Acne keloidalis nuchae
Acne keloidalis nuchae
Clinical features Acne keloidalis nuchae (folliculitis keloidalis nuchae) is the commonest form of scarring alopecia occurring in African males. It involves the nape of the neck, with a 20 : 1 male-to-female predominance.1–3
The denomination acne keloidalis is incorrect as the disease is not associated with acne lesions, or keloidal collagen in the histologic study.4
Differential diagnosis The differential diagnosis of dissecting cellulitis includes folliculitis decalvans, aseptic nodules of the scalp (pseudocyst of the scalp), and infectious processes.
The fluctuating suppurative nodules with fistulous tracts typical of dissecting cellulitis are not a feature of folliculitis decalvans. Histologically, the latter condition is characterized by a neutrophilic inflammatory infiltrate predominantly affecting the upper part of the hair follicle, and a lymphocytic infiltrate with focal foreign body granulomata to hair shafts. The aseptic nodule of the scalp consists of a solitary nodular lesion that drains purulent material leaving a cystic cavity. Contrary to dissecting cellulitis, the alopecia is reversible and the prognosis excellent.22,33,34
The disease begins as localized follicular papules that progressively increase in size and become confluent, forming keloidal plaques with subsequent loss of hair (Fig. 22.164). It has also been described in women of African and Latin American heritage and has been associated with keratosis follicularis spinulosa decalvans, tufted hair folliculitis, acanthosis nigricans, renal transplant patients on tacrolimus and sirolimus, ciclosporine A (in both white and African-heritage patients), lithium carbonate, antiepileptic medications, and the use of football helmets.5–17
Pathogenesis and histologic features The cause is unknown. It most probably reflects a response to a local irritative phenomenon complicated by secondary bacterial infection.18 Curly hairs that have been cut too short and grow back into the skin, inducing an inflammatory reaction, are thought to represent a likely cause. Although this same phenomenon has been postulated in the pathogenesis of pseudofolliculitis barbae there is no relationship between the two diseases.1,19 It
1108 Diseases of the hair
has also been considered a disorder of transepidermal elimination.1,20 Associations include high levels of testosterone, seborrheic dermatitis, and an increased density of mast cells in the nape of the neck.21
The best way to evaluate acne keloidalis is with vertical sections (Fig. 22.165). Histologically, the initial lesion is similar to that of folliculitis decalvans with a neutrophilic infiltrate in the isthmus and around sebaceous glands which eventually disappear. The infundibulum is dilated. Later, there are thick bands of compact collagen admixed with a variable lymphoplasmacytic inflammatory cell infiltrate centered mainly on the follicular infundibulum and isthmus (Fig. 22.166). As previously mentioned, true keloidal collagen is not observed.22 There is associated thinning of the external root sheath with lamellar fibroplasia (see Fig. 22.120), and eventually follicular destruction results in free hair shafts within the dermis where they elicit an intense inflammatory cell reaction (Fig. 22.167).23 Abscesses and fistulous tracts similar to those observed in dissecting cellulitis may sometimes be encountered. The hair follicles lose their sebaceous glands, and multiple follicles may fuse together to form a single follicular ostium containing multiple hair shafts (polytrichia).24
Differential diagnosis Central centrifugal scarring alopecia represents the main differential diagnosis. Although the clinical presentation and sites of involvement are very different, there is considerable histologic overlap. A case of tinea capitis mimicking acne keloidalis has also been reported in a female patient.25,26
Biopsies of clinically normal skin from the vicinity of abnormal lesions may show evidence of follicular destruction and fibrosis.23
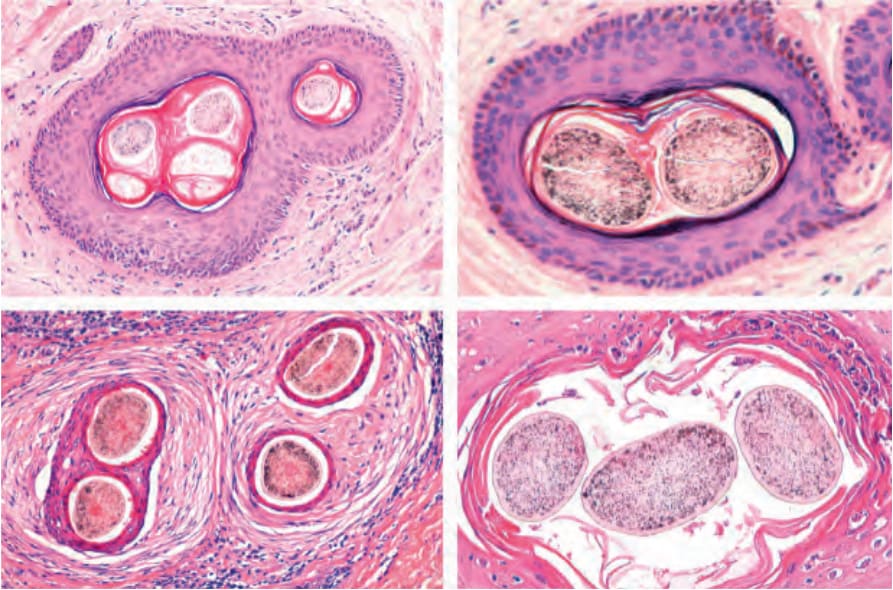
Fig. 22.120 Compound follicles. Upper panel, compound normal follicles transversally cut at the level of the infundibulum. Note the granular cell layer and discrete perifollicular fibrotic layer and minimal lymphocytic infiltrate. Lower panel, compound follicles in scarring alopecia. Horizontal sections at the level of the isthmus. There is extensive perifollicular fibrosis and an inflammatory infiltrate. The follicles on the left lower panel are from a case of acne keloidalis nuchae and those on the right panel from a case of folliculitis decalvans.

