Erosive pustular dermatosis
Erosive pustular dermatosis
Clinical features Erosive pustular dermatosis of the scalp was first described by Pye in 1979 as a chronic, noninfectious dermatosis principally affecting elderly women, and there is a frequent history of trauma to the scalp.1–3 Some cases outside the scalp have been reported, particularly on the legs and in areas of cutaneous atrophy and venous insufficiency.4–7 Isolated cases affecting the mucosal surfaces and in a child with Klippel-Feil syndrome have also been described. 8,9 Associations described include exogenous factors such as contusions, erosions, solar burns, perinatal scalp injury, cochlear implant, surgery, after skin grafts, hair transplant, radiation, synthetic fiber implantations, cryotherapy, CO2 laser treatment, and photodynamic therapy.2,10–26 Trauma may antedate the disease by days or years.2 The disease may also develop after herpes zoster. Its onset after treatment with topical, imiquimod, latanoprost, imiquimod, gefitinib, minoxidil, tacrolimus, and ingenol mebutate has also been described. Association with systemic diseases associated include rheumatoid arthritis, myasthenia gravis, and myelodysplastic syndrome.27–36 It has also been associated with basal cell carcinoma.37
A nonscarring pruritic superficial variant predominantly affecting the scalp may also be encountered (acne necrotica miliaris).1
Pathogenesis and histologic features Both S. aureus and Propionibacterium acnes have been implicated in the etiology of acne necrotica, and at least a subset of patients respond to antibiotic therapy.3–7 However, the latter response may well be the result of the anti-inflammatory action of antibiotics. Stress and manipulation have also been suggested as possible factors as have rosacea and seborrheic dermatitis.1,6,8
Early lesions are characterized by dermal edema and a superficial to mid-dermal perivascular and perifollicular lymphocytic infiltrate associated with spongiosis and apoptosis of the external root sheath, adjacent epidermis, and sebaceous gland.1 Eosinophils may also be present but neutrophils are not a feature. With progression, there is necrosis of the whole follicle and overlying epidermis (Fig. 22.168). A neutrophil-rich crust overlies the lesion and bacterial colonies may be prominent.1 Granulomatous inflammation is not a feature.1 Chronic lesions are characterized by loss of follicles and vertically oriented dermal scars.3
Differential diagnosis Differential diagnosis includes neurotic excoriations, eczema herpeticum, and conventional folliculitis. Lesions in neurotic excoriations are superficial and are not limited to the anterior part of the scalp. Eczema herpeticum may be differentiated with a biopsy or a Tzank test which will show the characteristic viral inclusions.5 Early varioliform necrotic acne may be
Early lesions are asymptomatic and edematous, with well-defined borders characterized by a scaly scab that upon removal leaves a lesion with pustules (Fig. 22.169). Late lesions develop scarring alopecia. There may be secondary bacterial or fungal colonization.2
Pathogenesis and histologic features The pathogenesis is unknown. Due to the high incidence in elderly patients, there has been speculation as to the role that chronic actinic damage, immunosuppression, and autoimmune disease may have in the pathogenesis of the disease.2,38 Laboratory data and bacteriological and mycological investigations are usually non-contributory.39
The histopathological picture is not specific.40 Erosion of the superficial epidermis with acanthosis, focal atrophy, parakeratosis, and subcorneal pustules is seen. In the dermis, there is a mixed inflammatory cell infiltrate composed of lymphocytes, neutrophils, and some giant cells. The hair follicles are progressively affected and disappear.41
1110 Diseases of the hair
Differential diagnosis The differential diagnosis is wide and includes many suppurative nonmicrobial diseases such as amicrobial pustulosis associated with autoimmune disease, pustular ulcerative dermatosis of the scalp, inflammatory tinea capitis (kerion celsi), folliculitis decalvans, sterile eosinophilic pustulosis of Ofuji, pustular psoriasis vulgaris, dissecting cellulitis, pemphigus vulgaris, mucous membrane pemphigoid, gangrenous pyoderma, bacterial folliculitis, and ischemic diseases such as temporal arteritis.42 From this list, only the first three will be discussed.
