Pseudopélade of Brocq
Pseudopélade of Brocq
Clinical features In 1885, Brocq described a form of progressive, idiopathic, noninflammatory scarring alopecia, which he named pseudopélade.1 This is a very controversial entity that has been the subject of heated debate for more than 100 years.2 At present, many of the cases described as pseudopélade are considered to represent final stages of diverse scarring alopecias including discoid lupus erythematosus, lichen planopilaris, and central centrifugal scarring alopecia.3,4 The term pseudopélade of Brocq should be restricted to those patients in whom exhaustive clinical and histologic examination and pertinent laboratory tests have excluded all other forms of scarring alopecia.5,6
Clinical features Graham-Little syndrome The clinical triad of scarring alopecia of the scalp, noncicatricial alopecia of pubic and axillary hair, and the development of keratosis pilaris on multiple hairy areas was originally described in 1914 by Piccardi and in 1915 by Graham-Little in two patients, one of them studied by Lassueur (Lassueur -Graham-Little-Piccardi syndrome).1–3 The disease is very rare and presents more frequently in middle-aged women, and the scarring alopecia frequently precedes the other components of the syndrome by months to years.4,5
Graham-Little syndrome has been associated with classic lichen planus, frontal fibrosing alopecia, erosive lichen planus, complete androgen insensitivity syndrome (testicular feminization syndrome), hepatitis B vaccination, and HLA-DR1 type in a mother and her daughter.3,6–11
Patients are generally white adult females with no previous symptoms who present with discrete asymptomatic areas of alopecia. These vary in shape and location and tend not to involve the peripheral hairline region of the scalp (Fig. 22.147). Lesions progress slowly with alternating periods of inactivity and exacerbation. When the disease stabilizes, confluent plaques of alopecia with a shiny white porcelain-like surface are seen (Fig. 22.148). There is loss of follicular ostia but a few follicles sometimes survive within the plaque. Mild erythema may be detected but in general there is little or no inflammation. Some lesions are hypopigmented and even depressed. Frequently, they are irregular and have a geometric form. Such foci have been classically described as ‘footprints in the snow’, implying that the atrophy is visualized as a focal depression within the plaque.7 However, many cases of pseudopélade of Brocq do not show atrophy or the ‘footprints in the snow’ sign.8 No cases involving individuals of black African descent have been reported so far in the literature.
Pathogenesis and histologic features The etiology is unknown. Recently, an autoimmune response against the INCENP centromere protein has been reported. 12 Graham-Little syndrome has usually been considered a variant of lichen planopilaris. However the clinical features differ from ordinary lichen planopilaris and the microscopic appearance is variable, including the presence of a lichenoid tissue reaction and follicular hyperkeratosis (Fig. 22.146).13
Differential diagnosis The most important differential diagnosis is keratosis follicularis spinulosa decalvans. However, the clinical picture of the latter is distinctly different. Keratosis follicularis is frequently familial, starting in infancy and
The diagnosis of pseudopélade is one of exclusion since an identical clinical and histologic picture may be seen in the end stages of other forms of scarring alopecia. In general, inflammation is minimal and, if prominent, the disease is most unlikely to represent pseudopélade.9 Cases particularly affecting the crown or vertex that are thought to represent pseudopélade are probably best classified as central centrifugal scarring alopecia.
Although pseudopélade classically affects the scalp, a case with concomitant involvement of the beard area has been documented.10 While the
1102 Diseases of the hair
Many conditions progress to scarring alopecia with irreversible loss of hair follicles as a final event. The minimal inflammatory cell infiltrate which is present in pseudopélade is particularly located around the follicular bulge. This is believed to lead to irreversible damage to the hair follicle with eventual complete destruction and subsequent scarring (Fig. 22.149).18
As mentioned above, a histologic diagnosis of pseudopélade of Brocq is one of exclusion. No pathognomonic pathological features of pseudopélade have been described, and an accurate diagnosis depends on an adequate biopsy.19 The best specimens are those taken from the periphery of a lesion. Biopsies from the central sclerotic area are likely to be identical irrespective of whether they come from a patient with pseudopélade, discoid lupus erythematosus, or lichen planopilaris. The most important characteristic to bear in mind at the moment of choosing the place to take the biopsy is the presence of inflammation in the scalp. Thus, any area with redness, perifollicular erythema, or scaliness must be preferred over others and submitted for biopsy.20
When pseudopélade is suspected, at least two biopsies should be taken: one for conventional staining for horizontal sections and the other for vertical sections and other studies including direct immunofluorescence, microbiological cultures, and Gram staining.21
The diagnosis is based on the presence of a scarring alopecia in the absence of other features which would allow a more specific diagnosis to be made. Pseudopélade has a very mild or absent mononuclear inflammatory cell infiltrate at the level of the follicular infundibulum and follicular fibrous tracts (Figs 22.150 and 22.151). Interface changes are not observed. The sebaceous glands are reduced or absent.
