuticle.
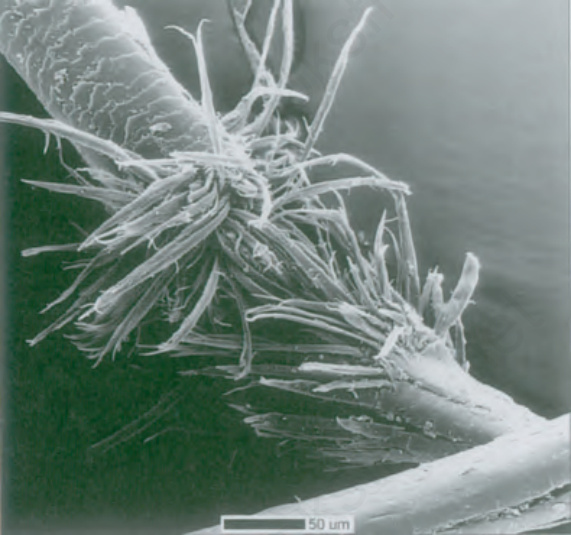
Fig. 22.173 Trichorrhexis nodosa: the features are likened to dried paintbrushes joined by their hair. The condition is commonly the result of trauma. Reproduced with permission from Hordinsky, M.E., Sawaya, M.E., Scher, R.K. (eds) (2000) Atlas of hair and nails. Philadelphia: Saunders.

Fig. 22.174 Trichothiodystrophy: note the sparse, short, and fragmented hairs. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
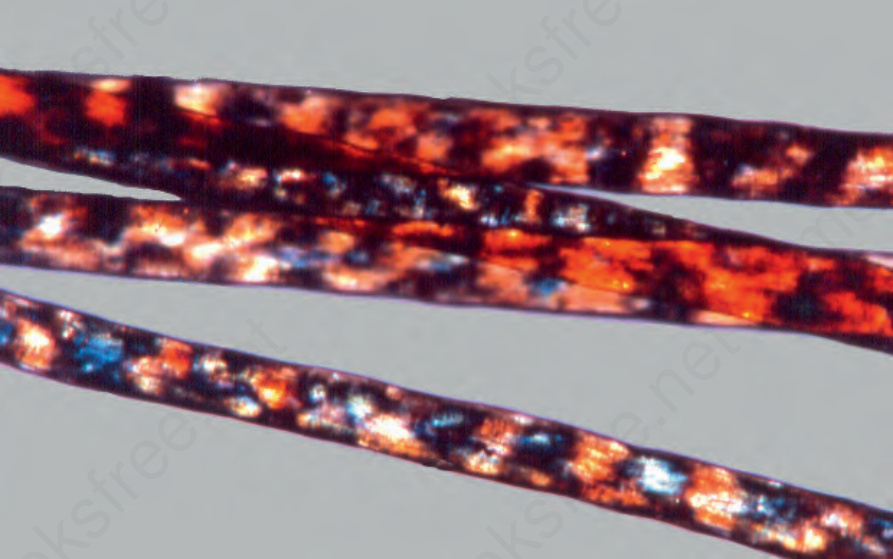
Fig. 22.175 Trichothiodystrophy: typical tiger tail appearance in hair shafts under polarized light. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
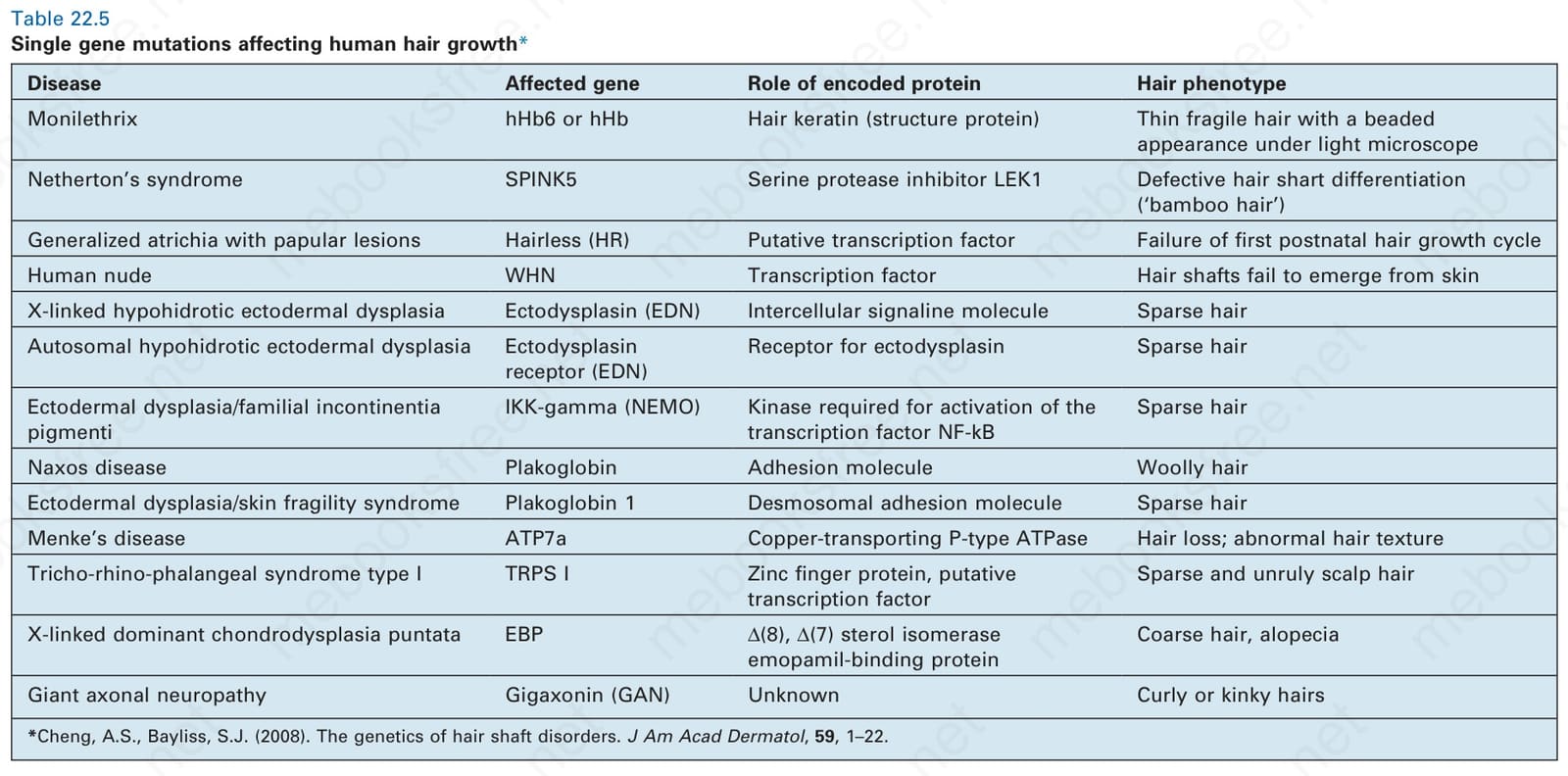
Table 22.5 Single gene mutations affecting human hair growth*