features with erosive pustular dermatosis.43–45 Pustular ulcerative dermatosis of the scalp affects mainly young men of African origin with severe malnutrition.46 Inflammatory tinea capitis may closely simulate an erosive pustular dermatosis of the scalp, requiring a direct scrape for KOH and culture. PAS or silver stains are also useful to confirm the diagnosis.47,48
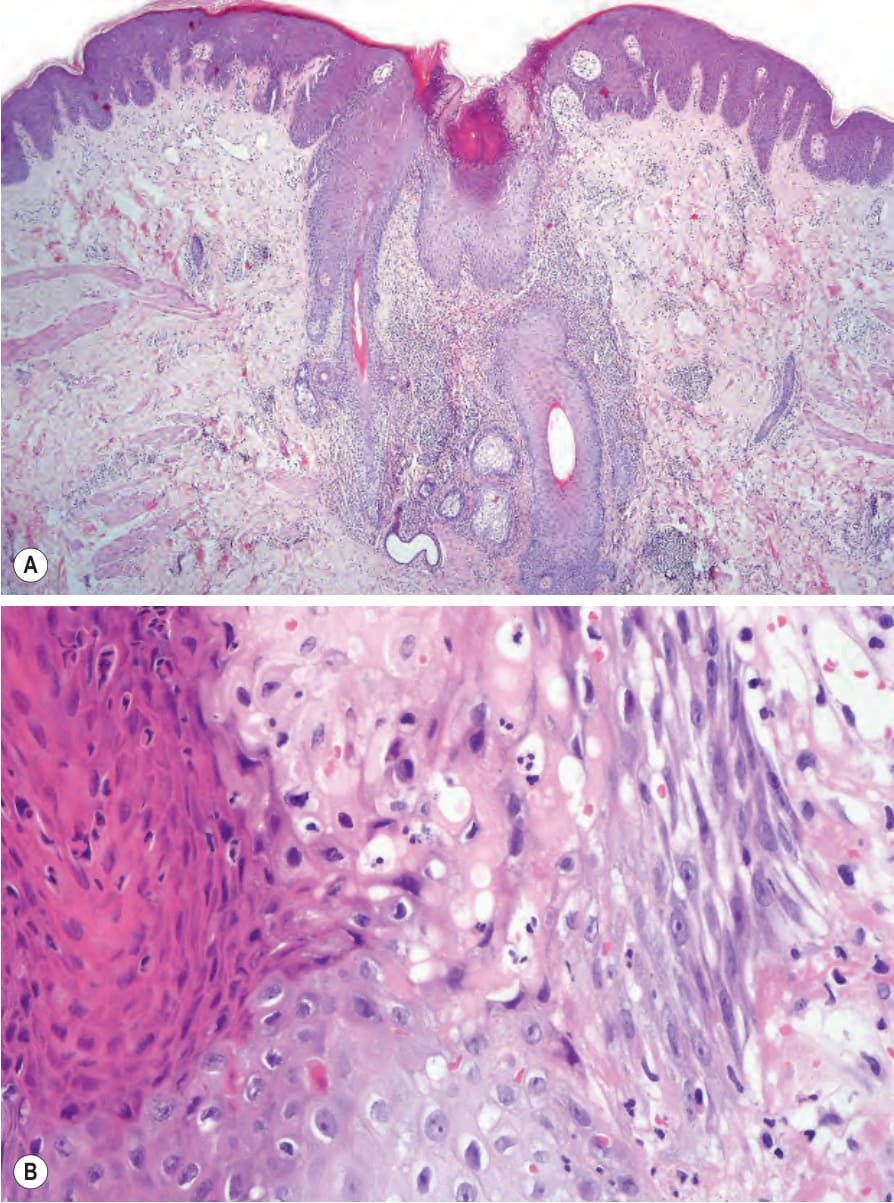
Fig. 22.168 (A, B) Acne necrotica. Note necrosis of the hair follicle.
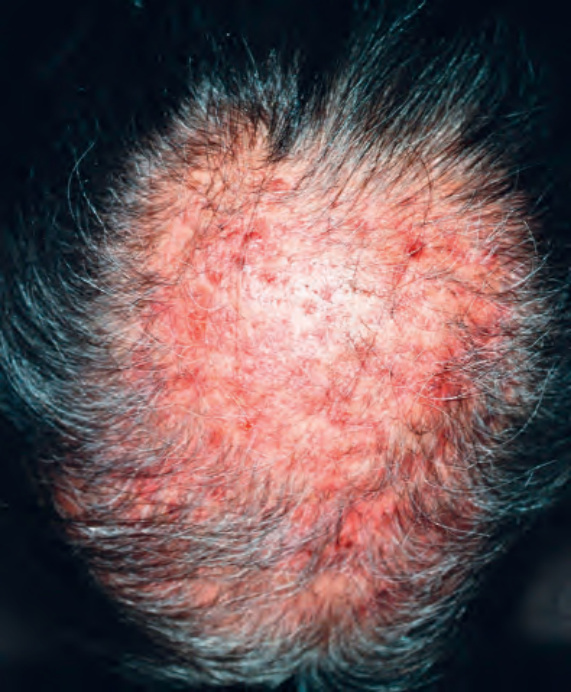
Fig. 22.169 Erosive pustular dermatosis: note the eroded and edematous appearance as a consequence of surgery. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.