In the end stage, there is extensive fibrosis and bands of fibrous tissue containing elastic fibers replace the hair follicles. In contrast to the follicular stellae normally present underneath telogen follicles, in pseudopélade these bands of fibrosis extend above and below the insertion of the arrector pili muscle (Fig. 22.152). In spite of the prominent scarring, the arrector pili muscles are resistant to the process and remain until the final stages of the disease (see Fig.22.150 and Fig. 22.152).
disease is more frequent in adult women, there are isolated cases reported in children.11 It has also been described in several families including in two brothers and in a mother and her son.12–15
Pathogenesis and histologic features The precise mechanism whereby hair loss and scarring develop is unknown. Borrelia burgdorferi has been detected within the scarred plaques of a number of patients, suggesting that it may be of etiological importance in at least a subset of cases.16 Specific genes, such as MMP11, TNFSF13B, and APOL2, have been identified with significant differential expression in association with lichen planopilaris and pseudopelade of Brocq, suggesting that they may represent two different diseases and not simply lichen planopilaris in its late phase.17
Direct immunofluorescence is usually negative although occasionally deposits of IgM are found along the basement membrane region.22,23
Differential diagnosis Pseudopélade of Brocq often represents the final phase of a wide range of scarring alopecias. Systematic examination of a biopsy often shows that cases clinically suspected of representing pseudopélade actually represent examples of central centrifugal scarring alopecia, lichen planopilaris, discoid lupus erythematosus, or any other type of alopecia that can lead to prominent scarring.24–26 With an adequate biopsy, clinical correlation, and
1103 Scarring alopecias
The condition is characterized by alopecia localized primarily to the vertex and crown, a chronic and progressive course (which gradually stabilizes), and symmetric expansion with inflammatory activity at the periphery of the lesions.7 The disease is usually asymptomatic. The presence of pruritus may indicate a fungal infection.8
The inflammatory component has variable expression. In some patients, it is mild and only evident after careful inspection. Other patients have a more progressive course with scaling, crusting, intense erythema, and pustules. Such variability may reflect superimposed bacterial infection and differences in the inflammatory reaction to follicular damage.
The condition can present with multiple small, solitary lesions measuring a few centimeters in diameter that gradually become confluent, or it may affect the whole vertex of the scalp. Isolated areas of alopecia show partial or complete loss of hair follicles and the degree of inflammation is variable (Fig. 22.153). In old scarred lesions, polytrichia (tufting) may be a feature.