Fig. 22.164 Acne keloidales nuchae: papules have coalesced forming a keloidal plaque. Pustules are also seen. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.

Fig. 22.165 Acne keloidales nuchae: surgical specimen showing intense fibrosis of the dermis with distortion of the orientation of the hair follicles. The epidermal surface shows some tufted follicles.
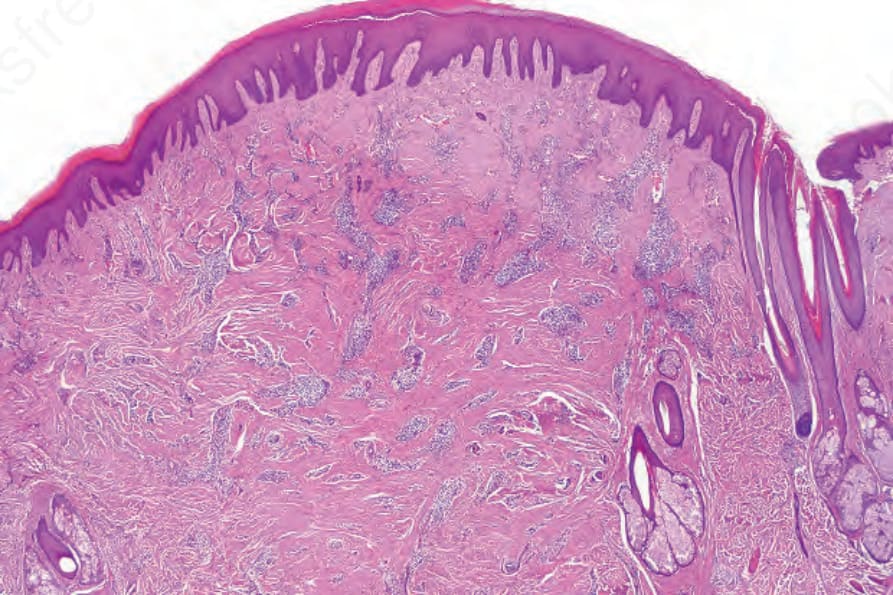
Fig. 22.166 Acne keloidales nuchae: scanning magnification showing dermal scarring and multiple free hair shaft fragments.
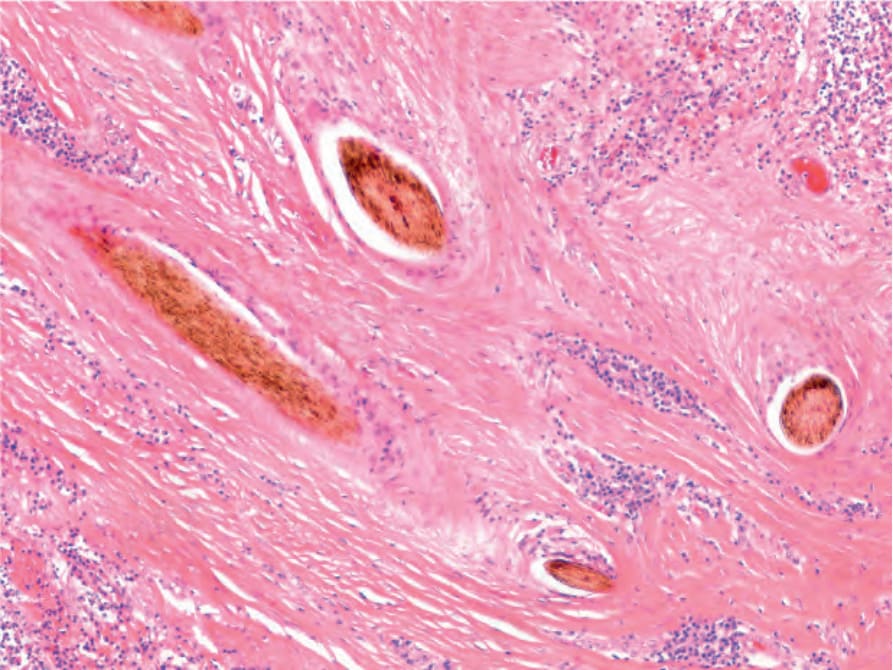
Fig. 22.167 Acne keloidales nuchae: high-power view of hair shaft fragments surrounded by dense fibrosis.