Syphilitic alopecia
Syphilitic alopecia
Clinical features Syphilitic alopecia is a nonscarring variant of alopecia that has resurfaced in recent years, particularly in association with HIV infection.1–3
The clinical manifestations of syphilitic alopecia were divided into two groups by McCarthy in 1940:
• Symptomatic syphilitic alopecia, which is associated with other manifestations of secondary syphilis, is the rarest form of alopecia. The hair loss may affect the scalp or any other hair-bearing area of the body. It can present in a diffuse or localized pattern (Figs 22.103 and 22.104).
• Essential syphilitic alopecia with no other features of secondary syphilis. This may also be diffuse or localized and represents a variant of latent syphilis.4 Three clinical forms have been described: moth eaten, which is the most frequent and presents usually in the occipital zone, diffuse, which corresponds to telogen effluvium as a reactive phenomenon and a mixed form.5
As the anagen phase is shortened, there is an increase in the number of hair follicles in telogen. Family groupings have been described suggesting an autosomal dominant hereditary pattern.10 Clinically, the hair is normal but there is an increase in the number of hairs obtained in a pull test.
Pathogenesis and histologic features Short anagen syndrome is a form of hair growth defect due to a shortened anagen phase; consequently, there is an increase in the hair follicles that enter telogen phase.1,2,10 The cause of this phenomenon is unknown.
Patients with symptomatic syphilitic alopecia have other manifestations of secondary syphilis and the diagnosis is usually easy. Patients with essential syphilitic alopecia are asymptomatic, and a high degree of suspicion is essential to achieve a correct diagnosis. Alopecia as a manifestation of
1088 Diseases of the hair
secondary or latent syphilis has been reported to occur with an incidence varying between 2.9% and 12.5%.6–9 Therefore, a serological test for syphilis should be considered when there is hair loss for which a satisfactory explanation is not apparent.10
It is important to bear in mind that syphilitic alopecia can involve the whole body and also occasionally present as localized disease at sites away from the scalp.11 Alopecia syphilitica has been described in a neonate with congenital syphilis and in accelerated form as a complication of the Jarisch-Herxheimer reaction.12,13
forms, the patches of alopecia present with a characteristic ‘moth-eaten’ appearance.
The clinical differential diagnosis of syphilitic alopecia is very broad, and the ‘moth-eaten’ alopecia pattern can be confused with trichotillomania, traction alopecia, or alopecia areata. The diffuse variant may be confused with telogen effluvium and a diffuse type of alopecia areata.14,15
The trichogram and the hair-pull test show an increase in the number of telogen hairs in the affected areas.
Histologic features The histologic findings in the lesions of symptomatic syphilitic alopecia are similar to those of secondary syphilis occurring elsewhere. In the papulosquamous lesion, there is psoriasiform hyperplasia of the epidermis, spongiosis and exocytosis of neutrophils, and focal interface change with hydropic degeneration of basal cells. Lymphocytes and plasma cells are present at the dermal–epidermal junction. In the dermis, there is a superficial and deep perivascular and periadnexal lymphohistiocytic inflammatory cell infiltrate with a variable number of plasma cells and occasionally a granulomatous infiltrate in the upper dermis (Fig. 22.105).16
Clinically, symptomatic and essential syphilitic alopecia are very similar and can only be differentiated by the presence of papulosquamous lesions on the scalp or other areas of the body in the symptomatic variant. In both
Essential syphilitic alopecia is characterized by less prominent epidermal changes, reduced anagen hairs, increased telogen and catagen hairs, and a bulbar, peribulbar, and peri-isthmic lymphocytic infiltrate with a variable number of plasma cells. Fibrous tracts may also show lymphocyte infiltration. Identification of Treponema pallidum in sections of tissue in biopsies of patients with syphilitic alopecia yields variable results. Immunohistochemistry is more reliable and sensitive than a silver stain (Fig. 22.105C).14,17–19 Molecular studies with the polymerase chain reaction may also be useful.
Differential diagnosis In essential syphilitic alopecia, the histologic features are very similar to those of alopecia areata. The presence of plasma cells and the tendency of the infiltrate to spare the hair bulb and involve the external root sheath at a higher level without eosinophils are helpful diagnostic pointers.4
Essential syphilis may also present as a telogen effluvium, and distinction between both these conditions on histologic grounds can be impossible, making serological screening for syphilis essential.