Central centrifugal scarring alopecia is the most common variant of scarring alopecia in patients of African heritage. The majority of the patients are adult women, and almost all of them have a history of using chemical products to straighten and style their hair.9 It has also been described in men but in this group the use of chemical products is not usually a feature.10 There are no identified cases of central centrifugal cicatricial alopecia in children.11
immunopathological approach, most of these entities can be excluded.27,28 Clinically, pseudopélade of Brocq may also be confused with alopecia areata; nevertheless, the histologic study easily sets aside the latter as inflammatory peribulbar inflammation is seen.29
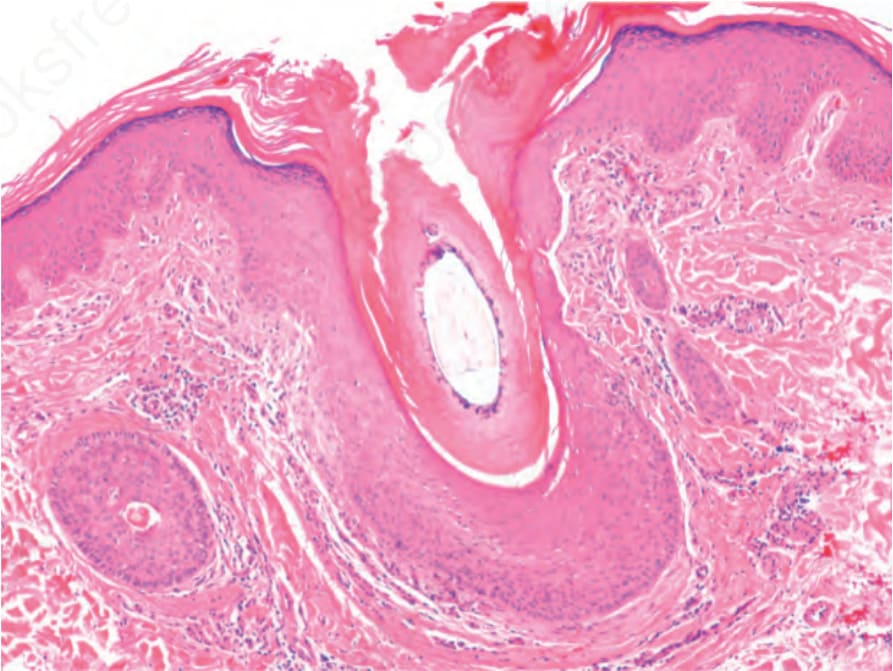
Fig. 22.146 Graham-Little syndrome: dilated infundibulum with hyperkeratosis, mild perifollicular inflammation and fibrosis.
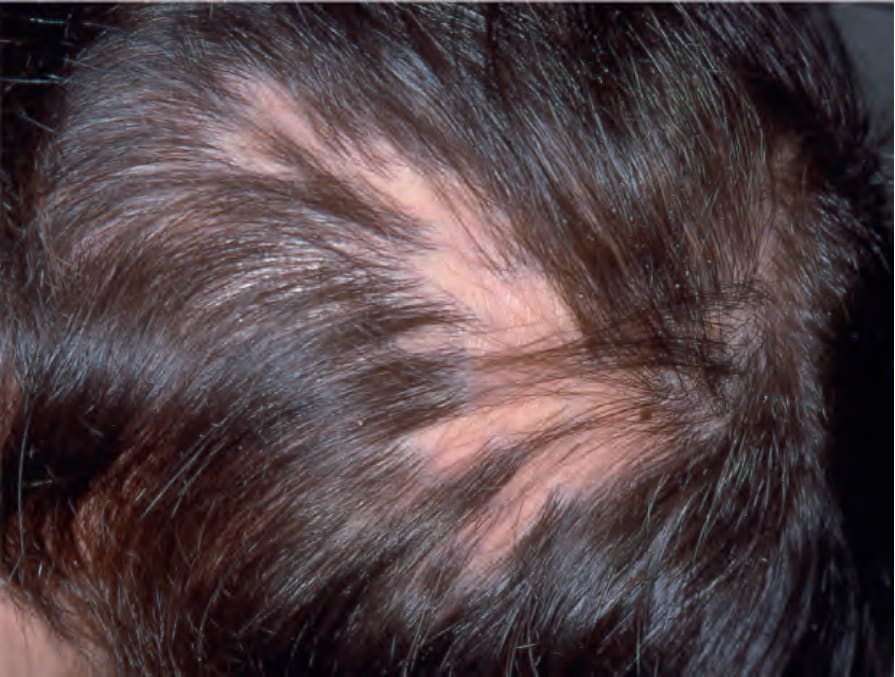
Fig. 22.147 Pseudopélade of Brocq: there are multiple foci of small atrophic patches containing isolated, scattered residual hairs. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.

Fig. 22.148 Pseudopélade of Brocq, late lesion: this example shows the characteristic porcelain-white hypopigmented plaque. Courtesy of A.M. Aristizábal, MD, Instituto de Ciencias de la Salud, Medellín, Colombia.
