Folliculitis decalvans
Folliculitis decalvans
Clinical features Quinquaud originally described folliculitis decalvans in 1888.1 It is presently considered a form of scarring alopecia with a prominent inflammatory component characterized by pustules at the periphery of the lesions, perifollicular erythema, and follicular tufting (Figs 22.157 and 22.158). In its initial phase it is very symptomatic with pain, pruritus, and a burning sensation in the scalp. It is more frequent in young and middle-aged adult men. Occipital and vertex areas are the main areas affected.2–4 Bad prognostic factors include early onset of the disease before 25 years of age and presence of pustules within the patch of alopecia.5
Folliculitis decalvans may involve the beard area (lupoid sycosis), the face, and the nape of the neck.6 It has been associated with Darier disease, human T-cell lymphotropic virus type I-associated myelopathy/tropical spastic paraparesis, squamous cell carcinoma, and micronychia. It also has
Pathogenesis and histologic features The pathogenesis of folliculitis decalvans is unknown. Although Staphylococcus aureus can be isolated in the majority of the patients it is thought that the pustules are the result of secondary bacterial colonization and not the cause of the illness. In nonpustular areas, the clinical picture is very similar to that of central centrifugal cicatricial alopecia. An immunity defect based on genetics and race has been considered.3,16 In early lesions, an infiltration of activated T-helper cells has been observed. Infiltration by neutrophils and fibrosis can be explained as the result of secretion of IL-8 and intercellular adhesion molecule (ICAM)-1 in the acute phase, and by basic fibroblast growth factor (B-FGF) and TGF-beta in the late phase, respectively.17
Biopsy should be taken of an active lesion for conventional histologic study and direct immunofluorescence. Vertical or horizontal sections may
1106 Diseases of the hair
Differential diagnosis The differential diagnosis of folliculitis decalvans includes perifolliculitis capitis abscendens et suffodiens and infectious processes. Perifolliculitis capitis abscedens et suffodiens is characterized by sinus tracts lined by squamous epithelium. Bacterial or fungal folliculitis have to be excluded by the use of cultures and special stains.18,19
As previously mentioned, end-stage lesions may be impossible to differentiate from a central centrifugal cicatricial alopecia or classic pseudopélade of Brocq.20,21

Fig. 22.157 Folliculitis decalvans: this patient shows tufted folliculitis. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
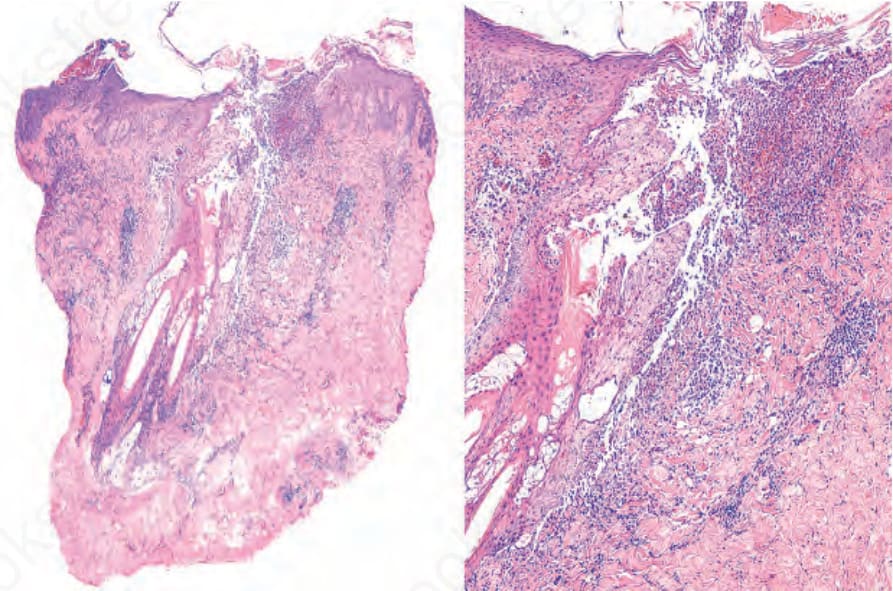
Fig. 22.159 Folliculitis decalvans: in this composite image, there is a superficial squamous crust containing neutrophils surrounding the opening of some hair follicles. In the dermis there is fusion of hair follicles (right).

Fig. 22.161 Dissecting cellulitis of the scalp: there are nodules and sinuses with suppuration, and scarring alopecia. Courtesy of E.Peña, MD, Clínica Medellín. Medellín, Colombia.