B
A
C
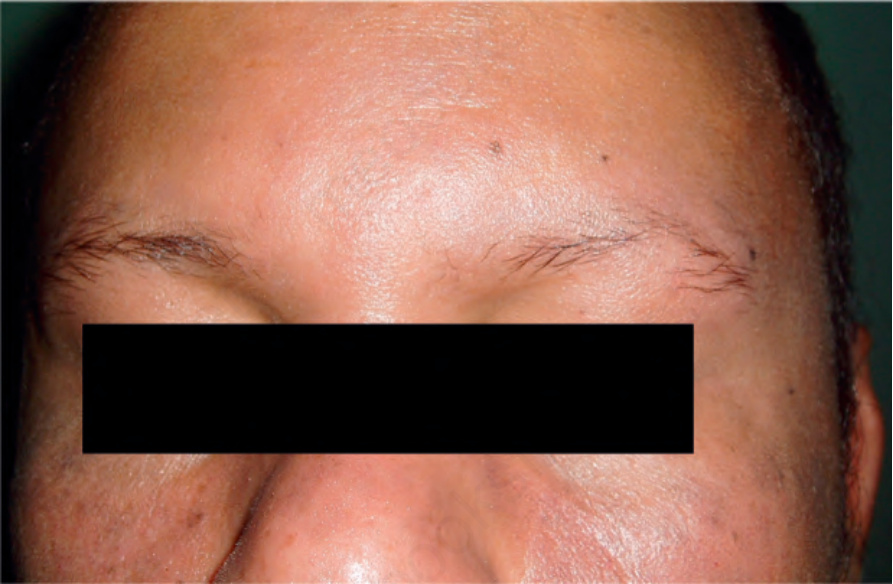
Fig. 22.104 Syphilitic alopecia: loss of eyebrows is not uncommon. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
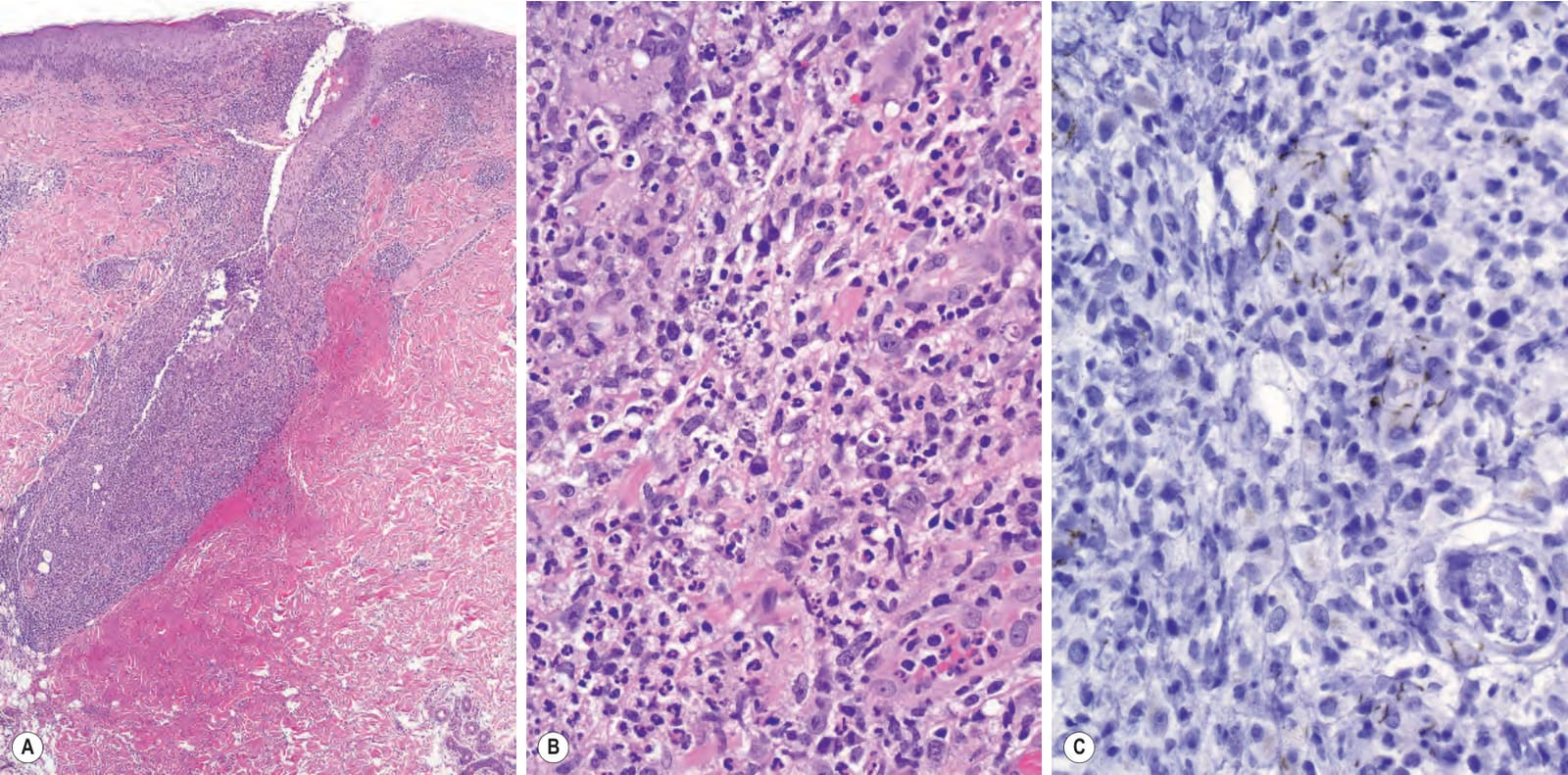
Fig. 22.105 Syphilitic alopecia: (A) there is follicular destruction and an intense inflammatory cell infiltrate; (B) the infiltrate consists of neutrophils, lymphocytes, histiocytes, and plasma cells; (C) numerous spirochetes are present (immunoperoxidase). (The case was kindly supplied by Nooshin Brinster.)