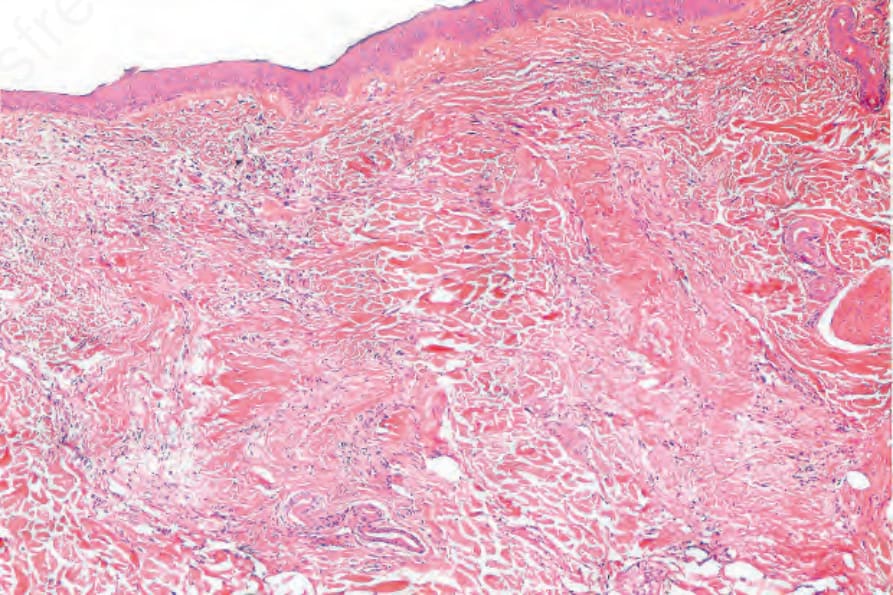
Fig. 22.149 Pseudopélade of Brocq: there is a dense fibrous scar, devoid of an inflammatory cell infiltrate. Two follicular stellae are visible. Note the absence of sebaceous glands.
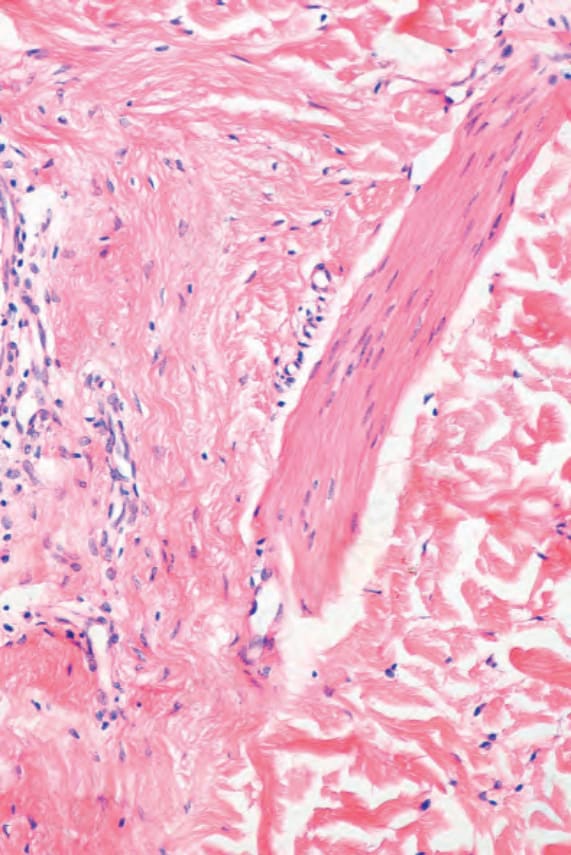
Fig. 22.150 Pseudopélade of Brocq: note the insertion of the arrector pili muscle into a fibrotic scar. There is a sparse inflammatory cell infiltrate.
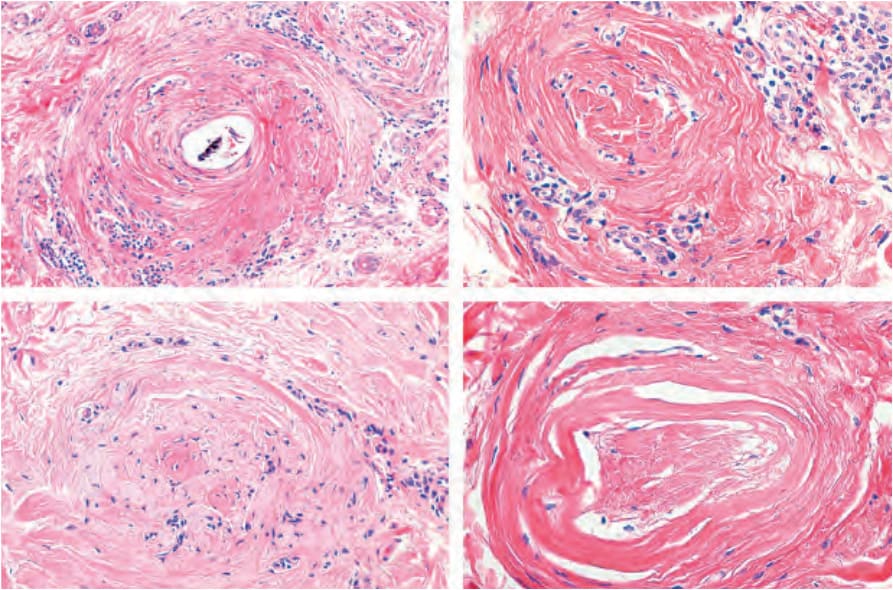
Fig. 22.151 Pseudopélade of Brocq. Follicular scars. In the top right-hand image, a residual lymphocyte inflammatory cell infiltrate is observed.
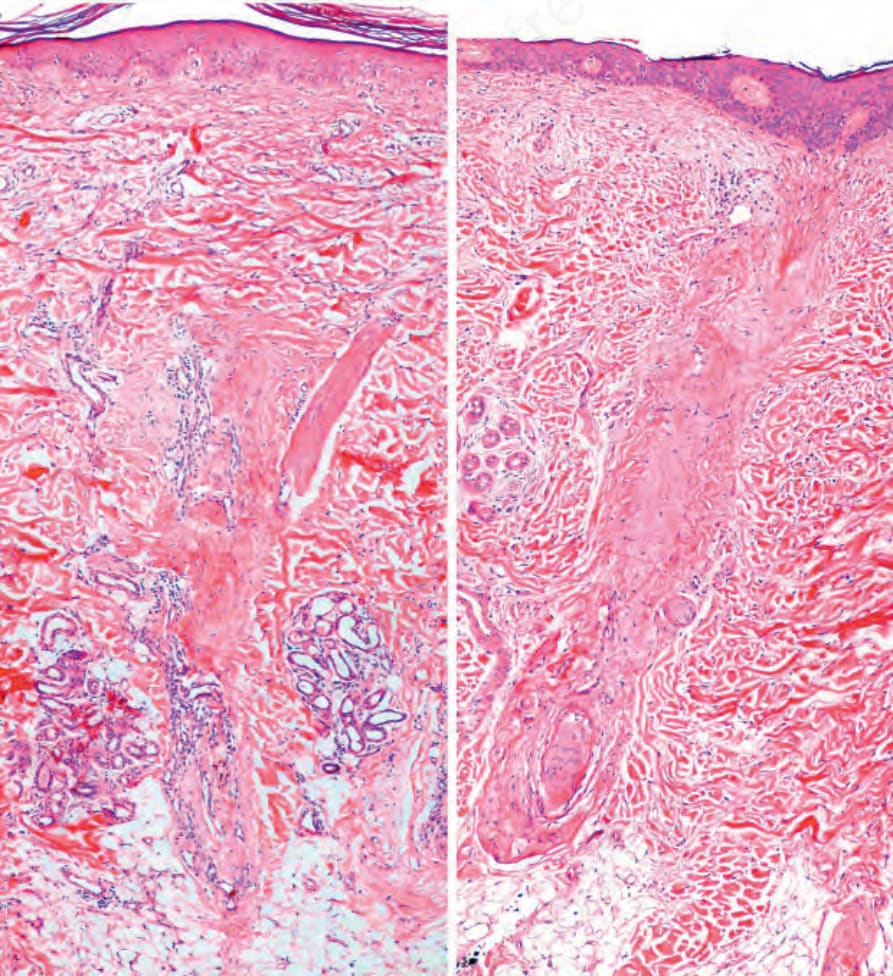
Fig. 22.152 Pseudopélade of Brocq: scarring of the hair follicles extends above and below the insertion of the arrector pili muscle.

Fig. 22.153 Central centrifugal cicatricial alopecia: 40-year-old African woman with a patch of permanent hair loss with centrifuge extension from the vertex. By courtesy of P. Reygagne. Centre Sabouraud. Paris. France.